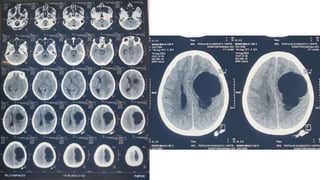
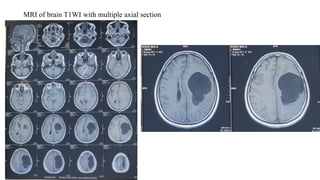
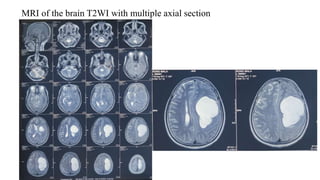
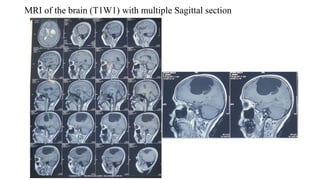
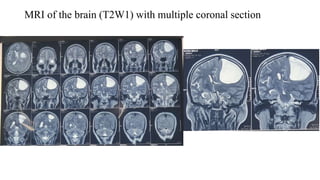
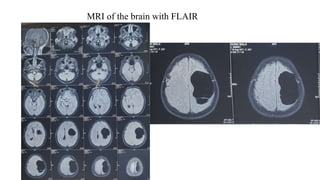
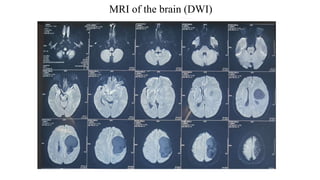
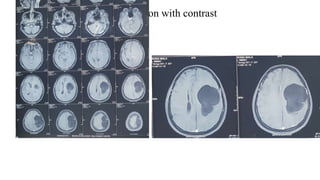
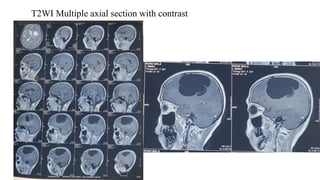
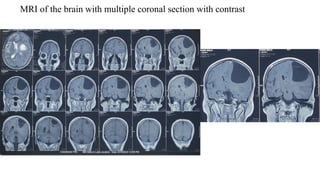
Mrs. Rangmala, a 52-year-old housewife, presented with 11 months of right-sided weakness and headache, as well as recent difficulty speaking and urinary incontinence. MRI revealed a left frontoparietal arachnoid cyst. The surgical plan is a left fronto-temporal craniotomy and marsupialization of the cyst to relieve pressure and symptoms. Risks include bleeding, neurological injury, seizures, CSF leakage, and infection.