Downloaded 10 times

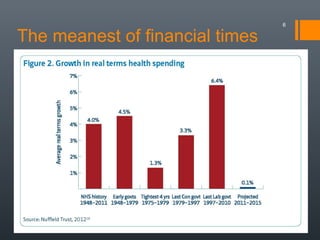




The document discusses the evolution of England's NHS since 1999, highlighting the diverging healthcare systems among the UK nations and the shift towards market-style reforms in England. Key points include increased funding and staffing during the Labour government, followed by austerity measures under the Tory coalition, leading to cuts, closures, and pressures on emergency services. The future of the NHS is questioned, particularly concerning potential privatization and the imposition of charges for certain services.












































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











