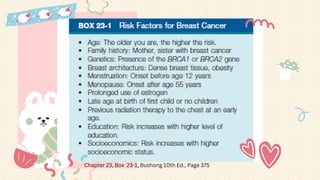
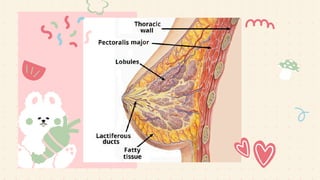
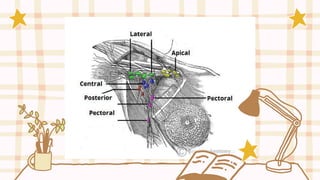
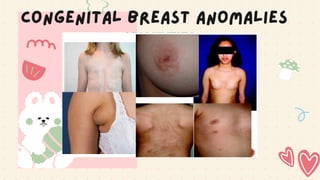
The document discusses breast anatomy and imaging techniques, particularly emphasizing the history and significance of mammography in detecting breast cancer. It highlights the evolution of mammography through various techniques, the effectiveness of early detection in reducing mortality rates, and provides details on breast structure, vasculature, and lymphatic drainage relevant to breast cancer metastasis. The document also mentions congenital breast anomalies and the physiological aspects of the breast related to lactation.