


















![References
1. Sharma N. The International Health Partnership (IHP) and Related
Initiatives (IHP+)and Nepal’s Experience. [Presentation]. 2009.
2. International Health Partnership official webpage
http://www.internationalhealthpartnership.net/
3. Paris Declaration on Aid Effectiveness, 2007
4. IHP + Strategic Directions 2016-17
5. Nepal Health Development Partnership. Kathmandu: Government
of Nepal; 2009.
6. Progress in the International Health Partnership & Related
Initiatives (IHP+). 2014.
7. Holzcheiter A. The Handbook of Transnational Governance:
Institutions and Innovations. UK: Polity Press; 2012.
22](https://image.slidesharecdn.com/internationalhealth-ihp-170905115952/75/International-Health-Partnership-22-2048.jpg)

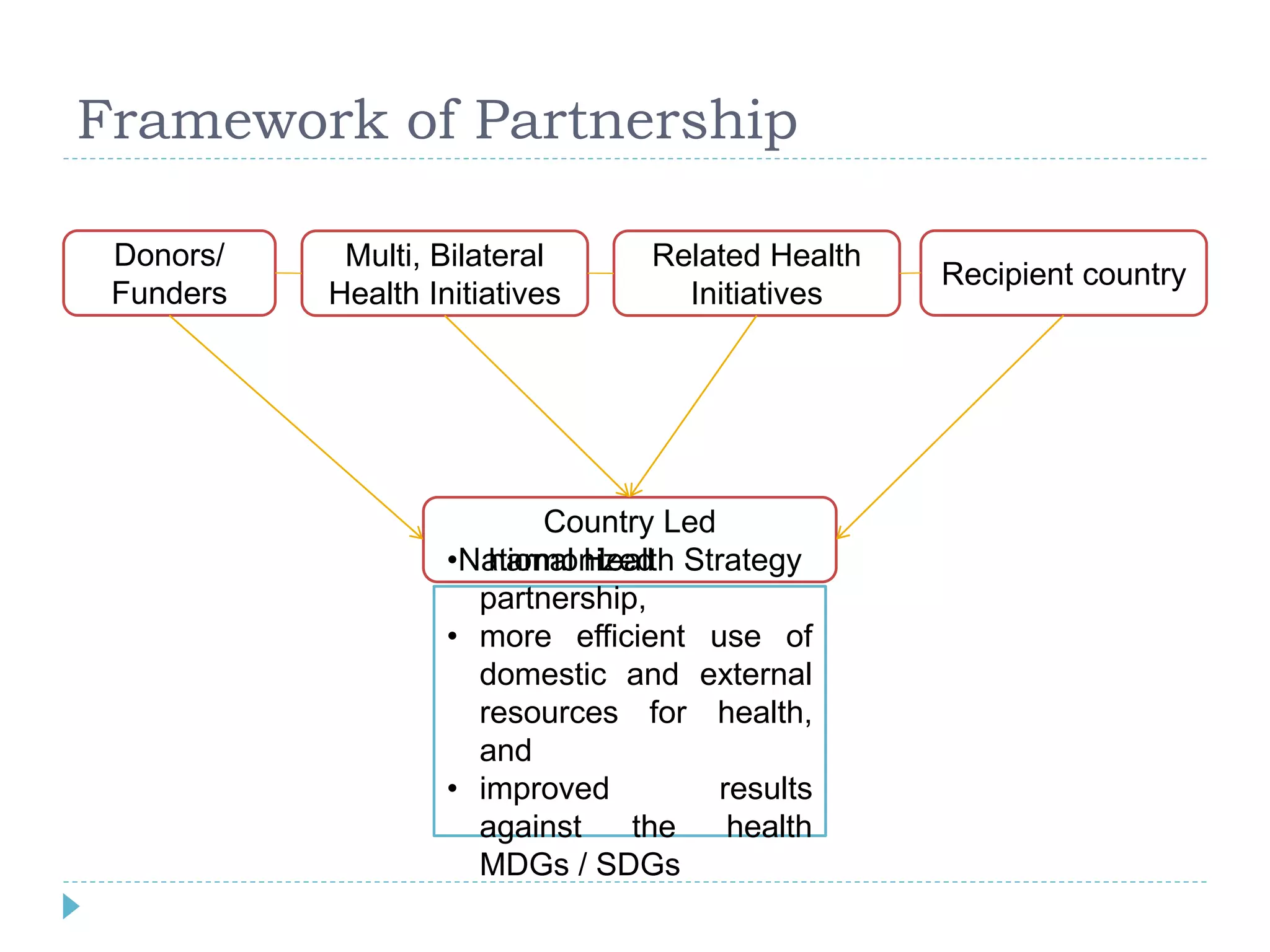
Prabesh Ghimire presented on the International Health Partnership (IHP). The IHP was launched in 2007 to help coordinate global health initiatives and improve health systems in developing countries. It aims to support country-led health plans, jointly assess strategies, negotiate funding agreements, and increase accountability. The IHP has grown to include 66 partner organizations and 37 countries. Country compacts outline commitments between governments and donors to align funding with national health priorities. Studies show countries engaged with IHP have seen positive results, including increased health funding and coverage. Nepal was an early adopter of IHP principles through its own health partnership compact.

































![GROUP_4677577675567856788_FINAL_(1)[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/group4final11-250928095912-6ec9da71-thumbnail.jpg?width=640&height=640&fit=bounds)





















































