Heart failure(HF) is a clinical syndrome caused by the inability of the heart to pump sufficient blood
to meet the metabolic needs of the body.
HF can result from any disorder that reduces ventricular filling (diastolic dysfunction) and/or
myocardial contractility (systolic dysfunction)
4.
PTHOPHYSIOLOGY
Causes ofsystolic dysfunction (decreased contractility) are
Reduction in muscle mass (e.g., myocardial infarction [MI]),
Dilated cardiomyopathies, and
Ventricular hypertrophy.
Ventricular hypertrophy can be caused by pressure overload (e.g., systemic or pulmonary hypertension, aortic or
pulmonic valve stenosis) or volume overload (e.g., valvular regurgitation, shunts, high-output states)
5.
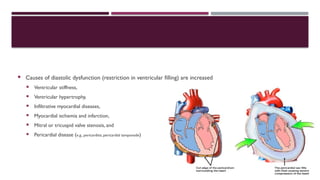
Causes ofdiastolic dysfunction (restriction in ventricular filling) are increased
Ventricular stiffness,
Ventricular hypertrophy,
Infiltrative myocardial diseases,
Myocardial ischemia and infarction,
Mitral or tricuspid valve stenosis, and
Pericardial disease (e.g., pericarditis, pericardial tamponade)
6.
The leadingcauses of HF are coronary artery disease and hypertension
As cardiac function decreases after myocardial injury, the heart relies on the following compensatory mechanisms:
tachycardia and increased contractility through sympathetic nervous system activation;
the Frank-Starling mechanism, whereby increased preload increases stroke volume;
Vasoconstriction; and
Ventricular hypertrophy and remodeling.
Although these compensatory mechanisms initially maintain cardiac function, they are responsible for the
symptoms of HF and contribute to disease progression
7.
The neurohormonalmodel of HF recognizes that an initiating event (e.g., acute MI) leads to decreased cardiac
output but that the HF state then becomes a systemic disease whose progression is mediated largely by
neurohormones and autocrine/paracrine factors.
These substances include angiotensin II, norepinephrine, aldosterone, natriuretic peptides, arginine vasopressin,
proinflammatory cytokines (e.g., tumor necrosis factor ,
α interleukin-6 and interleukin-1 ),
β and endothelin-1
Common precipitating factors that may cause a previously compensated patient to decompensate include
noncompliance with diet or drug therapy, coronary ischemia, inappropriate medication use, cardiac events (e.g.,
MI, atrial fibrillation), pulmonary infections, and anemia
8.
Drugsmay precipitate orexacerbate HF because of their negative inotropic, cardiotoxic, or sodium- and
water-retaining properties
9.
CLINICAL PRESENTATION
Thepatient presentation may range from asymptomatic to cardiogenic shock.
The primary symptoms are dyspnea (particularly on exertion) and fatigue, which lead to exercise intolerance.
Other pulmonary symptoms include orthopnea, paroxysmal nocturnal dyspnea, tachypnea, and cough
Fluid overload can result in pulmonary congestion and peripheral edema
10.
Nonspecific symptoms
Fatigue,
Nocturia,
Hemoptysis,
Abdominal pain,
Anorexia,
Nausea,
Bloating,
Ascites,
Poor appetite,
Mental status changes, and
Weight gain
11.
Physical examinationfindings may include
Pulmonary crackles,
An S3 gallop,
Cool extremities,
Cheyne-Stokes respiration - breathing disorder characterized by cyclical episodes of apnea and hyperventilation
Tachycardia,
Narrow pulse pressure,
Cardiomegaly,
Symptoms of pulmonary edema (extreme breathlessness, anxiety, sometimes with coughing pink, frothy sputum),
Peripheral edema,
Jugular venous distention,
hepatomegaly
12.
DIAGNOSIS
A completehistory and physical examination with appropriate laboratory testing are essential in the initial
evaluation of patients suspected of having HF
Laboratory tests for identifying disorders that may cause or worsen HF include
Compete blood count
Serum electrolytes
Renal function test
Liver function test
Thyroid function tests
Urinalysis
Lipid profile
Hemoglobin A1C
13.
Chest X-ray
ECG
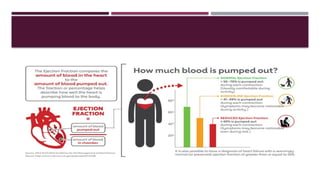
Echocardiogram is the single most useful evaluation procedure because it can identify abnormalities of the
pericardium, myocardium, or heart values and quantify the left ventricular ejection fraction (LVEF) to determine if
systolic or diastolic dysfunction is present
In ambulatory patients with dyspnea, measurement of BNP or N-terminal pro-B-type natriuretic peptide
(NT-proBNP) is useful to support clinical decision making regarding the diagnosis of HF, especially in the setting
of clinical uncertainty
Measurement of BNP or NT-proBNP is also useful for establishing prognosis or disease severity in chronic HF
14.
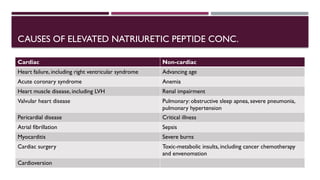
CAUSES OF ELEVATEDNATRIURETIC PEPTIDE CONC.
Cardiac Non-cardiac
Heart failure, including right ventricular syndrome Advancing age
Acute coronary syndrome Anemia
Heart muscle disease, including LVH Renal impairment
Valvular heart disease Pulmonary: obstructive sleep apnea, severe pneumonia,
pulmonary hypertension
Pericardial disease Critical illness
Atrial fibrillation Sepsis
Myocarditis Severe burns
Cardiac surgery Toxic-metabolic insults, including cancer chemotherapy
and envenomation
Cardioversion
15.
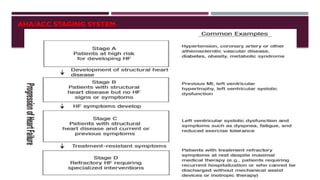
Both theACCF/AHA stages of HF and the NewYork Heart Association (NYHA)
functional classification provide useful and complementary information about the presence and severity of
HF.
The ACCF/AHA stages of HF emphasize the development and progression of disease and can be used to describe
individuals and populations, whereas
The NYHA classes focus on exercise capacity and the symptomatic status of the disease
DESIRED OUTCOMES
Thetherapeutic goals for chronic HF are to
Improve quality of life,
Relieve or reduce symptoms,
Prevent or minimize hospitalizations,
Slow disease progression, and prolong survival.
19.
TREATMENT
Non-pharmacological treatment
Patient education to facilitate HF self-care
Cardiac rehabilitation
Restriction of fluid intake (maximum 2 L/day from all sources) and dietary
Sodium (approximately 2 to 3 g of sodium per day)
Weight loss
Smoking cessation
20.
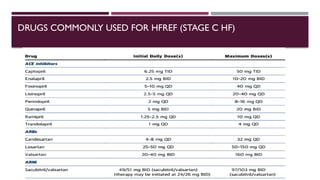
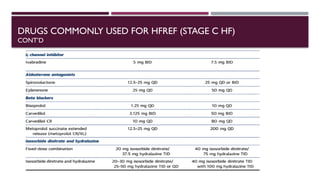
TREATMENT FOR STAGESA TO D (AHA/ACC GUIDELINES)
Stage A: Recommendations
Hypertension and lipid disorders should be controlled in accordance with contemporary guidelines to lower
the risk of HF
Other conditions that may lead to or contribute to HF, such as obesity, diabetes mellitus, tobacco use, and
known cardiotoxic agents, should be controlled or avoided.
21.
Stage B:Recommendations
Class I
In all patients with a recent or remote history of MI or ACS and reduced EF, ACE inhibitors should
be used to prevent symptomatic HF and reduce mortality. In patients intolerant of ACE inhibitors, ARBs are
appropriate unless contraindicated (Level of Evidence: A)
In all patients with a recent or remote history of MI or ACS and reduced EF, evidence-based beta
blockers should be used to reduce mortality (Level of Evidence: A)
In all patients with a recent or remote history of MI or ACS, statins should be used to prevent
symptomatic HF and cardiovascular events (Level of Evidence: A)
22.
In patientswith structural cardiac abnormalities, including LV hypertrophy, in the absence of a history of MI or
ACS, blood pressure should be controlled in accordance with clinical practice guidelines for hypertension to
prevent symptomatic HF
ACE inhibitors should be used in all patients with a reduced EF to prevent symptomatic HF, even if they do
not have a history of MI
Beta blockers should be used in all patients with a reduced EF to prevent symptomatic HF, even if they do not
have a history of MI (Level of Evidence: C)
23.
Class IIa
To prevent sudden death, placement of an implantable cardioverter-defibrillator (ICD) is
reasonable in patients with asymptomatic ischemic cardiomyopathy who are at least 40 days post-
MI, have an LVEF of 30% or less, are on appropriate medical therapy, and have reasonable
expectation of survival with a good functional status for more than 1 year (Level of Evidence: B)
Class III: Harm
Nondihydropyridine calcium channel blockers with negative inotropic effects may be harmful in
asymptomatic patients with low LVEF and no symptoms of HF after MI (Level of Evidence: C)
24.
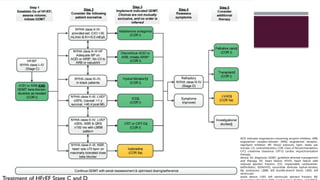
ACEI indicates angiotensin-convertingenzyme inhibitor; ARB,
angiotensin receptor-blocker; ARNI, angiotensin receptor-
neprilysin inhibitor; BP, blood pressure; bpm, beats per
minute; C/I, contraindication; COR, Class of Recommendation;
CrCl, creatinine clearance; CRT-D, cardiac resynchronization
therapy–
device; Dx, diagnosis; GDMT, guideline-directed management
and therapy; HF, heart failure; HFrEF, heart failure with
reduced ejection fraction; ICD, implantable cardioverter-
defibrillator; ISDN/HYD, isosorbide dinitrate hydral-nitrates;
Kþ, potassium; LBBB, left bundle-branch block; LVAD, left
ventricular
assist device; LVEF, left ventricular ejection fraction; MI,
#4 Regurgitation is the name for leaking heart valves. Sometimes the condition is minor and may not require treatment. At other times valve regurgitation places a strain on the heart. It can cause the heart to work harder and it may not pump the same amount of blood
#5 The infiltrative cardiomyopathies are a diverse group of cardiac diseases that are characterized by the deposition of abnormal substances within the heart tissue that causes the ventricular walls to develop either diastolic dysfunction or, less commonly and more of a late presentation of the disease, systolic dysfunction.
#6 ability of the heart to change its force of contraction and therefore stroke volume in response to changes in venous return is called the Frank-Starling mechanism (or Starling's Law of the heart)
#10 Hemoptysis is the coughing up of blood or blood-stained mucus from the bronchi, larynx, trachea, or lungs
#13 Ventricular hypertrophy can be demonstrated on chest x-ray or ECG. Chest x-ray may also show pleural effusions or pulmonary edema
the measurement of troponin I or T should be routine in patients presenting with acutely decompensated HF syndromes
#20 The emphasis is on identifying and modifying risk factors to prevent development of structural heart disease and subsequent HF. Strategies include smoking cessation and control of hypertension, diabetes mellitus, and dyslipidemia according to current treatment guidelines
![PTHOPHYSIOLOGY
Causes of systolic dysfunction (decreased contractility) are
Reduction in muscle mass (e.g., myocardial infarction [MI]),
Dilated cardiomyopathies, and
Ventricular hypertrophy.
Ventricular hypertrophy can be caused by pressure overload (e.g., systemic or pulmonary hypertension, aortic or
pulmonic valve stenosis) or volume overload (e.g., valvular regurgitation, shunts, high-output states)](https://image.slidesharecdn.com/hf-260107032826-ee6cabbe/85/Heart-failure-definition-condition-ecg-4-320.jpg)