Hyperphosphatemia
•
0 likes•3,491 views

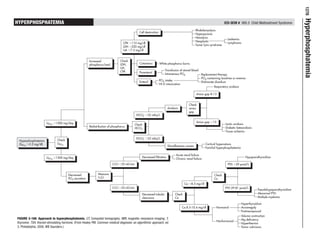
Hyperphosphatemia is a condition characterized by abnormally high levels of phosphorus in the blood. The document provides an algorithmic approach for evaluating and treating hyperphosphatemia. It outlines potential causes of hyperphosphatemia including increased phosphorus intake, decreased renal excretion or filtration, and redistribution of phosphorus from bones and cells. Laboratory tests that should be checked include levels of calcium, parathyroid hormone, bicarbonate, and creatinine clearance. Treatment depends on the underlying cause but may involve restricting phosphorus intake, using phosphate-binding medications, or treating any acidosis or kidney problems present.

More Related Content
Viewers also liked
Viewers also liked (11)
Recently uploaded
Recently uploaded (20)
Hyperphosphatemia
- 1. 1278 Hyperphosphatemia HYPERPHOSPHATEMIA ICD-9CM # 995.5 Child Maltreatment Syndrome Rhabdomyolysis Cell destruction Hyperpyrexia Hemolysis Leukemia Neoplastic CPK Ͼ110 mg/dl Lymphoma Tumor lysis syndrome LDH Ͼ220 mg/dl UA Ͼ7.5 mg/dl Increased Check phosphorus load LDH, Cutaneous White phosphorus burns UA, CPK Transfusion of stored blood Parenteral Intravenous PO4 Replacement therapy PO4-containing laxatives or enemas Enteral PO4 intake Etidronate disodium Vit D intoxication Respiratory acidosis Anion gap 8-13 Check Acidosis anion gap HCOϪ Ͻ22 mEq/L 3 UPO4 Ͼ1500 mg/day Anion gap Ͼ13 Check Lactic acidosis Redistribution of phosphorus Diabetic ketoacidosis HCOϪ3 Tissue ischemia HCOϪ Ͼ22 mEq/L 3 Hyperphosphatemia Check (SPO4 Ͼ5.2 mg/dl) UPO4 Cortical hyperostosis Miscellaneous causes Familial hyperphosphatemia Acute renal failure UPO4 Ͻ1500 mg/day Decreased filtration Hypoparathyroidism Chronic renal failure CrCI Ͻ25 ml/min PTH Ͻ29 pmol/L Decreased Measure Check PO4 excretion CrCI Ca Ca Ͻ8.5 mg/dl CrCI Ͼ25 ml/min PTH 29-81 pmol/L Pseudohypoparathyroidism Decreased tubular Check Abnormal PTH clearance Ca Multiple myeloma Hyperthyroidism Ca 8.5-10.4 mg/dl Hormonal Acromegaly Postmenopausal Volume contraction FIGURE 3-166 pproach to hyperphosphatemia. CT, Computed tomography; MRI, magnetic resonance imaging; T, A Mg deficiency Nonhormonal thyroxine; TSH, thyroid-stimulating hormone. (From Healey PM: Common medical diagnosis: an algorithmic approach, ed Hyperthermia 3, Philadelphia, 2000, WB Saunders.) Tumor calcinosis