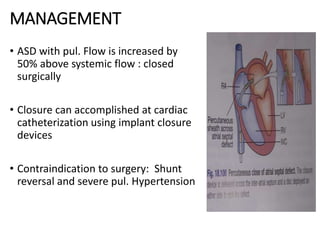
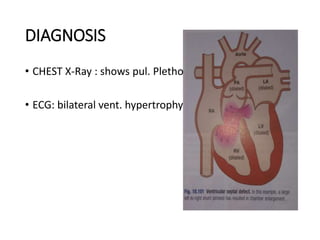
This document discusses several types of congenital heart diseases including their etiology, pathophysiology, clinical manifestations, diagnostic evaluation, and management. It covers tetralogy of fallot, persistent ductus arteriosus, atrial septal defect, and ventricular septal defect. For each condition, it provides details on the anatomical defects involved, characteristic signs and symptoms, relevant test findings, and treatment options including surgical repair when indicated.