Download to read offline
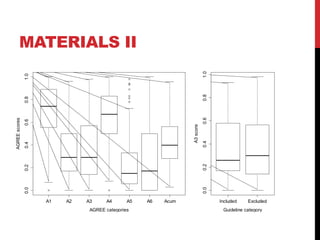
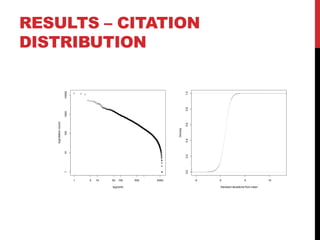
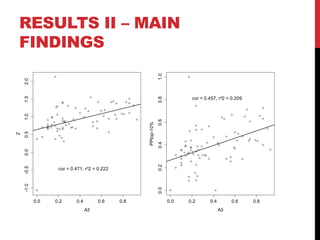
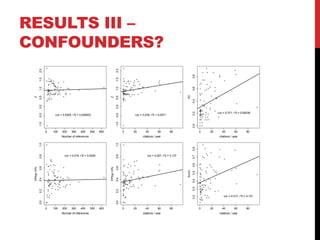

The document investigates the relationship between the quality of clinical practice guidelines (CPGs) and the citations of their references, focusing on the 'rigour of development' aspect assessed via the AGREE instrument. The study found a medium-strength correlation between the A3 scores of CPGs and the citation counts of their references, without significant confounding factors. However, it concludes that more data is needed to understand potential connections between citation metrics, clinical evidence, and health impacts.















































