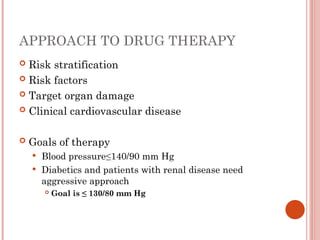
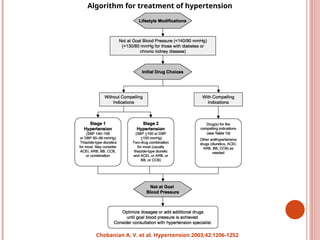
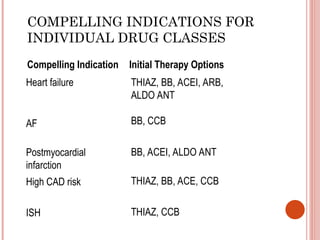
The document provides a comprehensive overview of hypertension, defining its types, causes, and the risk factors associated with it. It discusses the evaluation, classification, and management strategies for hypertension, including the importance of proper blood pressure measurement and treatment approaches tailored to individual patient profiles. Additionally, the document highlights hypertensive urgency and emergencies, emphasizing the need for timely intervention and appropriate therapy to manage associated target-organ damage.


































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















