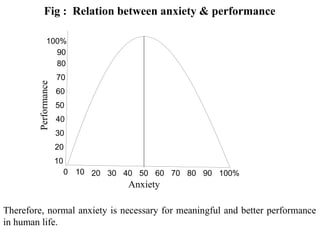
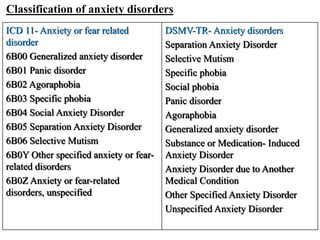
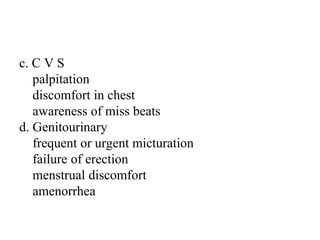
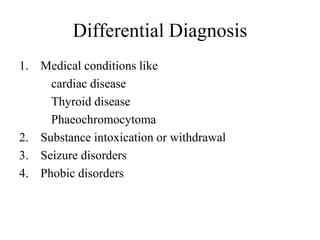
This document provides information on anxiety disorders, including what anxiety is, normal versus pathological anxiety, common anxiety symptoms, and descriptions of several specific anxiety disorders like generalized anxiety disorder, panic disorder, phobic anxiety disorders, and obsessive compulsive disorder. For each disorder, it discusses diagnostic features, differential diagnosis, and management approaches including education, relaxation techniques, medications, cognitive behavioral therapy, and referral to specialists.