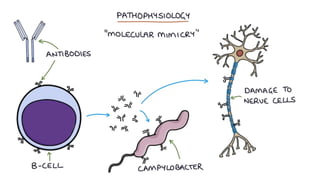
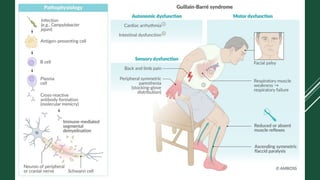
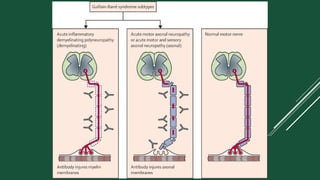
Guillain-Barré syndrome (GBS) is a rare, acute neurological disorder where the body's immune system mistakenly attacks its own peripheral nerves. This autoimmune response damages the nerve's protective covering (myelin sheath) or the nerve fibers (axons), disrupting the transmission of signals between the brain and the rest of the body.