INTRODUCTION
An unborn OffspringThat develops
and grows inside the Uterus (womb)
Of humans and other mammals.
In humans fetal Period begins from 8t
h
week after fertilization and it ends at
the time of birth.
3.
DEVELOPMENT OF FETUS
Thefetus grows from a diploid zygote to almost 6 billion cells by
38 weeks of gestation and at the time of birth the baby weighting
on an average of 2.9kg.
This fetal growth is influenced by genetic factors, placental
factors, sex of the fetus,parity and maternal nutrition.
Fetal growth can be judged by maternal weight
gain , symphyseofundal height and Ultrasound
5.
Respiratory system
Breathing movementare present as early as 11
weeks but these are irregular,become regular as
term approaches..
Final stage of alveolar development occurs by
23 weeks
Type 2 pneumocytes also produce
surfactant,which prevent alveolar collapse.
6.
Clinical importance ofsurfactant
The presence of surfactant in amniotic fluid is evidences of fetal lug
maturity. Surfactant is composed of 90% lipids and 10% protein
80% of the glycerophospholipids are phosphatidyl choline(lecithin).
The main active component of surfactant is dipalmitoyl phosphatidyl
choline.
Second active component is phosphatidyl glycerol.these components
along with phosphatidyl inositol are very important for the prevention of
RDS.
7.
Renal system
Excretory functionis mainly carried out by placenta .
In late pregnancy amniotic fluid sodium level fall while
creatinine rises.this is because the fetal kidney is unable
to conserve sodium efficiently.
The kidney produce 500-700ml of urine per day and this
is the major contributor to liquor volume from
approximately 20 weeks.
8.
Central Nervous system
After3 weeks of post implementation the CNS begins to
form. However , functional maturity is attained much later.
Blood supply to the brain is always maintained and even
in fetal growth restriction, there is brain sparing effect.
9.
Peripheral Nervous system
Gangliaand nerves appear by 28-35 days , however
motor and sensory nerve endings appear later
(12-16weeks)
The autonomous nervous system with the baroreceptor
mechanisms and pulmonary reflexes mature only
towards term.
10.
Skin
Sabaceous glands areresponsible for the production
of vernix caseosa
Sweat glands do not function very early they are not
required to regulate any water or eletrolyte
balance ,as this is done by placenta .
11.
Alimentary Tract
The fetusswallows fluid as early as 12 weeks and at term,
almost 250ml/day
The villi and glands are formed early and digestive enzymes
can be seen by 16-18 weeks .
The first stool of the New born is called
‘Meconium’. It is dark in colour due to
biliverdin.
This meconium contains cell,hair,Mucous and other
intestinal meterials.
12.
Reproductive system
T
estis isformed by 8 weeks and the Ovary is formed by 10
weeks. The wolffian and Mullerian structures are formed by 10-
12 weeks.
The external genitalia upto 10 weeks consisting of 2-urogenital fold,2-genital
swelling and a midline anterior genital tubercle.
In female genital tubercle – clitoris
Genital fold - labia
minora Genital swelling –
labia majora
The male development completed by 12 weeks ,and female development by
15 weeks.
13.
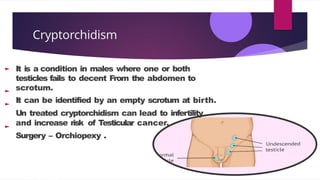
Cryptorchidism
It is acondition in males where one or both
testicles fails to decent From the abdomen to
scrotum.
It can be identified by an empty scrotum at birth.
Un treated cryptorchidism can lead to infertility
and increase risk of Testicular cancer.
Surgery – Orchiopexy .
14.
HAEMATOLO
GICAL
CHANGES
1. HAEMOPOIESIS (BLOODCELL
FORMATION)
SITES OF HAEMOPOIESIS
a)YO L K SAC
•First RBCs formed at 14 days.
•Produces macrocytic, nucleated RBCs with polychromatic
cytoplasm
•Not influenced by erythropoietin.
b)LIV ER
•Becomes haemopoietic from 6–10 weeks.
•Major site in 1st
& early 2nd
trimester.
•Activity declines in 2nd
trimester; stops by term.
c)B O N E M A R R OW
• Starts forming blood cells at 7–18 weeks.
• Progenitor cells present by 15–16 weeks.
• Becomes dominant site by mid-gestation
onwards.
d)SPLEEN
•Starts haemopoiesis at 19–20
weeks.
e)T H Y M U S & LY M P H N O D E S
•Act as supplemental sites during the 3rd
trimester.
1. Haemopoiesis (Blood Cell
Formation)
2. Red blood cells
3. Haemoglobin
4. Leucocytes and platelets
5. Immunoglobulins
15.
2. RED BLOOD
CELLS
►RBC concentration increases throughout gestation.
► At term: 5.1 × 10¹² / L.
► Hemoglobin rises from 6 g/dL (10 weeks) to 16–18
g/dL at term.
► Packed cell volume increases from 20% → 40%.
► Fetal RBCs are larger and more numerous.
► Fetal RBC lifespan ≈ 80 days.
► The Rh factor is developed by 38 days.
16.
3. HAEMOGLOBIN
HbF (α₂γ₂)
30%at 5 weeks.
≈90% of total Hb by 8 weeks.
High oxygen affinity (→
efficient oxygen transfer from
mother).
It is resistant to alkali and
acid.
Oxygen affinity: 80% in fetus
vs. 40% in mother.
HbA (α₂β₂)
► Appears at 5–10%
throughout gestation.
► Increases after 32–36
weeks.
► <1% after 4 months of birth.
► Fetal blood carries 25 mL O₂
/ 100 mL blood(maternal
blood carries 15 mL).
► Rh factor develops by 38
days.
17.
4. LEUKOCYTES AND
PLATELETS
►Leukocytes increase
progressively. At term: 15,000–
20,000 / mm³.
Thymus & spleen → major
lymphocyte sources.
Fetus produces minimal
antibodies (mostly maternal
transfer).
Platelet :
•Megakaryocytes appear in yolk
18.
5.IMMUNOGL
OBULINS •
IgG
→Only immunoglobulin
thatcrosses the placenta.
→Transfer begins at 12
weeks.
→Provides passive
maternal immunity.
•IgM
→Produced by fetus (does
not cross placenta).
→Presence at birth
suggests intrauterine
infection.
•IgA
→Produced only after birth
19.
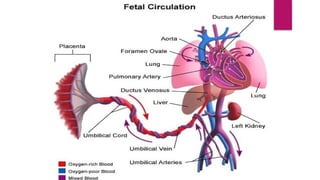
CARDIOVASCUL
A R SYSTEM
Developmentof the Heart
1.The heart appears as two tubes at 18 days of
embryonic life.
2. These tubes fuse into a single heart tube by 22 days.
3. The heart tube elongates and forms chambers.
4.The heart starts beating by 22 days, but it is
detected clinically much later.
20.
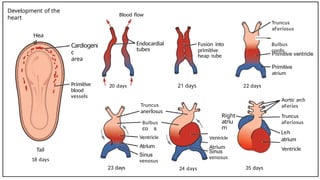
Development of the
heart
Hea
d
Tail
18days
Cardiogeni
c
area
Primitive
blood
vessels
Blood flow
20 days
23 days
Endocardial
tubes
Truncus
anerlosus
Bulbus
Ventricle
Atrium
venosus
21 days
24 days
Fusion into
primitive
heap tube
Right
atriu
m
Ventricle
Atrium
venosus
22 days
35 days
Truncus
aFeriosus
—
Bulbus
cordis
atrium
Aortic arch
aFeries
Truncus
aFeriosus
Leh
atrium
Ventricle
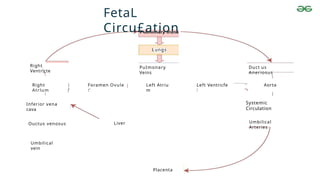
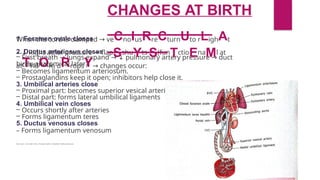
1. Foramen ovalecloses
2. Ductus arteriosus closes
– First breath → lungs expand → ↓ pulmonary artery pressure → duct
constricts.
– Becomes ligamentum arteriosum.
– Prostaglandins keep it open; inhibitors help close it.
3. Umbilical arteries close
– Proximal part: becomes superior vesical arteries
– Distal part: forms lateral umbilical ligaments
4. Umbilical vein closes
– Occurs shortly after arteries
– Forms ligamentum teres
5. Ductus venosus closes
– Forms ligamentum venosum
-
--
If you want, I can make it into a flowchart, table, or ultra-short 1-slide summary too.
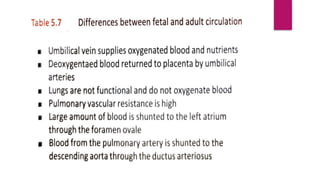
CHANGES AT BIRTH
When the cord is clamped → veCnoIusRreCturnUto rLighAt
atTriuOm dRropsY→ changes occur:
– ↓ Right atrial pressure → flapSshuYts S(funTctioEnaMl at
birth; anatomical later).
26.
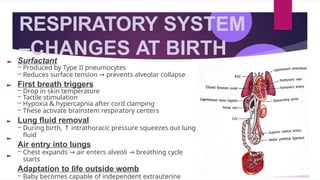
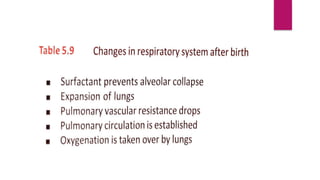
RESPIRATORY SYSTEM
–CHANGES ATBIRTH
Surfactant
– Produced by Type II pneumocytes
– Reduces surface tension → prevents alveolar collapse
First breath triggers
– Drop in skin temperature
– Tactile stimulation
– Hypoxia & hypercapnia after cord clamping
– These activate brainstem respiratory centers
Lung fluid removal
– During birth, ↑ intrathoracic pressure squeezes out lung
fluid
Air entry into lungs
– Chest expands → air enters alveoli → breathing cycle
starts
Adaptation to life outside womb
– Baby becomes capable of independent extrauterine