APPLIED ANATOMY AETIOPATHOGENESISCLINICAL
FEATURES INVESTIGATIONS & MANAGEMENT OF
MALIGNANT DISORDERS OF SKIN
(SU.18.2 & 18.3)
Dr Sanjeev R Navalyal
Asst. Prof. Dept. of General Surgery
KLE’S JGMMMC Hubballi
Source
Bailey & Love’s Short Practice of Surgery. 28th
.Edition. Chapter 45. Page 639 to 663
SRB Manual of Surgery. 7th
.Edition. Chapter 19. Page 314 to 335
Schwartz’s Principles of Surgery. 11th
. Edition. Chapter 16.Page 528 to 534
2.
PREMALIGNANT LESIONS OFSKIN
Extramammary Paget’s Disease ( Intraepidermal Adenocarcinoma )
Lesions in sites rich in apocrine glands ( axillae / genital / perianal region )
Giant congenital Pigmented Naevus / Giant Hairy Naevus
Hamartoma of naevo-melanocytes with naevus cells
Giant naevus > 1% of body surface area / > 20 cm in size
3.
HIGH RISK SKINCANCER LESIONS
BCC / SCC has higher risk to develop 2nd
. new skin cancers
> 2 cm in trunk & limbs
> 1cm in forehead & neck
> 6 mm in central face
Poorly defined margins
Recurrent type
Moderate / poor differentiation
Perineural / Vascular invasion
Presence of Immunosuppression
Previous Radio-therapy
4.
ATYPICAL ( DYSPLASTIC) NAEVUS
Three of the following characteristics
Variegated pigmentation
Ill-defined borders
Irregular surfaces
Size > 5 mm
Sporadic / Familial Atypical Multiple Mole–Melanoma ( FAMMM syndrome)
> 5 lesions confers a relative risk of melanoma
FAMMM syndrome confers 100% risk of malignant melanoma
CUTANEOUS SQUAMOUS CELLCARCINOMA / EPITHELIOMA / SCC
DEFINITION
Malignant tumour of keratinising cells of epidermis / its appendages arising from the
stratum basalis of epidermis
PREMALIGNANT CONDITIONS
Bowen’s disease
Paget’s disease
Leukoplakia
Chronic scars
Chemically induced chronic irritation
Radio-dermatitis
Senile keratosis
7.
Cutaneous Squamous CellCarcinoma Contd’
KANG CANCER
Seen in buttocks & heel of Tibetans due to sleeping over oven bed to avoid cold
CHIMNEY SWEEP CANCER
Observed in scrotum due to constant irritation by tar in chimney sweepers
KANGRI CANCER IN KASHMIR
Due to constant placing of hot charcoal pot ( kangri ) over abdominal wall to
avoid cold
8.
Cutaneous Squamous CellCarcinoma Contd’
EPIDEMIOLOGY
Second most common form of skin cancer
Sun exposure & damage in white-skinned living nearer equator
Common in men than women
Associated with chronic inflammation ( chronic sinus tracts / pre-existing scars
Osteomyelitis / burns / vaccination points ) & immunosuppression
9.
KERATOACANTHOMAS
Nodular tumours exhibitingsymmetry around a central keratin-filled crater
Considered as self-healing SCCs
Twice common in men than women
Usually on face / limbs
Chronically seen in sun-damaged 50- to 70-year-old white-skinned individuals
May be caused by HPV infection in hair follicle
Associated with smoking & chemical carcinogen exposure
10.
ACTIN / SOLARKERATITIS WITH CUTANEOUS HORN KERATOCANTHOMA
11.
BOWEN’S DISEASE
SCC insitu with dysplasia in hypertrophic AKs
Slowly enlarging erythematous scaly plaque on mucocutaneous surface
On the glans penis it is called Erythroplasia of Queyrat
COMMON SITES OFSCC
Dorsum of hand
Limbs / Face & Oral cavity
Skin of abdominal wall
External genitalia
Mucocutaneous junction
Respiratory system
Oesophagus
Gall-bladder
Urinary bladder
14.
CLINICAL FEATURES OFSCC
An Ulcerative / Ulceroproliferative / Proliferative lesion
Raised & everted edge
Indurated base & edge
Bloody discharge from lesion
Regional lymph nodes are hard / nodular / initially mobile
Fixed to underlying structures in late stages
Usually blood spread does not occur
15.
VARIANTS OF SCC
MARJOLIN’SULCER
SCC on chronic scar without lymph node spread
FERGUSON - SMITH SYNDROME
Self-healing SCC in face as a familial autosomal dominant ( Ch 9q ) disorder
SCC often associated with BCC
16.
Variants Of SCCContd’
VERRUCOUS CARCINOMA
SITES
Mucous membrane / mucocutaneous junction
FEATURES
Dry / Exophytic / Warty / Indurated growth
No lymph node spread
It has good prognosis
It is a curable malignancy
17.
VERRUCOUS SCC FOOTSCC OF FACE SCC OVER SSG OF SCALP SCC LABIAL SKIN
SCC OVER AMPUTATION STUMP SCAR SCC OF DORSUM OF HAND SCC/ MARJOLIN’S ULCER OVER BURNS
SCAR
18.
INDEPENDENT PROGNOSTIC VARIABLESFOR SCC
DEPTH
For SCC < 2 mm metastasis is highly unlikely
SCC >6 mm, 15% will have metastasised
SURFACE SIZE
Lesions > 2 cm have a worse prognosis than smaller ones
HISTOLOGICAL GRADE
Higher the Broders’ grade the worse the prognosis
19.
Independent Prognostic VariablesFor SCC Contd’
MICROSCOPIC INVASION
Lymphovascular spaces / nerve tissue high risk of metastatic disease
SITE
SCCs on the lips & ears have higher local recurrence rates
AETIOLOGY
Burn scars
Osteomyelitis
Skin sinuses
Chronic ulcers
Irradiated skin
Immunosuppression
20.
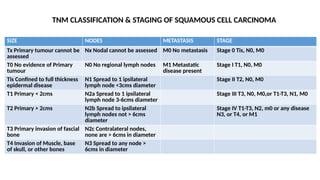
SIZE NODES METASTASISSTAGE
Tx Primary tumour cannot be
assessed
Nx Nodal cannot be assessed M0 No metastasis Stage 0 Tis, N0, M0
T0 No evidence of Primary
tumour
N0 No regional lymph nodes M1 Metastatic
disease present
Stage I T1, N0, M0
Tis Confined to full thickness
epidermal disease
N1 Spread to 1 ipsilateral
lymph node <3cms diameter
Stage II T2, N0, M0
T1 Primary < 2cms N2a Spread to 1 ipsilateral
lymph node 3-6cms diameter
Stage III T3, N0, M0,or T1-T3, N1, M0
T2 Primary > 2cms N2b Spread to ipsilateral
lymph nodes not > 6cms
diameter
Stage IV T1-T3, N2, m0 or any disease
N3, or T4, or M1
T3 Primary invasion of fascial
bone
N2c Contralateral nodes,
none are > 6cms in diameter
T4 Invasion of Muscle, base
of skull, or other bones
N3 Spread to any node >
6cms in diameter
TNM CLASSIFICATION & STAGING OF SQUAMOUS CELL CARCINOMA
21.
Squamous Cell CarcinomaContd’
INVESTIGATIONS
Wedge biopsy from the edge
FNAC from lymph node
USG / CT scan to identify nodal disease
MRI to identify local extension
Squamous Cell CarcinomaContd’
TREATMENT
Wide excision 2 cm clearance
Tumour < 2 cm 4 mm clearance
Tumour > 2 cm 1 cm clearance
Clearance both at margin & depth
Reconstruction by primary split skin grafting (SSG / Thiersch) / Flaps
24.
SCC Treatment Contd’
FORLYMPH NODES
Block dissection
Curative Radiotherapy (RT)
Tumours not adherent to deeper planes / cartilage
Dose of 6000 cGy units over 6 weeks /200 units /day
MARJOLIN’S ULCER (1828)
DEFINITION
Well-differentiated Squamous Cell Carcinoma which occurs in chronic scars like
burn scar / scar of venous ulcer
FEATURES
No lymphatics in scar tissue ( not spread to lymph nodes )
Scar is relatively avascular it grows slowly
As scar does not contain nerves it is painless
It occurs in unstable scar of long duration
27.
Marjolin’s Ulcer Contd’
CLINICALFEATURES
History of pre-existing venous ulcer / burn scar
Indurated / painless / nontender / ulcer with raised & everted edges
Biopsy from the edge confirms the diagnosis
TREATMENT
Wide Excision
In case of large ulcer Amputation is required
Radiotherapy should not be given as it may turn into poorly differentiated SCC
It is a curable malignancy
28.
BASAL CELL CARCINOMA/ BCC ( RODENT ULCER )
DEFINITION
Slow-growing locally invasive malignant tumour of Pluripotential epithelial cells
arising from basal epidermis & hair follicles affecting the pilosebaceous skin
It does not arise from mucosa
EPIDEMIOLOGY
Strongest predisposing factor to BCC is UVR ( ultra violet rays )
Elderly / the middle-aged after excessive sun exposure
95% occurring between the ages of 40 & 80 years
29.
Basal Cell CarcinomaContd’
PREDISPOSING FACTORS
Exposure to arsenical compounds / coal tar / aromatic hydrocarbons
Genetic skin cancer syndromes
White-skinned people are exclusively affected
Common in men than in women
FEATURES
Commonest ( 70%) malignant skin tumour
Common site is face—above the line drawn between angle of mouth & ear
lobule (90%)—Onghren’s line
Called as Tear Cancer as it is seen in area where tears roll down
30.
PATHOGENESIS OF BCC
Noapparent precursor lesions
Development is proportional to the initial dose of the carcinogen
It is only locally malignant
Does not spread through lymphatics / blood
Erodes into local tissues causing extensive local destruction (“rodent ulcer”)
Pathology of BCCContd’
SUPERFICIAL
Multifocal & superfcial spreading
INFILTRATIVE
Morphoeic ice pick & cicatrising
Geographical / Field fire / Forest fire BCC
Wide area of involvement with central scabbing & peripherally active
33.
Pathogenesis of BCCContd’
MICROSCOPY
Twenty-six histological subtypes have been described
Ovoid cells in nests with a single ‘palisading’ layer
Only the outer layer of cells that actively divide
Incompletely excised lesions are more aggressive
Basi - squamous—behaves like squamous cell carcinoma
Nodular & Nodulocystic variants account for 90% of BCCs
34.
CLINICO-PATHOLOGICAL TYPES OFBCC
SUPERFICIAL TYPE
Small buds of tumour masses
MORPHEIC TYPE
Dense stroma with basal cells & type IV collagen
Spreads rapidly ( sclerosing BCC )
FIBROEPITHELIOMA TYPE
Elongated cords of basaloid cells with mesh work
35.
BCC Contd’
CLINICAL FEATURESOF BCC
Ulcer on face in middle-aged man
Nontender / Dry / Slowly growing / Nonmobile / Raised & beaded edge
Central scab & depression / umbilication
No lymph node / blood spread
BCC Contd’
PROGNOSIS
HIGH-RISK BCCS
Tumoursare large ( > 2 cm)
Sites where direct invasion gives access cranium ( near the eye /nose & ear )
Recurrent tumours in presence of immunosuppression
Micronodular / Infiltrating histological subtypes
38.
TREATMENT OF BCC
RADIOTHERAPY(RT )
It is Radiosensitive
Lesion away from vital structure ( eyes ) curative radiotherapy can be given
Radiotherapy is not given if cartilage / bone invasion is present
RT is not given to BCC of ear & close to lacrimal canaliculi
39.
INDICATIONS FOR SURGERYIN BCC
Rodent ulcer eroding into cartilage / bone
BCC close to the eye
Recurrent BCC
WIDE EXCISION
(1 cm clearance) with skin grafting / primary suturing / Z plasty
Rhomboid rotation flap is the procedure of choice
40.
BCC Treatment Contd’
MOHS( MICROSCOPICALLY ORIENTED HISTOGRAPHIC SURGERY )
( Federic E Mohs – American Surgeon )
INDICATIONS
Useful in BCC close to eyes / nose / ear to preserve more tissues
Done by Dermatological surgeon with a Histotechnician / Histologist
41.
MOHS Contd’
PROCEDURE
Saucerised excisionof primary tumour is done
Quadrants of specimen are mapped with different colours
Specimen is sectioned by Histotechnician from margin & depth
Studied by MOHS surgeon / Histologist
Residual tumour from relevant mapped area is excised
Procedure is repeated until clear margin & clear depth are achieved
Cutaneous Malignant MelanomaContd’
EPIDEMIOLOGY
Commonest cancer in young adults (20–39 years)
Occupational & recreational exposure to sunlight Of White skinned individuals
Common in Queensland / Australia / Auckland / New Zealand
PATHOPHYSIOLOGY
Cumulative UVR exposure & ‘flash fry’ exposure
Typical of rapidly acquired holiday tans favours early onset of disease
44.
Cutaneous Malignant MelanomaContd’
HIGH RISK GROUP
Genetic syndromes
> 30 sun-acquired naevi
Five significant sunburns before the age of 20
People living close to Equator
Anyone with Excessive UVR Exposure
45.
Cutaneous Malignant MelanomaContd’
HIGH RISK CONDITIONS
Junctional naevus
Dysplastic naevi
Large Congenital naevi (larger than 20 cm)
Family history of melanoma
Patients on immunosuppressive drugs / after renal transplantation
46.
SITES OF MALIGNANTMELANOMA
Head & neck—25%
Trunk—25%
Lower limb—25%
Upper limb—11%
Other sites—14%
Females leg is the commonest site
Males front / back of trunk
Bantu tribe sole is the commonest site
47.
Sites of MalignantMelanoma Contd’
OTHER SITES
Eyes
Iris / ciliary body / choroids
Mucocutaneous junction
Anorectal region / genitalia
Head & neck
Meninges / oropharynx / nasopharynx / paranasal sinuses
48.
CLASSIFICATIONS OF MALIGNANTMELANOMA
Breslow’s Classification ( 1970 ) Based on Thickness of Invasion
Measured by Optical Micrometer—most important prognostic indicator
I: Less than 0.75 mm
II: Between 0.76 to 1.5 mm
III: 1.51 mm to 4 mm
IV: > 4 mm
49.
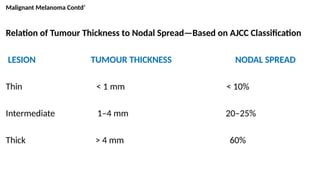
Malignant Melanoma Contd’
Relationof Tumour Thickness to Nodal Spread—Based on AJCC Classification
LESION TUMOUR THICKNESS NODAL SPREAD
Thin < 1 mm < 10%
Intermediate 1–4 mm 20–25%
Thick > 4 mm 60%
50.
CLINICAL TYPES OFMELANOMA
SUPERFICIAL SPREADING MELANOMA / ( SSM )
Most common. 70%.
Occurs in any part of the body with variegated irregular look
It has more radial growth & better prognosis
In men common in back in women in leg
Arises in a pre-existing naevus after years of slow change
Rapid growth in months before presentation
Nodularity heralds onset of vertical growth phase
NODULAR MELANOMA /( NM ) / 12–25%
Common in younger age group
Common in mucosa & mucocutaneous junction
Uniform / nodular / more vertical growth
Nodal spread is common & has poor prognosis
Common in men over trunk / head & neck
More aggressive with shorter clinical onset
Appear as blue / black papules 1–2 cm in diameter & sharply demarcated
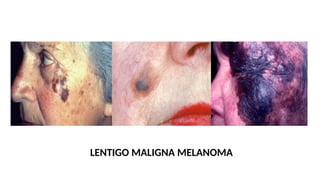
LENTIGO MALIGNA MELANOMA( LMM )
Less common & least malignant
Occurs in old age & common in face ( Hutchinson’s Melanotic Freckle )
Slow growing / variegated / brown macule
Common in face / neck / hands
Affects women > men
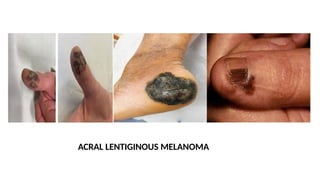
ACRAL LENTIGINOUS MELANOMA( ALM )
Occurs in palms / soles & subungual region
Poor prognosis & least common
Attains large size / nodular type
Common in Africa & Asia
Less common in whites
25% are Amelanotic
May mimic a fungal infection / pyogenic granuloma
AMELANOTIC MELANOMA
Worst type/ Undifferentiation tumour cells loose capacity to produce melanin
Rapidly progressive pinkish fleshy tumour
May mimic soft tissue sarcoma
Needs markers like S100 / HMB45 for diagnosis
May present as metastasis from an unknown skin primary
DESMOPLASTIC MELANOMA
Has highaffinity for perineural invasion
Common in head & neck with higher recurrence rate
SUBUNGUAL MELANOMA
Involvement of nail fold matrix ( not nail plate )
HUTCHINSON’S SIGN
Triangular / Macular / Widening pigmentation of nail fold / Nail dystrophy
Biopsy of nail matrix is indicated
.
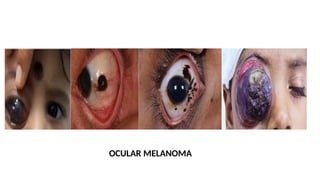
OCULAR MELANOMA
Commonest malignancyarising in eye
Arise from Retina / Iris / Ciliary body / Choroid
Rarely metastasize
Shows its distant spread to liver
Treated with Enucleation / Radiation / Photocoagulation
CLINICAL FEATURES
Induration is not seen
Ulceration / Bleeding / Itching / Change in colour
When a moleturns malignant following changes should be observed
( GLASGOW CRITERIA )
MAJOR SIGNS
Change in size (diameter more than 6 mm) shape & colour
OTHER CHANGES
Inflammation / Crusting / Bleeding / Itching
Nodularity / Ulceration / Halo around a mole
Satellite lesions
Doppler positive pigmented lesions ( > 1 mm thick lesion )
66.
FIVE MOST IMPORTANTFEATURES OF MELANOMA
Asymmetry
Border irregularity
Colour variation
Diameter > 6 mm
Elevation
67.
SPREAD OF MELANOMA
LYMPHATICS
Regionallymph nodes either by permeation / by embolisation
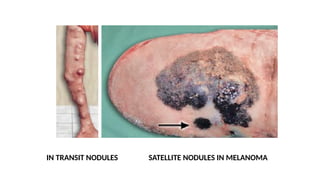
In-transit nodules / satellite nodules
Seen in the skin between the primary lesion & regional lymph node area
HAEMATOGENOUS
To lungs / liver (huge liver) / brain / skin / bones
Secondaries are typically black
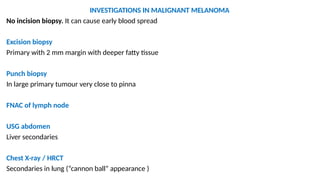
INVESTIGATIONS IN MALIGNANTMELANOMA
No incision biopsy. It can cause early blood spread
Excision biopsy
Primary with 2 mm margin with deeper fatty tissue
Punch biopsy
In large primary tumour very close to pinna
FNAC of lymph node
USG abdomen
Liver secondaries
Chest X-ray / HRCT
Secondaries in lung (“cannon ball” appearance )
71.
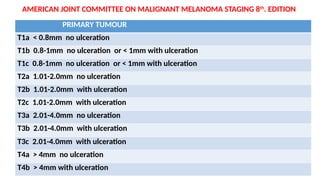
AMERICAN JOINT COMMITTEEON MALIGNANT MELANOMA STAGING 8th
. EDITION
PRIMARY TUMOUR
T1a < 0.8mm no ulceration
T1b 0.8-1mm no ulceration or < 1mm with ulceration
T1c 0.8-1mm no ulceration or < 1mm with ulceration
T2a 1.01-2.0mm no ulceration
T2b 1.01-2.0mm with ulceration
T2c 1.01-2.0mm with ulceration
T3a 2.01-4.0mm no ulceration
T3b 2.01-4.0mm with ulceration
T3c 2.01-4.0mm with ulceration
T4a > 4mm no ulceration
T4b > 4mm with ulceration
72.
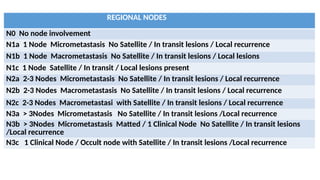
REGIONAL NODES
N0 Nonode involvement
N1a 1 Node Micrometastasis No Satellite / In transit lesions / Local recurrence
N1b 1 Node Macrometastasis No Satellite / In transit lesions / Local lesions
N1c 1 Node Satellite / In transit / Local lesions present
N2a 2-3 Nodes Micrometastasis No Satellite / In transit lesions / Local recurrence
N2b 2-3 Nodes Macrometastasis No Satellite / In transit lesions / Local recurrence
N2c 2-3 Nodes Macrometastasi with Satellite / In transit lesions / Local recurrence
N3a > 3Nodes Micrometastasis No Satellite / In transit lesions /Local recurrence
N3b > 3Nodes Micrometastasis Matted / 1 Clinical Node No Satellite / In transit lesions
/Local recurrence
N3c 1 Clinical Node / Occult node with Satellite / In transit lesions /Local recurrence
73.
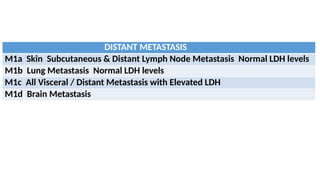
DISTANT METASTASIS
M1a SkinSubcutaneous & Distant Lymph Node Metastasis Normal LDH levels
M1b Lung Metastasis Normal LDH levels
M1c All Visceral / Distant Metastasis with Elevated LDH
M1d Brain Metastasis
74.
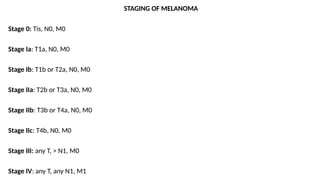
STAGING OF MELANOMA
Stage0: Tis, N0, M0
Stage Ia: T1a, N0, M0
Stage Ib: T1b or T2a, N0, M0
Stage IIa: T2b or T3a, N0, M0
Stage IIb: T3b or T4a, N0, M0
Stage IIc: T4b, N0, M0
Stage III: any T, > N1, M0
Stage IV: any T, any N1, M1
75.
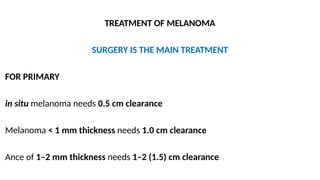
TREATMENT OF MELANOMA
SURGERYIS THE MAIN TREATMENT
FOR PRIMARY
in situ melanoma needs 0.5 cm clearance
Melanoma < 1 mm thickness needs 1.0 cm clearance
Ance of 1–2 mm thickness needs 1–2 (1.5) cm clearance
76.
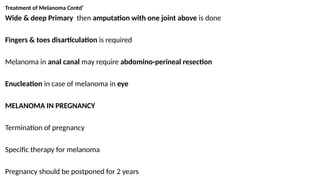
Treatment of MelanomaContd’
Wide & deep Primary then amputation with one joint above is done
Fingers & toes disarticulation is required
Melanoma in anal canal may require abdomino-perineal resection
Enucleation in case of melanoma in eye
MELANOMA IN PREGNANCY
Termination of pregnancy
Specific therapy for melanoma
Pregnancy should be postponed for 2 years
77.
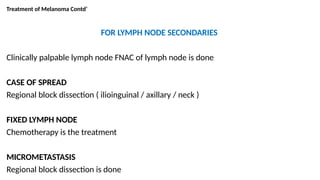
Treatment of MelanomaContd’
FOR LYMPH NODE SECONDARIES
Clinically palpable lymph node FNAC of lymph node is done
CASE OF SPREAD
Regional block dissection ( ilioinguinal / axillary / neck )
FIXED LYMPH NODE
Chemotherapy is the treatment
MICROMETASTASIS
Regional block dissection is done
78.
Treatment of MelanomaContd’
SLNB is useful for melanoma with thickness more than 1 mm depth
Less than 1 mm thickness is considered as low-risk for metastases
1-4 mm thickness is considered as intermediate-risk for metastases
> 4 mm thickness will be considered as high-risk for metastases
Elective lymph node dissection is done when tumour thickness is 1 to 4mm.
79.
Treatment of MelanomaContd’
MANAGEMENT IN UNKNOWN PRIMARY
Nodal radical dissection at the region with adjuvant chemotherapy
FOR LOCO REGIONAL RECURRENT MELANOMA
Local recurrence ( within 5 cm radius of the primary tumour )
ISOLATED LIMB PERFUSION
Cytotoxic agents used
Melphalan
Interleukin 2
Tumour necrosis factor ( TNF )
LASER ABLATION
For multiple small cutaneous lesions
80.
CHEMOTHERAPY FOR MELANOMA
INDICATIONS
Secondariesin lungs / liver / bones
After surgery for melanoma
DRUGS USED
DTIC: Diethyl Triamine Iminocarboxamide
Melphalan
Carboplatin
Vindesine
CVD REGIME— Cisplatin / Vinblastine / Dacarbazine
81.
PROGNOSIS FOR MELANOMA
Poorsince it is very aggressive tumour
Old age has worse prognosis
Females show better prognosis
Extremity melanoma has better prognosis than head & Neck
Higher the mitotic index the poorer the prognosis of primary tumour
Lymph node metastases most important prognostic index in melanoma
Number of nodes & extranodal extension are significant outcome predictors
If nodes are clinically involved 70–85% have occult distant metastases