The study examined the correlation between axial blood velocity (Vax) and microvessel diameter (D) in 104 human conjunctival venules and 30 arterioles. Venules were divided into 4 groups based on diameter size. For venules, Vax increased with diameter but the correlation was weak and not significant within each diameter group. Vax was significantly lower in smaller venule groups compared to larger groups. For arterioles, there was no correlation between Vax and diameter. The results suggest Vax is dependent on diameter at a broader scale but not for small variations within defined diameter ranges in human microvasculature.
![AUTHORCOPY
Clinical Hemorheology and Microcirculation 61 (2015) 429–438
DOI 10.3233/CH-141888
IOS Press
429
Correlation of axial blood velocity to venular
and arteriolar diameter in the human eye
in vivo
Aristotle G. Koutsiaris∗
Bio-Medical Informatics Laboratory, Department of Medical Laboratories, School of Health Sciences,
Technological Educational Institute (TEI) of Thessaly, Larissa, Greece
Abstract. The axial blood velocity (Vax) association with microvessel diameter (D) was studied at 104 different postcapillary
venules (4 m < D < 24 m) and 30 different precapillary arterioles (6 m ≤ D ≤ 12 m) in the human conjunctiva of normal
healthy humans. Venular diameter sizes were classified as “very small” (Group 1, 4.4 m ≤ D < 8.9 m), “small” (Group 2,
8.9 m ≤ D < 13.8 m), “medium” (Group 3, 13.8 m ≤ D < 19.1 m) and “large” (Group 4, 19.1 m ≤ D ≤ 23.5). The Spear-
man’s correlation coefficient (rs) in all 4 venular groups was less than 0.36 and not statistically significant (n = 26, p ≥ 0.08).
Similar correlation results were observed for the arteriolar group (rs) ≈ 0) for the peak systolic, the average and the end systolic
axial velocities. Vax was significantly (p < 0.001) lower in Group 1 in comparison to that in Group 2 and significantly (p < 0.01)
lower in Group 2 in comparison to that in Group 3. However, Vax was not significantly lower in Group 3 in comparison to that
in Group 4. Average Vax and standard deviation was 0.48 ± 0.13, 0.64 ± 0.16, 0.82 ± 0.25 and 0.88 ± 0.32 mm/s for Groups
1, 2, 3 and 4 respectively. The above results reinforce the importance of measuring D in microvascular hemodynamics. Higher
diameters suggest higher axial velocities but Vax does not change significantly within the limits of each of the aforementioned
groups.
Keywords: Human, eye, conjunctiva, venules, arterioles, axial velocity, diameter, correlation
1. Introduction
Blood velocity measurements in the human smallest microvessels appeared in the seventies [3, 4, 10].
Since then, several groups published velocity measurements from various human tissues such as the nail
fold [24, 28, 29, 34], the bulbar conjunctiva [6, 12, 13, 18, 20, 32] and the retina [1, 23, 30, 35].
In the majority of the above cases the quantity that was actually measured was the axial or centerline
blood velocity (Vax). However, the relationship of Vax to micro vessel diameter has not been studied in
detail, in humans. In fact, many of the researchers did not report diameter measurements in relation to
the measured Vax [1, 13, 23, 30, 34].
In general, in mammal microcirculation, higher diameters suggest higher velocities but this general
principle does not seem to be valid for small variations of diameter [16]. The question that has not been
answered yet is how “small” these diameter variations might be and answering this question for humans
was one of the targets of this work.
∗
Corresponding author: Dr. Aristotle Koutsiaris, 9 Miauli St, 41223 Larissa, Greece. Tel.: +30 2410 411284; E-mails:
ariskout@otenet.gr; ariskout@teilar.gr.
1386-0291/15/$35.00 © 2015 – IOS Press and the authors. All rights reserved](https://image.slidesharecdn.com/4b2023b9-f8eb-47ae-a2dc-f01802bdcb84-160605085945/85/HDMICS-Koutsiaris-2016-1-320.jpg)
![AUTHORCOPY
430 A.G. Koutsiaris / Correlation of axial blood velocity to venular and arteriolar diameter
If a monotonic association between Vax and D does not exist or, if it is weak and not statistically
significant, at a specific diameter range, then all velocity measurements in that range could be treated as
one group or cluster. Therefore, another target of this work was to give average values of Vax of healthy
individuals in correspondence to specific diameter ranges. This could be proved useful to other exper-
imental investigations and to other groups developing new semi-automatic or fully automatic velocity
measurement techniques.
In addition, it could have a clinical or diagnostic application. For example, conjunctival Vax has been
used to discriminate sickle cell disease patients [6], Alzheimer’s disease patients [27] and Type-1 diabetes
mellitus patients [7].
Also, statistically significant differences in the Vax of the conjunctival microcirculation have been
reported after the application of contact lenses [8, 12] and transfusion therapy [9].
Other important hemodynamic parameters which can be estimated from Vax are volume flow Q [17],
wall shear stress WSS [18, 21], the velocity profile [19] and the resistive index RI [20, 22].
All the above parameters are essential in many research areas such as theoretical models on vascular
design [15], the amount of chemicals exchanged between blood and tissue, the micro mechanobiology
of endothelium cells in health and disease and vascular targeted drug carriers [5].
Furthermore, hemodynamic parameters are important for the realistic design of in vitro apparatuses
and assays for the study of angiogenesis [14], the blood brain barrier [25], the endothelial response [11,
31] and cell adhesion. Cell adhesion is a broad topic implicated in many research areas comprising the
attachment of circulating tumor cells, tissue engineering and regenerative medicine [33].
2. Methods
This work was carried out using previously measured velocity data [18, 20]. However, data statistical
processing, results and conclusions are all new.
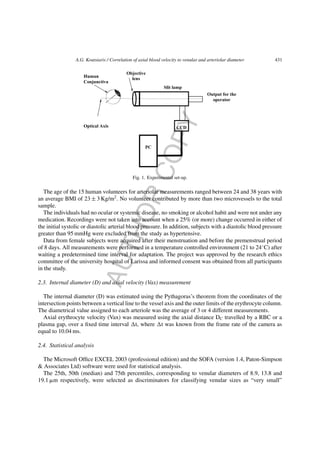
2.1. Experimental set up
The experimental set up (Fig. 1) consisted of a slit lamp (Nikon FS-3 V) connected with a high-speed
CCD camera (12 bit, PCO Computer Optics GmbH, Germany) and a PC (Pentium 4, 3 GHz). The system
produced digital images of 320 × 240 pixels at a frame rate of 96 frames per second (fps) with an enhanced
maximum magnification of 242x and a digital resolution of 1.257 ± 0.004 m/pixel.
2.2. Subjects
Images were taken from the venules of the right eyes (temporal side of the bulbar conjunctiva) of 17
normal human volunteers (8 men and 9 women) and from the arterioles of the right eyes (temporal side
of the bulbar conjunctiva) of 15 normal human volunteers (9 men and 6 women).
The age of the 17 human volunteers for venular measurements ranged between 25 and 38 years with an
average body mass index (BMI, defined as the number of body kilograms over the square of the height)
of 24 ± 3 Kg/m2
. All volunteers contributed by approximately the same number of velocity points (5 to
7) to the total sample and from the total velocity point ensemble, 54 points were from females and 50
points were from males.](https://image.slidesharecdn.com/4b2023b9-f8eb-47ae-a2dc-f01802bdcb84-160605085945/85/HDMICS-Koutsiaris-2016-2-320.jpg)
![AUTHORCOPY
432 A.G. Koutsiaris / Correlation of axial blood velocity to venular and arteriolar diameter
(Group 1, 4.4 m ≤ D < 8.9 m), “small” (Group 2, 8.9 m ≤ D < 13.8 m), “medium” (Group 3,
13.8 m ≤ D < 19.1 m) and “large” (Group 4, 19.1 m ≤ D≤23.5).
The majority of the variable distributions were not normal and therefore differences between vessel
groups were examined using the Mann-Whitney U test. Spearman’s rank correlation coefficient (rs) was
used for measuring the strength of monotonic association between D and Vax. The level of significance
was set at p < 0.05.
3. Results
Venular diameters ranged between 4 and 24 m and venular axial velocities between 0.24 and
1.70 mm/s. Venular velocity points are shown as black dots in Fig. 2a. In the same figure, velocity
points were grouped by vessel size into four venular groups with 26 points each, without overlapping
diameters, according to the Methods section.
The Spearman’s correlation coefficient (rs) for the 4 venular groups was less than 0.36 and not
statistically significant (n = 26, p ≥ 0.08) as it is shown in Table 1.
Descriptive statistics of D and Vax are shown in Tables 2, 3 and 4 for all four venular groups. The range
of diameters for all vessel groups was between 4.4 and 5.1 m. D and Vax were significantly (p < 0.001)
lower in Group 1 in comparison to those in Group 2 (Table 2) and significantly (p < 0.01) lower in Group
2 in comparison to those in Group 3 (Table 3). However, Vax was not significantly lower in Group 3 in
comparison to that in Group 4 (Table 4).
In Fig. 2b, axial velocity average and standard deviation values are shown for each venular ves-
sel group, namely 0.48 ± 0.13, 0.64 ± 0.16, 0.82 ± 0.25 and 0.88 ± 0.32 mm/s for Group 1, 2, 3 and 4
respectively.
Finally, at the arteriolar side of the human bulbar conjunctiva, arteriolar diameters ranged between 6
and 12 m and arteriolar axial velocities between 0.40 and 5.84 mm/s, as it is shown in Fig. 3. There
was practically no monotonic association (rs ≈ 0) between axial velocity and arteriolar diameter. This
was true for either the peak systolic (ARTPSV), the average (ARTAVV) and the end systolic (ARTEDV)
axial velocities.
4. Discussion
The human eye is an open window to the human microcirculation and in most of the ophthalmology
departments there are instruments with which operators can see blood flow. With some modifications, the
same instruments can be used to acquire image data appropriate for hemodynamic and morphological
quantification [6, 12, 18, 26].
The most frequently measured hemodynamic parameters in the microcirculation are vessel diameter
and axial blood velocity but not always in relation to one another.
In this work, conjunctival venules were categorized into four (4) groups by diameter and, investigating
Vax in relation to D inside the limits of each group, it was found that there was no monotonic association
(and consequently no correlation) between axial velocity and diameter.
The same was observed for the arteriolar group and it is furthermore supported by earlier recordings
from rabbit mesenteric precapillary arterioles [16]. Vax measurements from a total of 19 mesenteric
precapillary arterioles ranging in diameter between 7.4 and 12.4 m are shown in Fig. 4. Measurements
from 9 more precapillary arterioles are presented here in addition to those from 10 arterioles published](https://image.slidesharecdn.com/4b2023b9-f8eb-47ae-a2dc-f01802bdcb84-160605085945/85/HDMICS-Koutsiaris-2016-4-320.jpg)


![AUTHORCOPY
A.G. Koutsiaris / Correlation of axial blood velocity to venular and arteriolar diameter 435
Fig. 3. Blood axial velocity (Vax) versus diameter (D) in the precapillary arterioles of the human bulbar conjunctiva. ARTeriolar
Peak Systolic Velocities (ARTPSV) are shown as rhombuses, ARTeriolar AVerage Velocities (ARTAVV) are shown as black
dots and ARTeriolar End Diastolic Velocities (ARTEDV) are shown as crosses. In all cases, there was no statistically significant
monotonic association (rs ≈ 0, p > 0.5).
Fig. 4. Blood axial velocity (Vax) versus diameter (D) in the precapillary arterioles of the rabbit mesentery. ARTeriolar Peak
Systolic Velocities (ARTPSV) are shown as rhombuses, ARTeriolar AVerage Velocities (ARTAVV) are shown as black dots
and ARTeriolar End Diastolic Velocities (ARTEDV) are shown as crosses. In all cases, there was no statistically significant
monotonic association (0.13 ≤ rs ≤ 0.41, p ≥ 0.08).
previously [16]. There was no statistically significant (p ≥ 0.08) monotonic association between arteriolar
velocity and diameter for either the peak systolic (ARTPSV), the average (ARTAVV) and the end systolic
(ARTEDV) values.
The above two paragraphs lead to a useful conclusion concerning axial blood velocity, that for venular
diameter spans less than ≈ 5 m (Fig. 2a) and for arteriolar diameter spans less than ≈ 6 m (Fig. 3),
there is practically no correlation between Vax and D.](https://image.slidesharecdn.com/4b2023b9-f8eb-47ae-a2dc-f01802bdcb84-160605085945/85/HDMICS-Koutsiaris-2016-7-320.jpg)
![AUTHORCOPY
436 A.G. Koutsiaris / Correlation of axial blood velocity to venular and arteriolar diameter
The next step was to compare the axial velocities from the 4 different venular groups. A statistically
significant difference among axial velocities in the first three groups (Tables 2 and 3) was found, indicating
the importance of vessel diameter as a parameter influencing the value of axial velocity. This should be
taken into account, especially when using instruments and techniques for measuring velocity in high
diameter spans, for example between 4 and 40 m [23].
The results shown in Table 3 for Groups 2 and 3 are in accordance with Wanek et al. [32] who found
a statistically significant difference between axial velocities measured in venules categorized into two
groups by vessel size using the diameter of 15 microns as a discriminator.
The average velocities of each of the 4 venular groups (Fig. 2b), might be used in future works for
gross comparisons between different experimental methods and different subject groups, physiological
or pathological.
As a first example, regarding physiological subjects, the average Vax of 0.60 mm/s measured by Wanek
et al. [32] and Jiang et al. [12] in diameters higher than 15 m is approximately 27% lower than that
of 0.82 mm/s measured here in Group 3 (Fig. 2b). In addition, the average Vax of 0.32 mm/s measured
by Wanek et al. [32] in diameters of 11.2 (±0.9) m is 50% lower than that of 0.64 mm/s measured
here in Group 2 (Fig. 2b). Given that both Wanek et al. [32] and Jiang et al. [12] measured velocity with
semi-automated methods based on variations of the space-time image technique, these discrepancies may
be a result of the different measurement techniques.
As a second example, the average Vax value of 0.48 mm/s reported here for diameters between 4.4 and
8.8 m (Fig. 2b, Table 2), is more than double the average value of 0.19 mm/s reported by Ubbink et al.
[29] at a diameter of 5 m in the nail-fold of the big toe in the supine position. However, except from
the fact that they measured at a different tissue, their measurements were from 16 asymptomatic patients
with a mean age of 70 years. In addition, some of them were under vasoactive medication and presented
signs of atheromatic disease. Furthermore, they measured using the flying spot technique introduced by
Basler (1919) which is a subjective technique accurate for very slow varying flows (periods longer than
5 seconds).
Ubbink et al. [29] showed that video microscope velocimetry has predictive and discriminative power
to discern patients belonging to different Fontaine stages. However, a physiological reference of axial
velocity in relation to diameter from the human big toe nail-fold is missing.
Concerning pathological situations, Wanek et al. [32] found differences in the hemodynamic behavior
between SS and SC sickle cell disease patients, indicating a diagnostic potential of video microscope
velocimetry.
In conclusion, the results of this work showed the importance of measuring diameter and subdividing
microvessels accordingly in hemodynamic studies either clinical or not. Higher diameters suggest higher
axial velocities but not for diameter changes less than approximately 5 m in venules and 6 m in
arterioles.
References
[1] O. Arend, A. Harris, B.J. Martin and A. Remky, Scanning laser ophthalmoscopy-based evaluation of epipapillary velocities:
Method and physiologic variability, Surv Ophthalmol 44(Suppl 1) (1999), S3–9.
[2] A. Basler, Uber die bestimmung der stromungsgeschwindgkeit in den blutkapillaren der menschlichen Haut, Munchner
Med Wschr 13 (1919), 347–348.
[3] A. Bollinger, P. Butti, J.-P. Barras, H. Trachsler and W. Siegenthaler, Red blood cell velocity in nailfold capillaries of man
measured by a television microscopy technique, Microvasc Res 7 (1974), 61–72.](https://image.slidesharecdn.com/4b2023b9-f8eb-47ae-a2dc-f01802bdcb84-160605085945/85/HDMICS-Koutsiaris-2016-8-320.jpg)
![AUTHORCOPY
A.G. Koutsiaris / Correlation of axial blood velocity to venular and arteriolar diameter 437
[4] P. Buti, M. Intaglietta, H. Reimann, C.H. Holliger, A. Bollinger and M. Anliker, Capillary red blood cell velocity
measurements in human nailfold by videodensitometric method, Microvasc Res 10 (1975), 220–227.
[5] P. Charoenphol, R.B. Huang and O. Eniola-Adefeso, Potential role of size and hemodynamics in the efficacy of vascular-
targeted spherical drug carriers, Biomaterials 31 (2010), 1392–1402.
[6] A.T.W. Cheung, P.C.Y. Chen, E.C. Larkin, P.L. Duong, S. Ramanujam, F. Tablin and T. Wun, Microvascular abnormalities
in sickle cell disease: A computer assisted intravital microscopy study, Blood 99 (2002), 3999–4005.
[7] A.T.W. Cheung, M.M. Smith, P.C.Y. Chen, E. Miguelino, C.S. Li and S. Devaraj, Correlation of microvascular abnormalities
and endothelial dysfunction in Type-1 Diabetes Mellitus (T1DM): A real-time intravital microscopy study, Clin Hemorheol
Microcirc 42 (2009), 285–295.
[8] A.T.W. Cheung, B.S. Hu, S.A. Wong, J. Chow, M.S. Chan, W.J. To, J. Li, S. Ramanujam and P.C.Y. Chen, Microvascular
abnormalities in the bulbar conjunctiva of contact lens users, Clin Hemorheol Microcirc 51 (2012), 77–86.
[9] A.T.W. Cheung, J.W. Miller, M.G. Miguelino, W.J. To, J. Li, X. Lin, P.C. Chen, S.L. Samarron, T. Wun, T. Zwerdling
and R. Green, Exchange transfusion therapy and its effects on real-time microcirculation in pediatric sickle sell anemia
patients: An intravital microscopy study, J Pediatr Hematol Oncol 34 (2012), 169–174.
[10] B. Fagrell, A. Fronek and M. Intaglietta, A microscope-television system for studying flow velocity in human skin
capillaries, Am J Physiol 233 (1977), H318–H321.
[11] S. Forconi and T. Gori, Endothelium and hemorheology, Clin Hemorheol Microcirc 53 (2013), 3–10.
[12] H. Jiang, J. Zhong, D.C. DeBuc, A. Tao, Z. Xu, B.L. Lam, C. Liu and J. Wang, A functional slit lamp biomicroscopy for
imaging bulbar conjunctival microvasculature in contact lens wearers, Microvasc Res 92 (2014), 62–71.
[13] H. Jiang, Y. Ye, D.C. DeBuc, B.L. Lam, T. Rundek, A. Tao, Y. Shao and J. Wang, Human conjunctival microvasculature
assessed with a retinal function imager (RFI), Microvasc Res 85 (2013), 134–137.
[14] H. Kang, H.I. Kwak, R. Kaunas and K.J. Bayless, Fluid shear stress and sphingosine 1-phosphate activate calpaine to
promote membrane type 1 matrix metalloproteinase (MT1-MMP) membrane translocation and endothelial invasion into
three-dimensional collagen matrices, J Biol Chem 286 (2011), 42017–42026.
[15] G.S. Kassab, Scaling laws of vascular trees: Of form and function, Am J Physiol Heart Circ Physiol 290 (2006),
H894–H903.
[16] A.G. Koutsiaris and A. Pogiatzi, Velocity pulse measurements in the mesenteric arterioles of rabbits, Physiol Meas 25
(2004), 15–25.
[17] A.G. Koutsiaris, Volume flow estimation in the precapillary mesenteric microvasculature in-vivo and the principle of
constant pressure gradient, Biorheology 42 (2005), 479–491.
[18] A.G. Koutsiaris, S.V. Tachmitzi, N. Batis, M.G. Kotoula, C.H. Karabatsas, E. Tsironi and D.Z. Chatzoulis, Volume flow
and wall shear stress quantification in the human conjunctival capillaries and post-capillary venules in-vivo, Biorheology
44 (2007), 375–386.
[19] A.G. Koutsiaris, A velocity profile equation for blood flow in small arterioles and venules of small mammals in vivo and
an evaluation based on literature data, Clin Hemorheol Microcirc 43 (2009), 321–334.
[20] A.G. Koutsiaris, S.V. Tachmitzi, P. Papavasileiou, N. Batis, M. Kotoula, A.D. Giannoukas and E. Tsironi, Blood velocity
pulse quantification in the human conjunctival pre-capillary arterioles, Microvasc Res 80 (2010), 202–208.
[21] A.G. Koutsiaris, S.V. Tachmitzi and N. Batis, Wall shear stress quantification in the human conjunctival pre-capillary
arterioles in vivo, Microvasc Res 85 (2013), 34–39.
[22] A.G. Koutsiaris, The resistive index as a function of vessel diameter in the human carotid arterial tree, Microvasc Res 89
(2013), 169–171.
[23] G. Landa, A.A. Jangi, P.M.T. Garcia and R.B. Rosen, Initial report of quantification of retinal blood flow velocity in normal
human subjects using the Retinal Functional Imager (RFI), Int Ophthalmol 32 (2012), 211–215.
[24] L.C. Lo, K.C. Lin, Y.N. Hsu, T.P. Chen, J.Y. Chiang, Y.F. Chen and Y.T. Liu, Pseudo three–dimensional vision-based
nail-fold morphological and hemodynamic analysis, Computers in Biology and Medicine 42 (2012), 873–884.
[25] P. Naik and L. Cucullo, In vitro blood-brain barrier models: Current and perspective technologies, J Pharm Sci 101 (2011),
1337–1354.
[26] M. Shahidi, J. Wanek, B. Gaynes and T. Wu, Quantitative assessment of conjunctival microvascular circulation of the
human eye, Microvasc Res 79 (2010), 109–113.
[27] M.M. Smith, P.C.Y. Chen, C.S. Li, S. Ramanujam and A.T.W. Cheung, Whole blood viscosity and microvascular abnor-
malities in Alzheimer’s Disease, Clin Hemorheol Microcirc 41 (2009), 221–239.
[28] D.T. Ubbink, M.J.H.M. Jacobs, D.W. Slaaf, G.J.W.J.M. Tangelder and R.S. Reneman, Capillary recruitment and pain relief
on leg dependency in patients with severe lower limb ischemia, Circulation 85 (1992), 223–229.](https://image.slidesharecdn.com/4b2023b9-f8eb-47ae-a2dc-f01802bdcb84-160605085945/85/HDMICS-Koutsiaris-2016-9-320.jpg)
![AUTHORCOPY
438 A.G. Koutsiaris / Correlation of axial blood velocity to venular and arteriolar diameter
[29] D.T. Ubbink, M.J.H.M. Jacobs, G.J. Tangelder, D.W. Slaaf and R.S. Reneman, The usefulness of capillary microscopy,
transcutaneous oximetry and laser Doppler fluxmetry in the assessment of the severity of the lower limb ischaemia, Int J
Microcirc 14 (1994), 34–44.
[30] A. Uji, M. Hangai, S. Ooto, K. Takayama, N. Arakawa, H. Imamura, K. Nozato and N. Yoshimura, The source of moving
particles in parafoveal capillaries detected by adaptive optics scanning laser ophthalmoscopy, Invest Ophthalmol Vis Sci
53 (2012), 171–178.
[31] F. Vozzi, F. Bianchi, A. Ahluwalia and C. Domenici, Hydrostatic pressure and shear stress affect endothelin-1 and nitric
oxide release by endothelial cells in bioreactors, Biotechnology Journal 9 (2014), 146–154.
[32] J. Wanek, B. Gaynes, J.I. Lim, R. Molokie and M. Shahidi, Human bulbar conjunctival hemodynamics in haemoglobin SS
and SC disease, Am J Hematol 88 (2013), 661–664.
[33] J.W. Warrick, E.W.K. Young, E.G. Schmuck, K.W. Saupe and D.J. Beebe, High-content adhesion assay to address limited
cell samples, Integrative Biology (Camb) 5 (2013), 720–727.
[34] C.C. Wu, G. Zhang, T.C. Huang and K.P. Lin, Red blood cell velocity measurements of complete capillary in finger nail-fold
using optical flow estimation, Microvasc Res 78 (2009), 319–324.
[35] Z. Zhong, B.L. Petrig, X. Qi and S.A. Burns, In vivo measurement of erythrocyte velocity and retinal blood flow using
adaptive optics scanning laser ophthalmoscopy, Opt Express 16 (2008), 12746–12756.](https://image.slidesharecdn.com/4b2023b9-f8eb-47ae-a2dc-f01802bdcb84-160605085945/85/HDMICS-Koutsiaris-2016-10-320.jpg)











































































