5
Practical Training Rotation
1st
Week
Biostatistics & Data Collection of House Hold Survey
2nd
Week
Biostatistics
House Hold Survey / Data analysis
7
Assessment
MCQs :15 Marks
OSPE: 20 Marks (5 Stations , 4 marks each)
House Hold Survey: 15 Marks
Total : 50 Marks
* The marks will be added in the practical
internal assessment
8.
8
Objectives of thelecture
The students should be able to:
Define public health
Know the phases of evolution of public health.
Appreciate the philosophy of new public health
Appreciate the difference between clinical and
community medicine
11
EVOLUTION OF PUBLICHEALTH
(ANCIENT MEDICINE)
Indian medicine
Chinese medicine
Egyptian
medicine
Greek medicine
Roman medicine
12.
12
Phases of evolution
Dawnof scientific medicine
Changing concepts of public health
1. Environmental (1846)
2. Individualistic (1870)
3. Therapeutic (1940)
13.
History
In analmost complete absence of scientific
medical knowledge, it would not be fair to say
that the early practitioners of medicine
contributed nothing to the alleviation of man's
suffering from disease.
13
Medical knowledge has been derived from the
observations and cumulative experiences gleaned
from others.
It is study of the
evolution of man and of
human knowledge down
the ages
14.
Medicine hasdrawn from the traditional
cultures, and later from biological and natural
sciences and more recently from social and
behavioral sciences.
14
The "explosion" of knowledge
during the 20th century has
made medicine more complex,
and treatment more costly
15.
The glaringcontrasts in the
state of health between the
developed and developing
countries, between the
rural and urban areas, and
between the rich and poor
have attracted worldwide
criticism as "social injustice
15
". The commitment of all countries,
under the banner of the World
Health Organization, is to wipe out
the inequalities in the distribution of
health resources and services, and
attain the Millenium Development
Goals
16.
Goal of ModernMedicine
The goal of modern medicine
is no longer merely treatment
of sickness.
Prevention of disease
Promotion of health
Improvement of the quality
of life (individuals, groups or
communities.).
16
It is also
regarded as an
essential
component of
socio-economic
development
17.
“Primitive medicine: Supernaturaltheory of
disease
17
It is thus obvious that medicine in the prehistoric times
(about 5000 B.C.) was intermingled with superstition,
religion, magic and witchcraft.
Medicine was conceived in sympathy and born out of
necessity
The medicine he practiced consisted in appeasing gods by
prayers, rituals and sacrifices, driving out "evil spirits" from
the human body by witchcraft and other crude means
18.
18
The supernatural theoryof disease is as new as
today. For example, in India, one may still hear
the talk of curing snake bites by "mantras
19.
19
Traditional healers" arefound everywhere.
They live close to the people and their
treatments are based on various
combinations of religion, magic and
empiricism.
20.
Chinese medicine(2700 B.C.)
Chinese medicine claims to be the world's
first organized body of medical knowledge
dating back to Hygiene, dietetics,
hydrotherapy, massage, drugs were all used
by the Chinese physicians.
The Chinese were early pioneers of
immunization
20
21.
To a Chinese,"the great doctor is one who
treats not someone who is already ill but
someone not yet ill".
The Chinese have great faith in their
traditional medicine, which is fully integrated
with modern medicine.
21
22.
Egyptian medicine (2000B.C)
Egypt had one of the oldest civilizations
the art of medicine was mingled with religion.
Egyptian physicians were co-equals of
priests, trained in schools within the temples.
22
Specialization prevailed in Egyptian times eye
doctors, head doctors and tooth doctors. All
these doctors were officials paid by the State
23.
Egyptian medicinewas far from primitive.
They believed in pathological nature of
disease
They believed that the pulse was "the speech
of the heart".
Different modalities of treatment like enema,
blood-letting and a wide range of drugs were
used
Egyptians are to be considered the "the best
of all" the ancient doctors
24.
In therealm of public health also, the Egyptians
excelled. They built planned cities, public baths
and underground water supply.
They had also some knowledge of inoculation
against smallpox, the value of mosquito nets and
the association of plague with rats.
24
25.
Mesopotamian medicine
Inancient Mesopotamia, the basic concepts of
medicine were religious, and taught and practiced
by herb doctors, knife doctors and spell doctors -
a classification that roughly parallels our own
internists, surgeons and psychiatrists.
Prescriptions were written on tablets, in
cuneiform writing.
25
26.
the "Hippocratic oath"
hasbecome the keystone
of medical ethics.
Greek medicine (460- 136 B.C
Civilizers of the ancient world.
They taught men to think in terms
of 'Why' and 'How”
They gave rise to dynasties of
healers (curative medicine) and
hygienists (preventive medicine)
with different philosophies.
By far the greatest physician in
Greek medicine was Hippocrates
(460-370 B.C.) who is often
called the "Father of Medicine
26
27.
Greeks gave anew direction to medica thought. They
rejected the supernatural theory of diseas• and looked
upon disease as a natural process
Hippocrates was also an Epidemiologist. He
distinguished between epidemic and endemic,
He studied such things as climate, water, clothing
diet, habits of eating and drinking and stressed the
relation between man and his environment.
27
28.
28
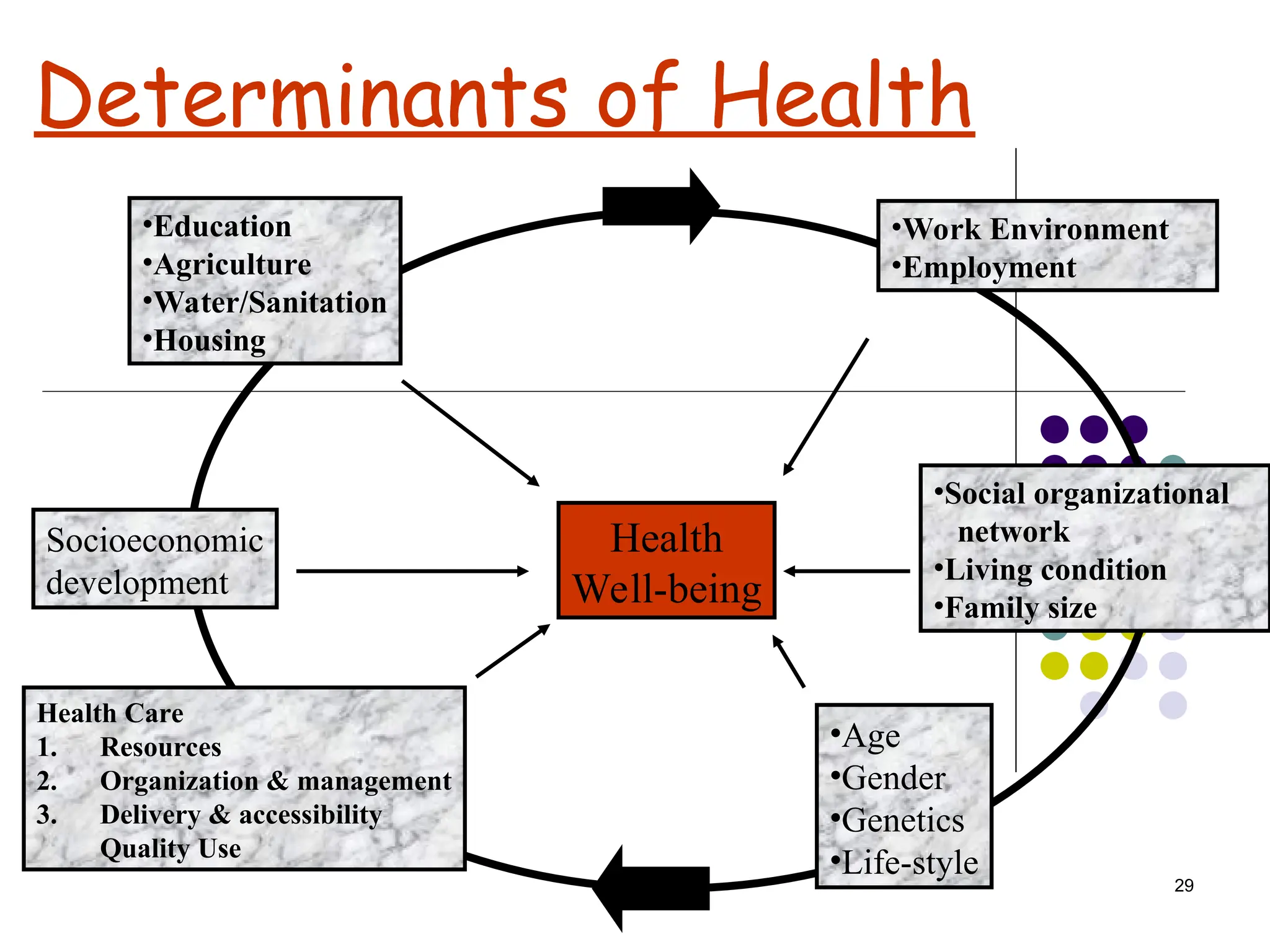
Health
A state ofcomplete physical,
mental and social well-being and
not merely the absence of disease
and infirmity.
31
4. Winslow’s 1923Definition of Public
Health adapted by WHO (1952)
Winslow Definition
The science and art of preventing disease, prolonging life
and promoting physical and mental health and efficiency
through the organized community efforts for the sanitation
of environments,the control of communicable infection, the
education of the individual in personal hygiene, the
organization of medical and nursing services for the early
diagnosis and preventive treatment of disease and the
development of social machinery to ensure to every
individual a standard of living adequate for the
maintenance of health, so organizing these benefits as to
enable every citizen to realize his birth right of health and
longevity.
32.
32
5. Basic HealthServices (1953)
Maternal and child health
communicable disease control
Environmental sanitation
Maintenance of record for
statistical purposes
Health education of the public
Public health nursing
Medical care
33.
33
6. BHORE COMMITTEE(1946)
No individual should be left out.
Fully developed health services.
Concept of health promotion.
As close to people as possible.
Involvement of the people.
34.
34
7. New publichealth (1977-78)
Primary Health Care has
absorbed all the concepts of
basic health services but stressed
community participation and
political will as additional
criteria for action towards
achieving health for all.
35.
35
New Public HealthApproach
The principles of good health are:
Equitable access to effective care
Health friendly public policy based on
community participation
Intersectoral collaboration
Supportive environment
Personal skill development
36.
36
New Public HealthApproach
(Renaissance)
The idea that living conditions (physical social
and economic environment) are the main
determinants of health. Health services are
important but new public health focuses on
changing the determinants rather than
providing treatment for the sick.
37.
37
Upstream Thinking
The lifesavers save the
drowning people and resuscitate
them after the casualty but
sensible decision would be to go
upstream and see why people
fall into the river.
40
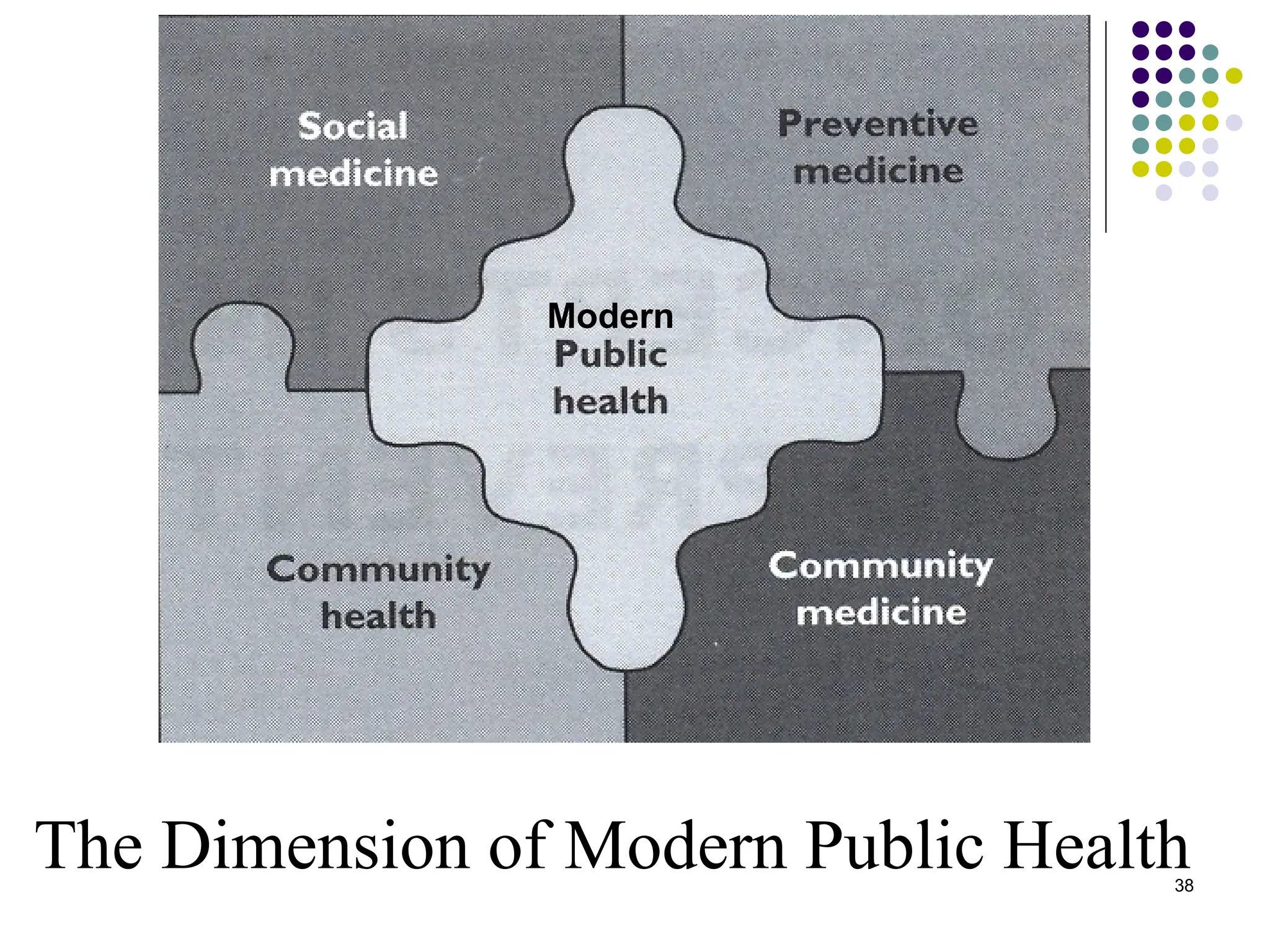
SOCIAL MEDICINE
• SocialMedicine is the study of man in his
total environment, physical, biological and
socioeconomic. It is concerned not only with
curative medicine, but also with health
promotion and prevention. It is concerned
with factors that influence the utilization and
effectiveness of the health and health related
services.
41.
41
COMMUNITY HEALTH
• Communityhealth deals with the services that
aim at protecting the health of the community.
The interventions vary from environmental
sanitation including vector control to personal
health care, immunization, health education
and such like. It includes an important
diagnostic element – community diagnosis –
aimed at surveying and monitoring
community health needs and assessing the
impact of interventions.
42.
42
COMMUNITY MEDICINE
Asystem of delivery of comprehensive health-
care to the people by a health team in order to
improve the health of the community.
43.
43
KEY PUBLIC HEALTHFUNCTIONS
Public health services perform a wide
range of functions, which can be classified
as four key elements:
2.Planning, implementing and evaluating public health
programme
1.Assessing and monitoring of the health of the
population
3.Identifying and dealing with environmental hazards
4.Communicating with people and organizations to
promote public health
46
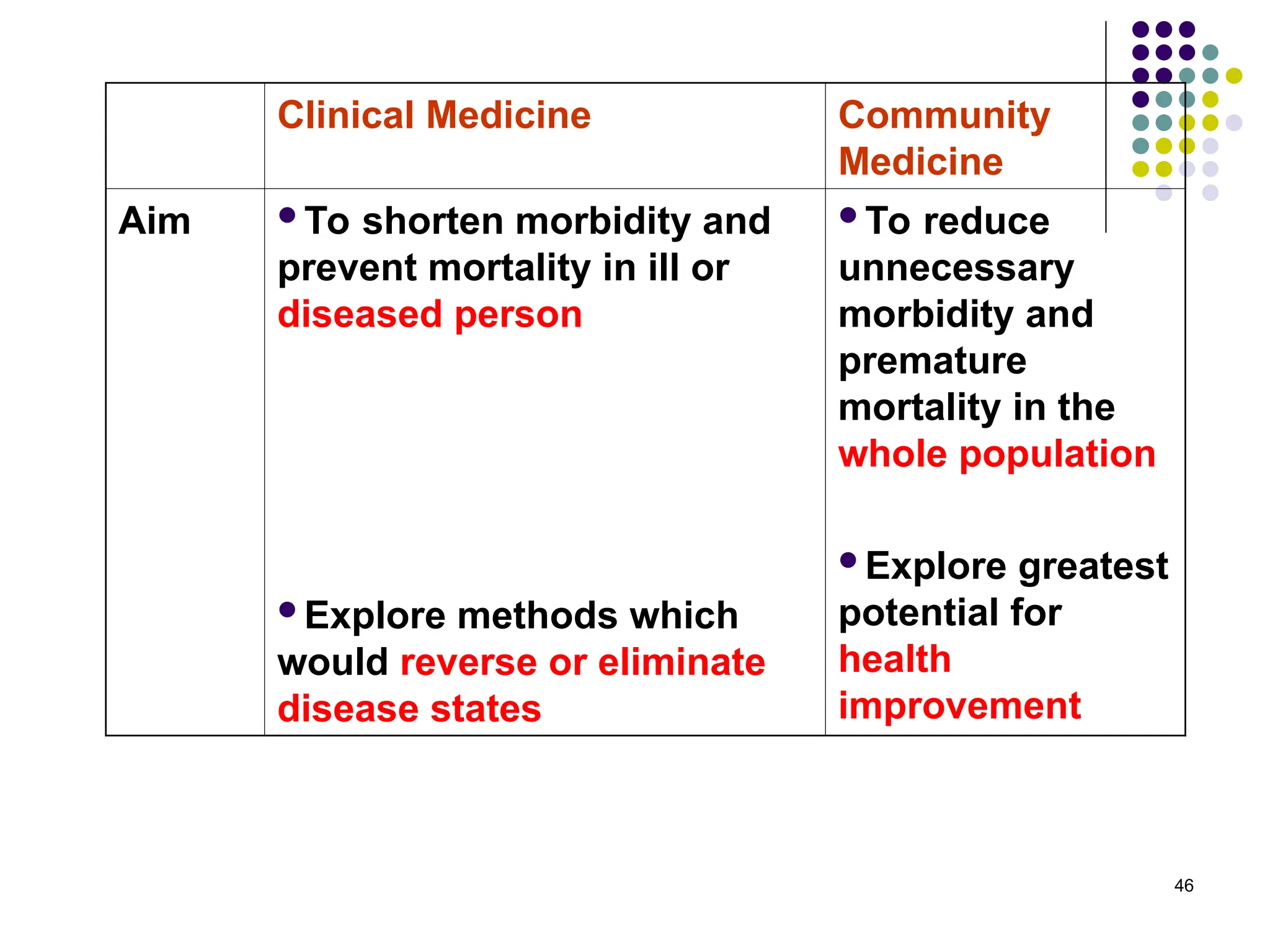
Clinical Medicine Community
Medicine
AimTo shorten morbidity and
prevent mortality in ill or
diseased person
Explore methods which
would reverse or eliminate
disease states
To reduce
unnecessary
morbidity and
premature
mortality in the
whole population
Explore greatest
potential for
health
improvement
47.
47
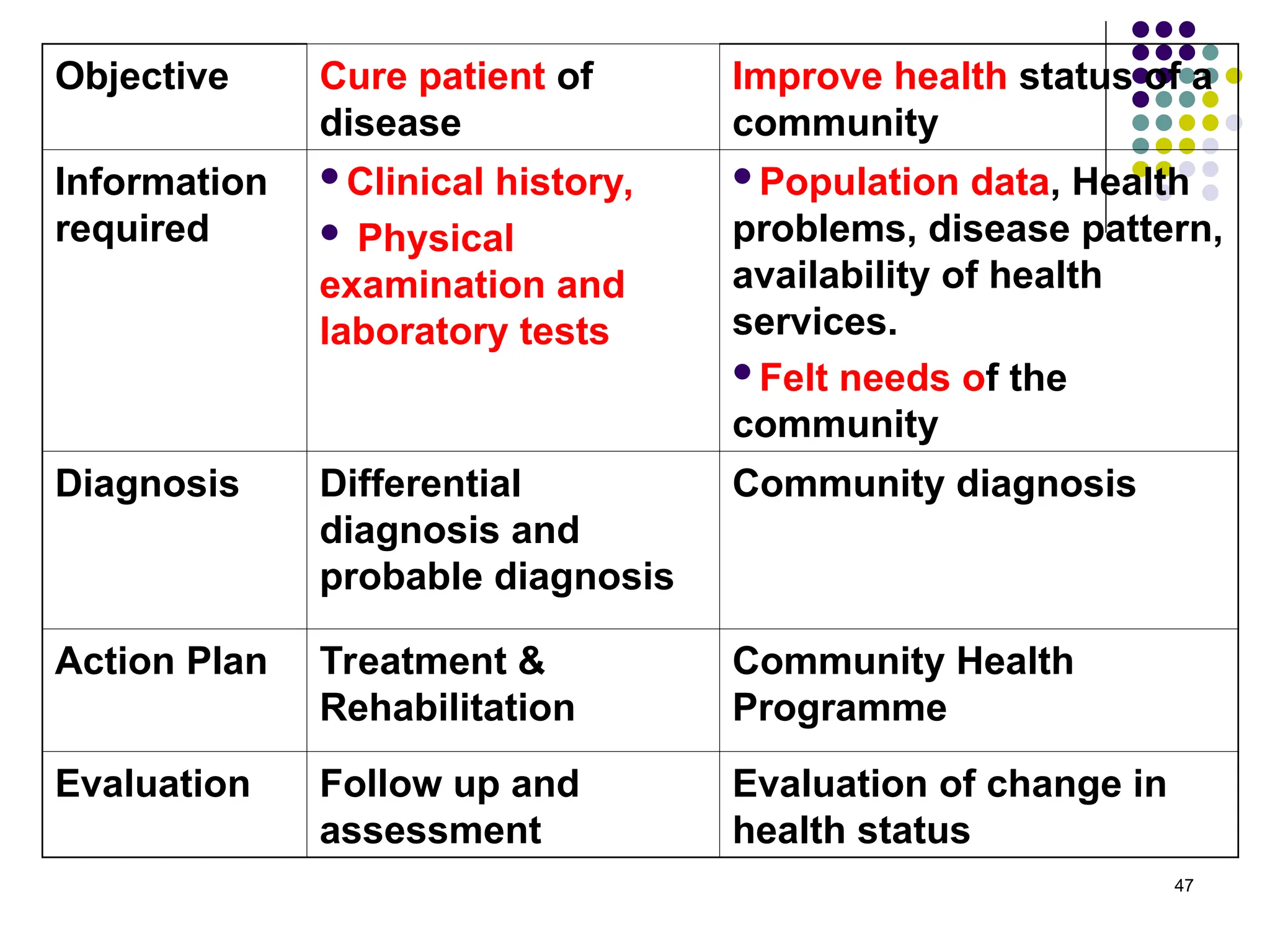
Objective Cure patientof
disease
Improve health status of a
community
Information
required
Clinical history,
Physical
examination and
laboratory tests
Population data, Health
problems, disease pattern,
availability of health
services.
Felt needs of the
community
Diagnosis Differential
diagnosis and
probable diagnosis
Community diagnosis
Action Plan Treatment &
Rehabilitation
Community Health
Programme
Evaluation Follow up and
assessment
Evaluation of change in
health status