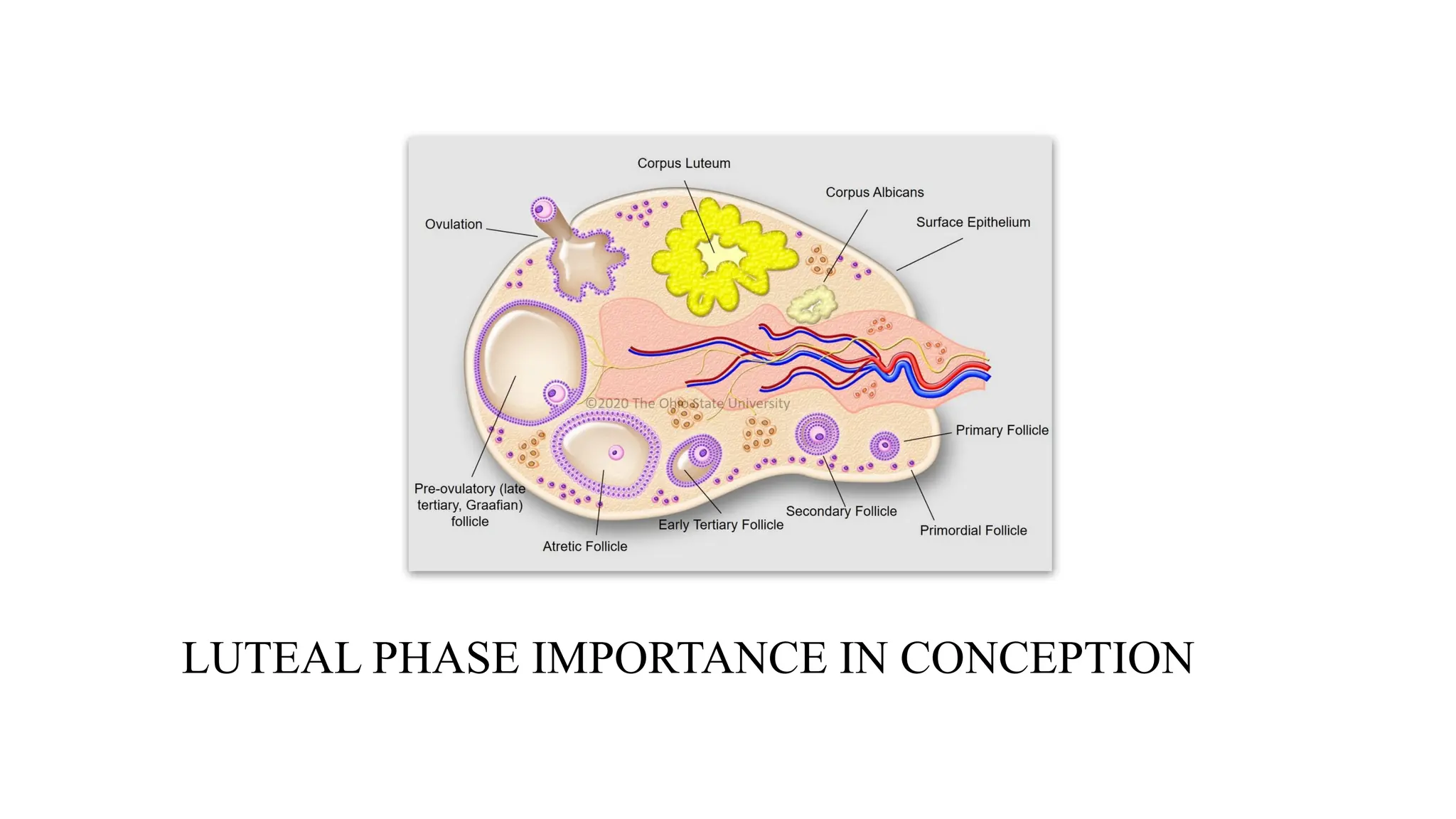
•The luteal phaseis the second part of the menstrual
cycle, occurring after ovulation and before the start of
the next period.
•During this phase, a structure called the corpus luteum
forms and produces progesterone to thicken the uterine
lining, preparing the uterus for a potential pregnancy.
If pregnancy does not occur, hormone levels drop, and
the uterine lining sheds, resulting in menstruation.
6.
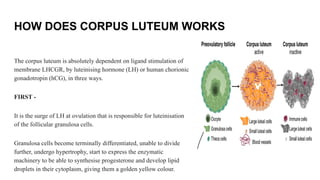
HOW DOES CORPUSLUTEUM WORKS
The corpus luteum is absolutely dependent on ligand stimulation of
membrane LHCGR, by luteinising hormone (LH) or human chorionic
gonadotropin (hCG), in three ways.
FIRST -
It is the surge of LH at ovulation that is responsible for luteinisation
of the follicular granulosa cells.
Granulosa cells become terminally differentiated, unable to divide
further, undergo hypertrophy, start to express the enzymatic
machinery to be able to synthesise progesterone and develop lipid
droplets in their cytoplasm, giving them a golden yellow colour.
7.
SECOND
The second isits maintenance as luteal progesterone
production is absolutely dependent on LHCGR stimulation.
8.
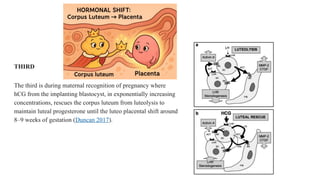
THIRD
The third isduring maternal recognition of pregnancy where
hCG from the implanting blastocyst, in exponentially increasing
concentrations, rescues the corpus luteum from luteolysis to
maintain luteal progesterone until the luteo placental shift around
8–9 weeks of gestation (Duncan 2017).
9.
SHORT LUTEAL PHASE
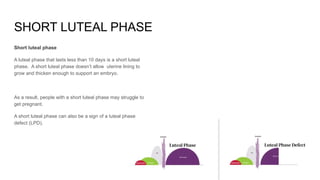
Shortluteal phase
A luteal phase that lasts less than 10 days is a short luteal
phase. A short luteal phase doesn’t allow uterine lining to
grow and thicken enough to support an embryo.
As a result, people with a short luteal phase may struggle to
get pregnant.
A short luteal phase can also be a sign of a luteal phase
defect (LPD).
10.
Long luteal phase
Longluteal phase
A long luteal phase is the opposite of a short luteal
phase. It means period comes 18 days or later after
ovulation.
People with a long luteal phase may have a hormonal
imbalance like PCOS (polycystic ovary syndrome).
11.
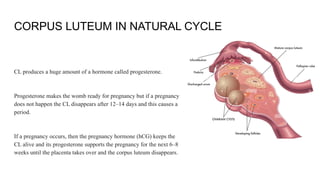
CORPUS LUTEUM INNATURAL CYCLE
CL produces a huge amount of a hormone called progesterone.
Progesterone makes the womb ready for pregnancy but if a pregnancy
does not happen the CL disappears after 12–14 days and this causes a
period.
If a pregnancy occurs, then the pregnancy hormone (hCG) keeps the
CL alive and its progesterone supports the pregnancy for the next 6–8
weeks until the placenta takes over and the corpus luteum disappears.
12.
That means thatif the CL is not working correctly there could be
problems getting pregnant or staying pregnant.
If a CL is not producing enough progesterone it usually means there is
a problem with the growing or releasing of the egg and treatment
should focus on these areas.
In IVF cycles, where normal hormones are switched off, the CL does
not produce quite enough progesterone before the pregnancy test and
extra progesterone is needed at this time.
In recurrent or threatened miscarriage, however, there is not any
evidence that the CL is not working well or progesterone is low.
13.
However, there isbenefit in taking extra progesterone if there
is bleeding in early pregnancy in women with previous
miscarriages.
15.
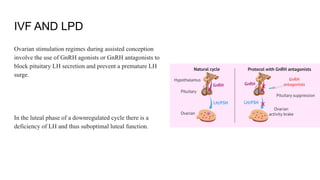
IVF AND LPD
Ovarianstimulation regimes during assisted conception
involve the use of GnRH agonists or GnRH antagonists to
block pituitary LH secretion and prevent a premature LH
surge.
In the luteal phase of a downregulated cycle there is a
deficiency of LH and thus suboptimal luteal function.
16.
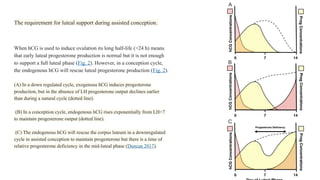
The requirement forluteal support during assisted conception.
When hCG is used to induce ovulation its long half-life (>24 h) means
that early luteal progesterone production is normal but it is not enough
to support a full luteal phase (Fig. 2). However, in a conception cycle,
the endogenous hCG will rescue luteal progesterone production (Fig. 2).
(A) In a down regulated cycle, exogenous hCG induces progesterone
production, but in the absence of LH progesterone output declines earlier
than during a natural cycle (dotted line).
(B) In a conception cycle, endogenous hCG rises exponentially from LH+7
to maintain progesterone output (dotted line).
(C) The endogenous hCG will rescue the corpus luteum in a downregulated
cycle in assisted conception to maintain progesterone but there is a time of
relative progesterone deficiency in the mid-luteal phase (Duncan 2017).
17.
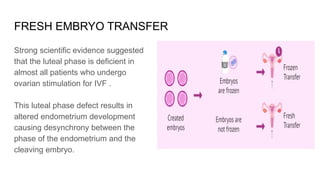
FRESH EMBRYO TRANSFER
Strongscientific evidence suggested
that the luteal phase is deficient in
almost all patients who undergo
ovarian stimulation for IVF .
This luteal phase defect results in
altered endometrium development
causing desynchrony between the
phase of the endometrium and the
cleaving embryo.
18.
As suggested bythe European Society of
Human Reproduction and Embryology (ESHRE)
guidelines,
With regard to the timing of LPS, progesterone
supplementation should be started in the interval
between the evening of the day of oocyte
retrieval and day 3 post oocyte retrieval (19–23)
while starting progesterone before oocyte
retrieval should be discouraged (24)
19.
Hence susten isto be started on day 0 of the cycle that day of oocyte pick up
Better to check p4 before trigger to ensure that Lh surge has not occurred before
20.
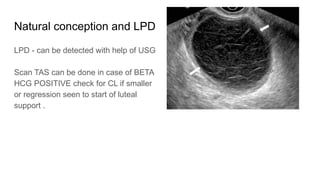
Natural conception andLPD
LPD - can be detected with help of USG
Scan TAS can be done in case of BETA
HCG POSITIVE check for CL if smaller
or regression seen to start of luteal
support .
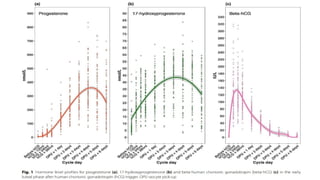
Assessments Blood samples(2 mL each) for analysis of
serum concentrations of progesterone, 17-
hydroxyprogesterone and hCG were collected on the
day of triggering (before hCG), at 12, 24 and 36 h after
hCG administration, and at 1, 2, 3, 4, 5 and 6 days after
oocyte pick-up.
Serum progesterone concentration reflects hormone
secreted by the corpus luteum and exogenous vaginal
progesterone used for luteal phase support,
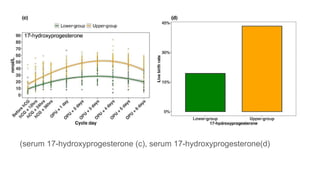
while serum 17-hydroxyprogesterone reflects only
corpus luteum production.
Concentrations of progesterone,
17-hydroxyprogesterone and hCG were determined at
the Clinic.
27.
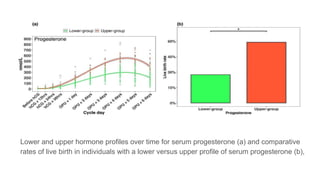
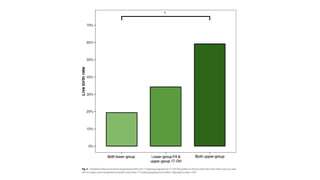
Lower and upperhormone profiles over time for serum progesterone (a) and comparative
rates of live birth in individuals with a lower versus upper profile of serum progesterone (b),
Specialty section: Thisarticle was
submitted to Reproduction, a
section of the journal Frontiers in
Endocrinology Received: 18
January 2020 Accepted: 23 June
2020 Published: 18 August 2020
Citation: Di Guardo F, Midassi H,
Racca A, Tournaye H, De Vos M
and Blockeel C (2020) Luteal
Phase Support in IVF: Comparison
Between Evidence-Based
Medicine and Real-Life Practices.
Front. Endocrinol. 11:500. doi:
10.3389/fendo.2020.00500