Downloaded 11 times

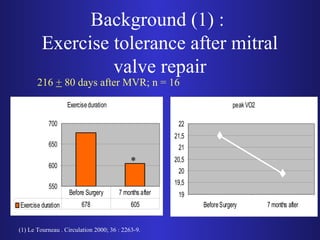
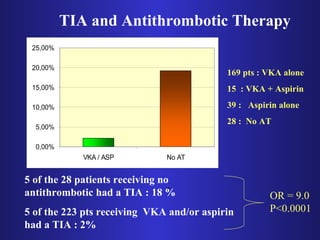
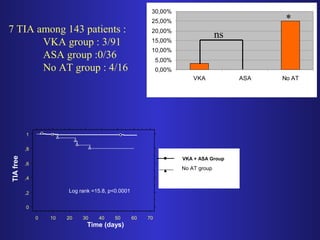

The document discusses cardiac rehabilitation after mitral valve repair, highlighting the importance of exercise training which improves exercise tolerance while addressing concerns about potential damage to the repair. It reviews the necessity of antithrombotic therapy post-surgery and provides evidence that such therapy is essential for at least the first six weeks. The findings support early rehabilitation as safe and beneficial in improving patient outcomes without increasing complications.























































































