Download to read offline

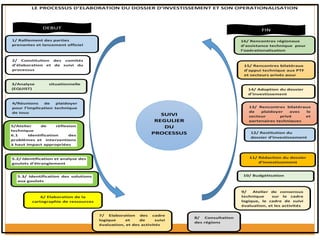


The document discusses the GFF process in Cameroon, including national health statistics, challenges in maternal and child health, and the importance of investment cases. It outlines the operationalization steps for developing the investment case, highlighting the involvement of stakeholders and the role of the private sector in financing. The GFF aims to improve health outcomes by increasing resources for maternal and child health in the country while addressing key bottlenecks and enhancing data quality.






























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




