1. Microneedling, also known as collagen induction therapy, is a minimally invasive procedure that uses fine needles to create micro-injuries in the skin, stimulating collagen production.
2. The needles cause controlled skin injuries that release growth factors to induce collagen and elastin formation. New capillaries are also formed, improving skin quality over time.
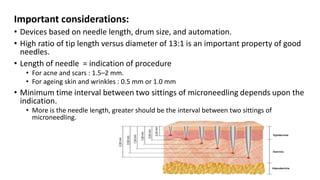
3. Various microneedling devices exist, including dermarollers, dermapens, and fractional radiofrequency microneedling pens, which differ in needle size and arrangement. The optimal device and technique depends on the condition being treated.