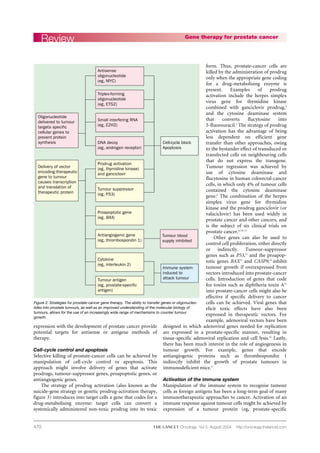
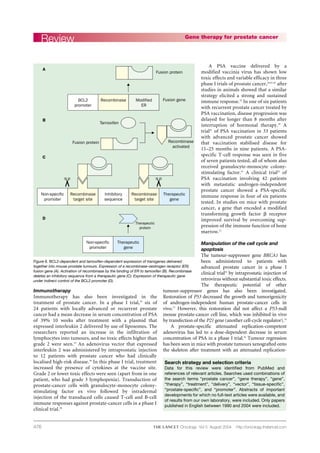
This document discusses gene therapy approaches for prostate cancer that have been investigated. It outlines several strategies, including delivering genes to induce cell death or inhibit cell growth, activate the immune system against tumor cells, and target specific gene expression. Clinical trials are evaluating therapies using the herpes simplex virus gene with ganciclovir to activate a prodrug, as well as other approaches to manipulate cell proliferation, apoptosis, angiogenesis, and the immune response. Tissue-specific delivery and regulation of gene expression offer promise for gene therapy in prostate cancer.