Improving the Recognition and Management of Migraine in an Era of Expanding Options for Acute Treatment and Prevention: How Is the Role of the Primary Care Clinician Evolving?
•
1 like•120 views

Deborah I. Friedman, MD, MPH, prepared useful Practice Aids pertaining to migraine management for this CME activity titled "Improving the Recognition and Management of Migraine in an Era of Expanding Options for Acute Treatment and Prevention: How Is the Role of the Primary Care Clinician Evolving?" For the full presentation, monograph, complete CME information, and to apply for credit, please visit us at http://bit.ly/2qQuwAt. CME credit will be available until November 22, 2019.

Recommended
Recommended
More Related Content
Similar to Improving the Recognition and Management of Migraine in an Era of Expanding Options for Acute Treatment and Prevention: How Is the Role of the Primary Care Clinician Evolving?
Similar to Improving the Recognition and Management of Migraine in an Era of Expanding Options for Acute Treatment and Prevention: How Is the Role of the Primary Care Clinician Evolving? (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Improving the Recognition and Management of Migraine in an Era of Expanding Options for Acute Treatment and Prevention: How Is the Role of the Primary Care Clinician Evolving?
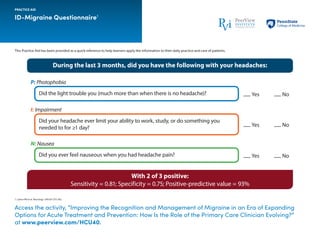
- 1. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. ID-Migraine Questionnaire1 1. Lipton RB et al. Neurology. 2003;61:375-382. PRACTICE AID Access the activity, “Improving the Recognition and Management of Migraine in an Era of Expanding Options for Acute Treatment and Prevention: How Is the Role of the Primary Care Clinician Evolving?” at www.peerview.com/HCU40. With 2 of 3 positive: Sensitivity = 0.81; Specificity = 0.75; Positive-predictive value = 93% During the last 3 months, did you have the following with your headaches: Did the light trouble you (much more than when there is no headache)?Did the light trouble you (much more than when there is no headache)? Yes No P: Photophobia Did your headache ever limit your ability to work, study, or do something you needed to for ≥1 day? Yes No I: Impairment Did you ever feel nauseous when you had headache pain? Yes No N: Nausea
- 2. Access the activity, “Improving the Recognition and Management of Migraine in an Era of Expanding Options for Acute Treatment and Prevention: How Is the Role of the Primary Care Clinician Evolving?” at www.peerview.com/HCU40. Selected Emerging Therapies for the Acute Treatment of Migraine This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. CGRP: calcitonin gene-related peptide receptor antagonist. 1. Wietecha LA et al. American Academy of Neurology 2018 Annual Meeting (AAN 2018). Abstract S50.008. 2. Lipton RB et al. American Headache Society 60th Annual Scientific Meeting (AHS 2018). Poster PS123LB. 3. Lipton RB et al. AHS 2018. Poster IOR-02LB. 4. Trugman J et al. AAN 2018. Emerging Science Abstract 008. 5. Silberstein S et al. AHS 2018. Poster PS111B. PRACTICE AID Therapy MOA Current Status Lasmiditan1 Centrally acting serotonin (5-HT1F ) agonist • Two positive phase 3, randomized, placebo-controlled trials • Most frequently reported AEs after first dose: dizziness, paresthesia, somnolence, fatigue, nausea, and lethargy Rimegepant2,3 CGRP receptor antagonist • Two positive phase 3, randomized, placebo-controlled trials • Most frequently reported AEs included nausea and UTI Ubrogepant4,5 CGRP receptor antagonist • Two positive phase 3, randomized, placebo-controlled trials • Most frequently reported AEs within 48 h of dosing: nausea, somnolence, and dry mouth
- 3. This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. Approved and Emerging Anti-CGRP Monoclonal Antibodies for Migraine Prevention CGRP: calcitonin gene-related peptide receptor antagonist. 1. Aimovig (erenumab-aooe) Prescribing Information. https://pi.amgen.com/~/media/amgen/repositorysites/pi-amgen-com/Aimovig/Aimovig_pi_hcp_english.pdf. Accessed October 24, 2018. 2. Ajovy (fremanezumab-vfrm) Prescribing Information. https://www.ajovyhcp.com/ globalassets/ajovy/ajovy-pi.pdf. Accessed October 24, 2018. 3. Emgality (galcanezumab-gnlm) Prescribing Information. http://pi.lilly.com/us/emgality-uspi.pdf. Accessed October 24, 2018. 4. Saper R et al. American Academy of Neurology 2018 Annual Meeting (AAN 2018). Abstract S20.001. 5. Kudrow DB et al. AAN 2018. Abstract P4.470. PRACTICE AID Access the activity, “Improving the Recognition and Management of Migraine in an Era of Expanding Options for Acute Treatment and Prevention: How Is the Role of the Primary Care Clinician Evolving?” at www.peerview.com/HCU40. Monoclonal Antibody Antibody Type Directed Against Indication Recommended Dosage Approved Erenumab-aooe1 Fully human CGRP receptor Preventive treatment of migraine in adults • 70 mg subQ, once monthly • Some patients may benefit from 140 mg subQ, once monthly (administered as two consecutive injections of 70 mg) Fremanezumab-fvrm2 Humanized CGRP ligand Preventive treatment of migraine in adults • 225 mg subQ, once monthly or • 675 mg subQ, every 3 months (administered as three consecutive injections of 225 mg) Galcanezumab-gnlm3 Humanized CGRP ligand Preventive treatment of migraine in adults • 240 mg subQ loading dose (administered as two consecutive injections of 120 mg), followed by monthly doses of 120 mg Emerging Eptinezumab4,5 Humanized CGRP ligand Positive data from phase 3 migraine prevention trials have been reported