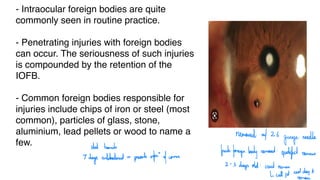
- Intraocular foreignbodies are quite
commonly seen in routine practice.
- Penetrating injuries with foreign bodies
can occur. The seriousness of such injuries
is compounded by the retention of the
IOFB.
- Common foreign bodies responsible for
injuries include chips of iron or steel (most
common), particles of glass, stone,
aluminium, lead pellets or wood to name a
few.
removed at 26
gauge
needle
stat homich
I
days antibacteria -
prevents infer" of comea
fresh foreign
body remoud:
epidefectremain
2 -
3
days old: crust
remain
I call pt.
nextday
remove
3.
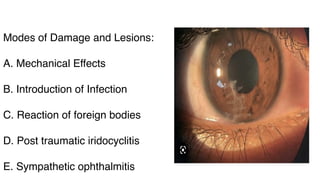
Modes of Damageand Lesions:
A. Mechanical Effects
B. Introduction of Infection
C. Reaction of foreign bodies
D. Post traumatic iridocyclitis
E. Sympathetic ophthalmitis
4.
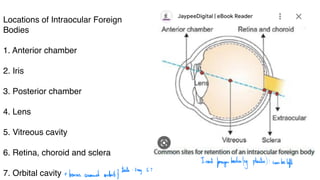
Locations of IntraocularForeign
Bodies
1. Anterior chamber
2. Iris
3. Posterior chamber
4. Lens
5. Vitreous cavity
6. Retina, choroid and sclera
7. Orbital cavity
Inert
foreign
bodies
leg plastic): can be
left
-bones around artery
tests:Xray, CT
5.
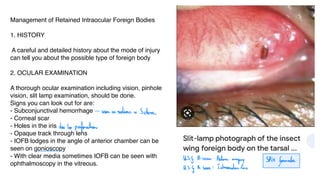
Management of RetainedIntraocular Foreign Bodies
1. HISTORY
A careful and detailed history about the mode of injury
can tell you about the possible type of foreign body
2. OCULAR EXAMINATION
A thorough ocular examination including vision, pinhole
vision, slit lamp examination, should be done.
Signs you can look out for are:
- Subconjunctival hemorrhage
- Corneal scar
- Holes in the iris
- Opaque track through lens
- IOFB lodges in the angle of anterior chamber can be
seen on gonioscopy
- With clear media sometimes IOFB can be seen with
ophthalmoscopy in the vitreous.
seen as redness in Schere
due to perforation
ISG B scow: Retina
imaging SRK
faumda
US
I A scan: IntraocularLens
6.
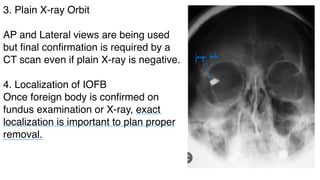
3. Plain X-rayOrbit
AP and Lateral views are being used
but final confirmation is required by a
CT scan even if plain X-ray is negative.
4. Localization of IOFB
Once foreign body is confirmed on
fundus examination or X-ray, exact
localization is important to plan proper
removal.
foreign
body
- - -
7.
1. Radiographic localization
a.Limbal ring technique- This technique is now
obsolete. A metallic ring of corneal diameter is stitched
to the limbus. AP and lateral views are taken along with
3 exposures of patient looking straight, upwards and
downwards. The position of the foreign body is
estimated from its relationship with the metallic ring in
different positions.
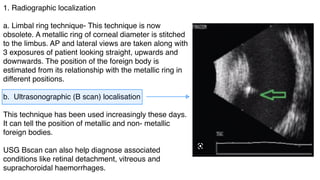
b. Ultrasonographic (B scan) localisation
This technique has been used increasingly these days.
It can tell the position of metallic and non- metallic
foreign bodies.
USG Bscan can also help diagnose associated
conditions like retinal detachment, vitreous and
suprachoroidal haemorrhages.
8.
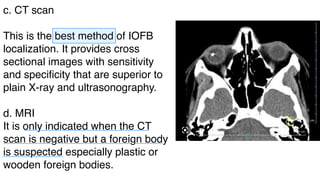
c. CT scan
Thisis the best method of IOFB
localization. It provides cross
sectional images with sensitivity
and specificity that are superior to
plain X-ray and ultrasonography.
d. MRI
It is only indicated when the CT
scan is negative but a foreign body
is suspected especially plastic or
wooden foreign bodies.
-
-
-
9.
Removal of foreignbodies
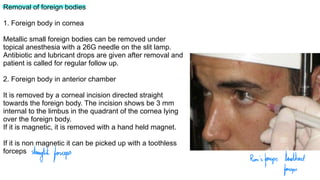
1. Foreign body in cornea
Metallic small foreign bodies can be removed under
topical anesthesia with a 26G needle on the slit lamp.
Antibiotic and lubricant drops are given after removal and
patient is called for regular follow up.
2. Foreign body in anterior chamber
It is removed by a corneal incision directed straight
towards the foreign body. The incision shows be 3 mm
internal to the limbus in the quadrant of the cornea lying
over the foreign body.
If it is magnetic, it is removed with a hand held magnet.
If it is non magnetic it can be picked up with a toothless
forceps
straight forceps Rim's
forceps:toothed
forceps
10.
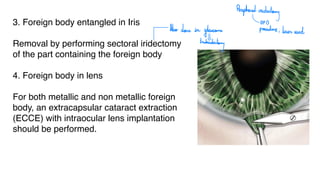
3. Foreign bodyentangled in Iris
Removal by performing sectoral iridectomy
of the part containing the foreign body
4. Foreign body in lens
For both metallic and non metallic foreign
body, an extracapsular cataract extraction
(ECCE) with intraocular lens implantation
should be performed.
Peripheral
iridectomy
OPB
Also done in
glaucoman procedie; laser used
trabeculectory
11.
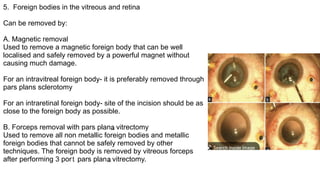
5. Foreign bodiesin the vitreous and retina
Can be removed by:
A. Magnetic removal
Used to remove a magnetic foreign body that can be well
localised and safely removed by a powerful magnet without
causing much damage.
For an intravitreal foreign body- it is preferably removed through
pars plans sclerotomy
For an intraretinal foreign body- site of the incision should be as
close to the foreign body as possible.
B. Forceps removal with pars plans vitrectomy
Used to remove all non metallic foreign bodies and metallic
foreign bodies that cannot be safely removed by other
techniques. The foreign body is removed by vitreous forceps
after performing 3 pore pars plans vitrectomy.
N
M N