Levosimendan is afirst-line drug in the management
of acute heart failure ?
or
in some types of AHF ?
„ Background for the debate ?
1. Introduction of a new drug with a novel mechanism of
action ( discrepancy between clinical trial results )
2. Lack of consensus about the definition and
management of AHF
3. Old dogma „ inotropes are bad“ in heart failure !
Arguments PRO
F. Follath, Zürich
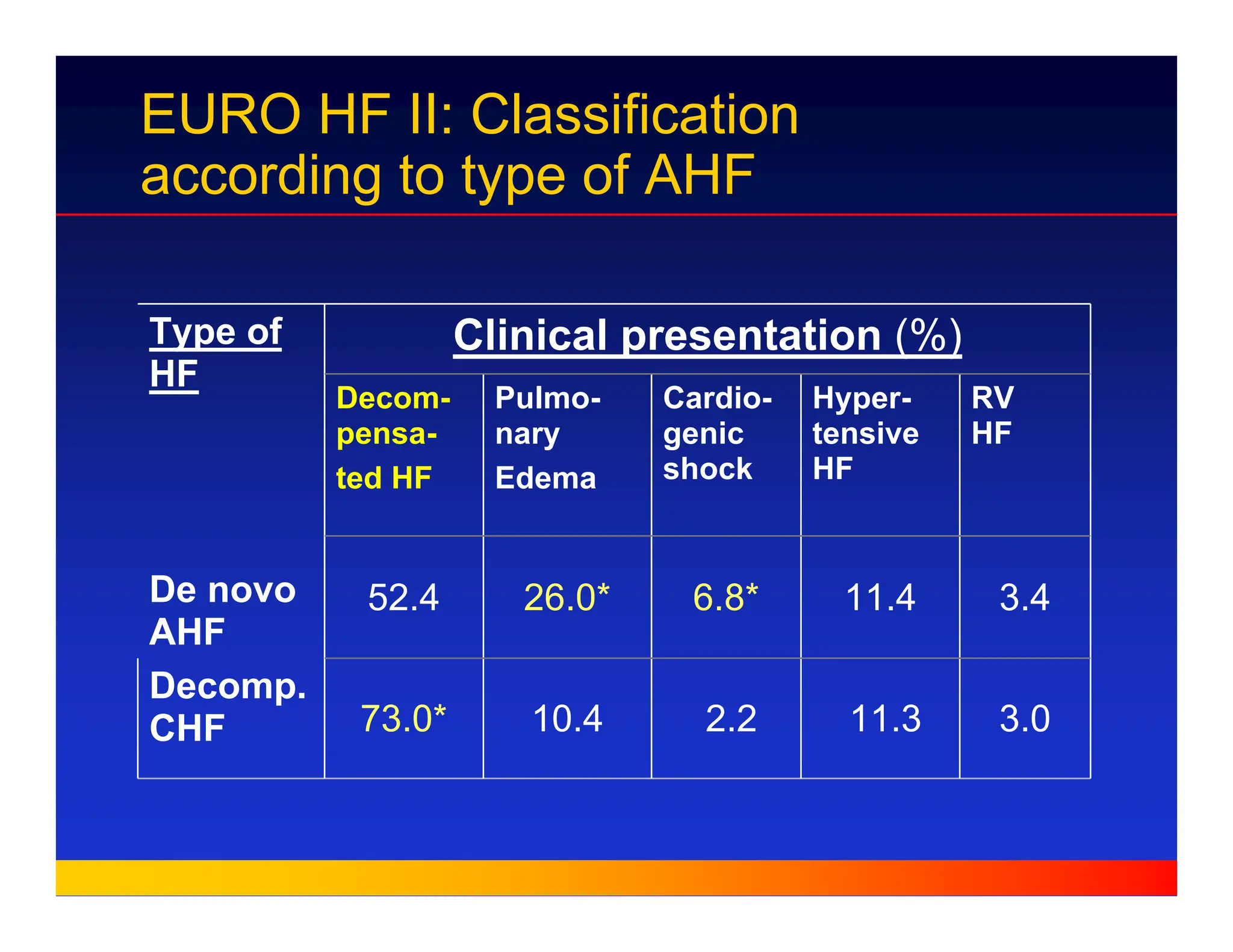
EURO HF II:Classification
according to type of AHF
3.0
11.3
2.2
10.4
73.0*
Decomp.
CHF
3.4
11.4
6.8*
26.0*
52.4
RV
HF
Hyper-
tensive
HF
Cardio-
genic
shock
Pulmo-
nary
Edema
Decom-
pensa-
ted HF
Clinical presentation (%)
Type of
HF
De novo
AHF
4.
European experience with
Levosimendan
-Well documented haemodynamic efficacy and good
tolerance ( LIDO and dose finding studies) )
- Improved survival at 30 and 180 days (LIDO,RUSSLAN)
- Post-marketing Studies:
PORTLAND - clinical efficacy & no AE in 80%
- improved renal function
Routine clinical use in several countries ( Sweden, Finland,
Austria, Greece, Italy, Portugal , Spain )
5.
Inclusion Criteria /LIDO
„ EF 35% (determined 1 month prior to study)
„ CI <2.5 L/m2/min and mean PCWP >15 mmHg
Mean(SD) values: C.I. 1.94 (0.36) L/min/m2
PCW 25 (8) mmHg
„ Clinical need for i.v. treatment with positive inotropic agents.
Patient categories:
– Severe chronic HF, clinical condition deteriorating despite
optimal oral therapy ( Dobut. 92%, Levo 84%)
– Acute HF related to recent onset of cardiac or non-cardiac
conditions
– Severe HF after cardiac surgery
6.
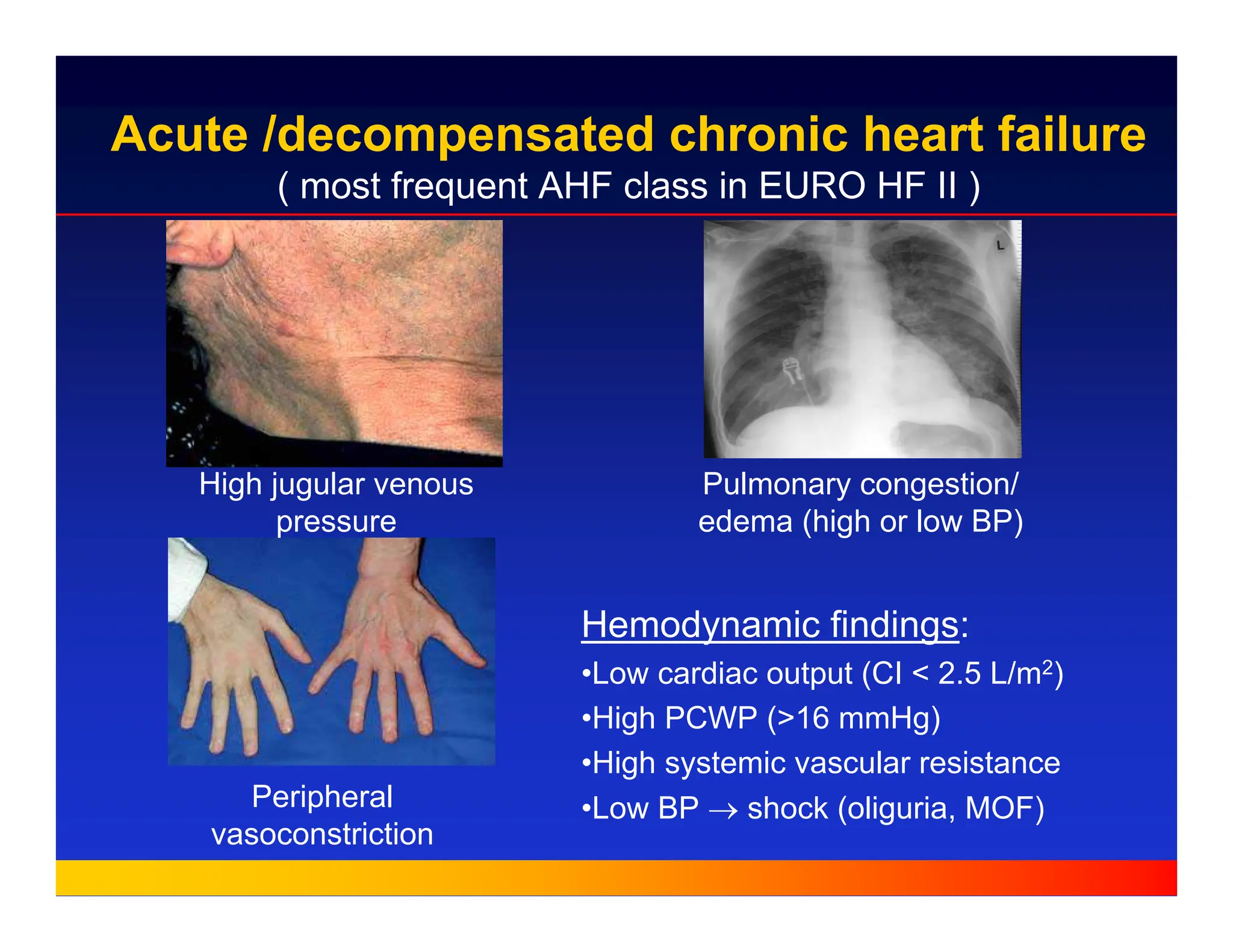
Acute /decompensated chronicheart failure
( most frequent AHF class in EURO HF II )
High jugular venous
pressure
Peripheral
vasoconstriction
Pulmonary congestion/
edema (high or low BP)
Hemodynamic findings:
•Low cardiac output (CI < 2.5 L/m2)
•High PCWP (>16 mmHg)
•High systemic vascular resistance
•Low BP → shock (oliguria, MOF)
7.
Exclusion criteria
„ Chestpain at randomisation ( acute CAD)
„ VT or VF within previous 2 weeks
„ Systolic BP < 85 mmHg
„ i.v. beta-adrenergic drugs (< 30 min.)
„ i.v. vasodilators (< 2 hours )
„ i.v. milrinone or enoximone (< 12 hours)
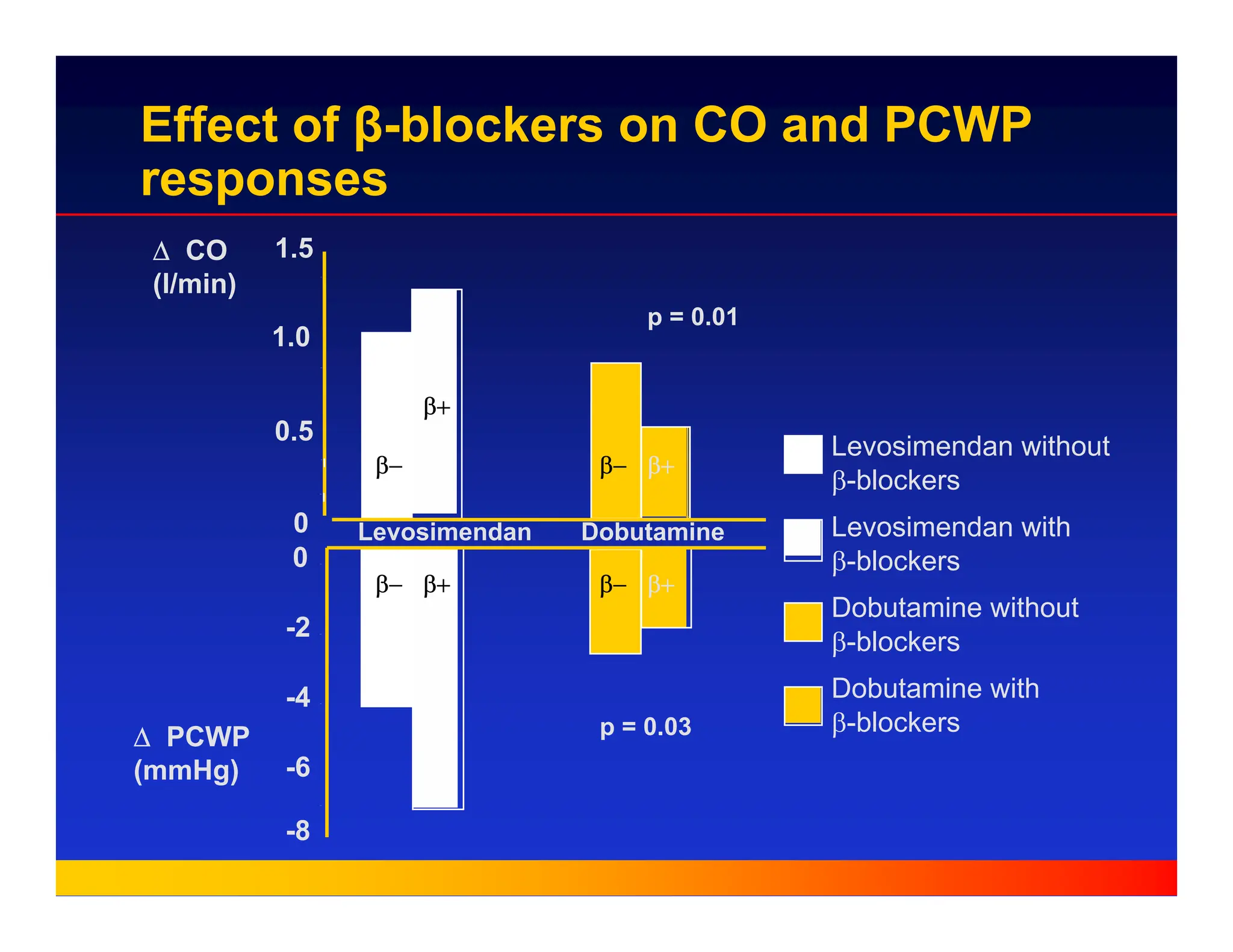
Effect of β-blockerson CO and PCWP
responses
∆ CO
(l/min)
∆ PCWP
(mmHg)
0
0.5
1.0
1.5
Levosimendan without
β-blockers
Levosimendan with
β-blockers
Dobutamine without
β-blockers
Dobutamine with
β-blockers
-8
-6
-4
-2
0
Levosimendan Dobutamine
p = 0.01
p = 0.03
β−
β+
β− β+
β− β+ β− β+
10.
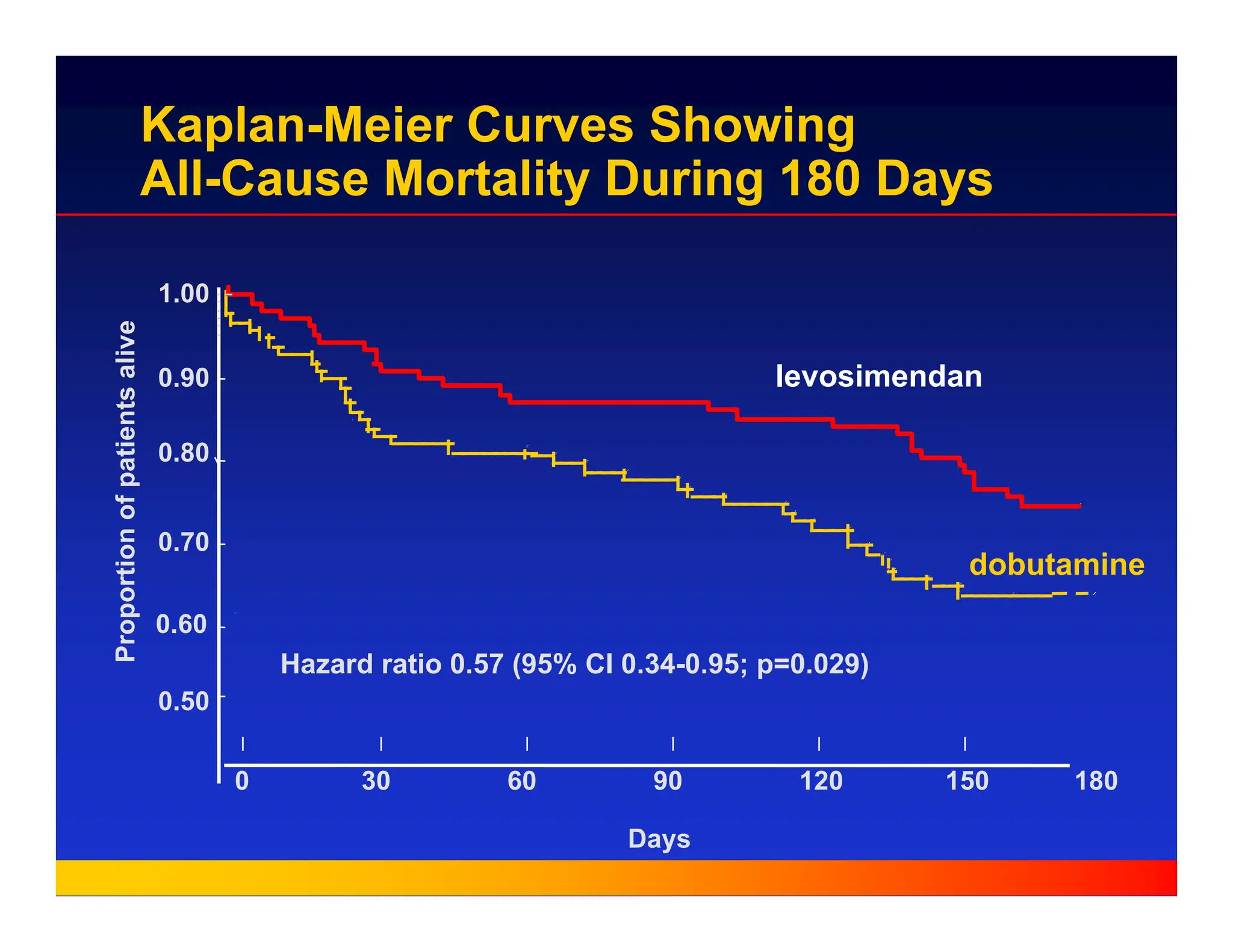
Hazard ratio 0.57(95% CI 0.34-0.95; p=0.029)
1.00
0.90
0.80
0.70
0.60
Days
0.50
Proportion
of
patients
alive
levosimendan
dobutamine
120 150
90
30
0 60 180
Kaplan-Meier Curves Showing
All-Cause Mortality During 180 Days
11.
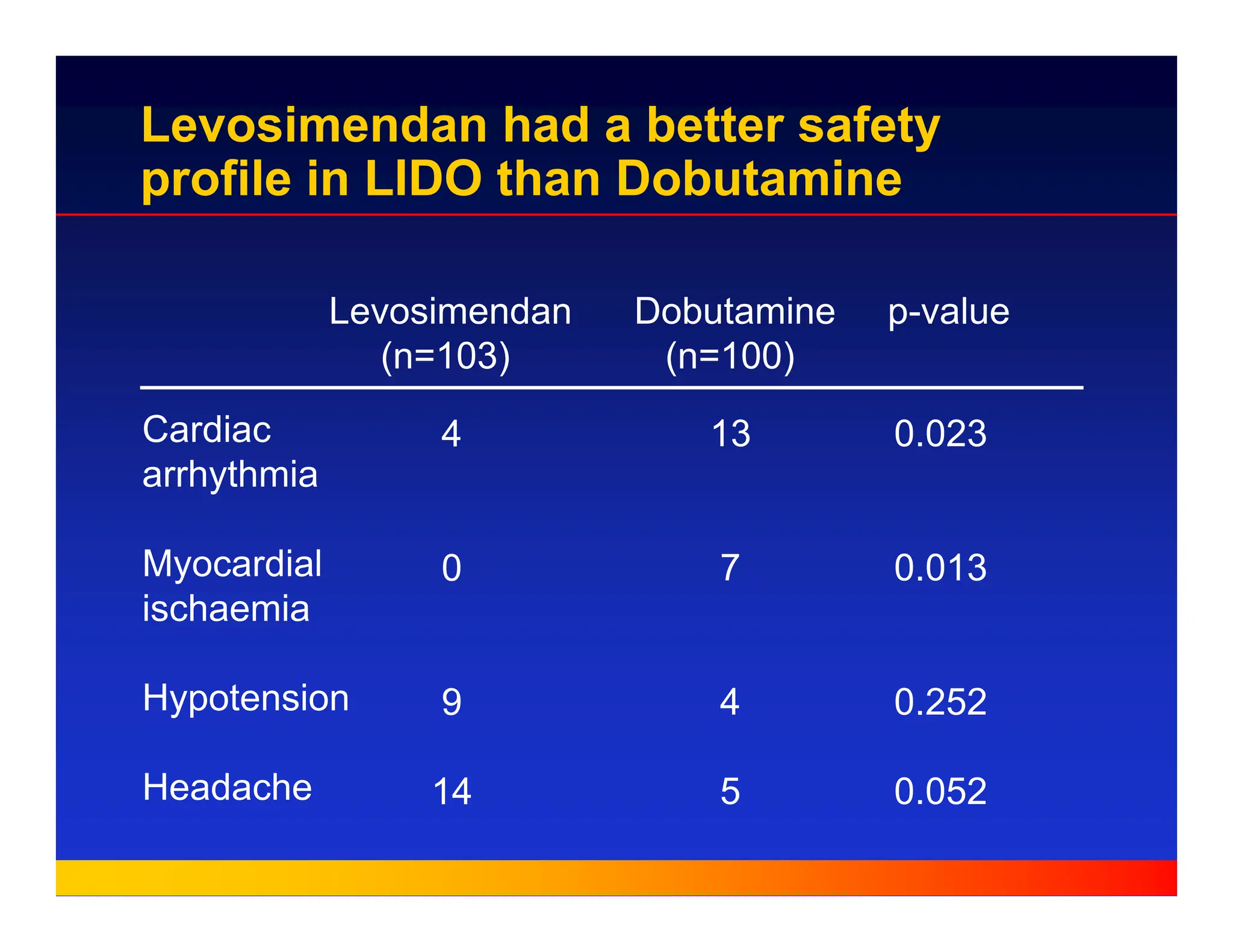
Levosimendan Dobutamine p-value
(n=103)(n=100)
Cardiac
arrhythmia
Myocardial
ischaemia
Hypotension
Headache
4
0
9
14
13
7
4
5
0.023
0.013
0.252
0.052
Levosimendan had a better safety
profile in LIDO than Dobutamine
12.
RUSSLAN
„ Non-invasive safetystudy
„ Heart failure after AMI (clinical & chest x-ray)
„ Multi-centre study in Russia and Latvia
„ n = 504 ( placebo vs. 4 dose levels of
levosimendan )
13.
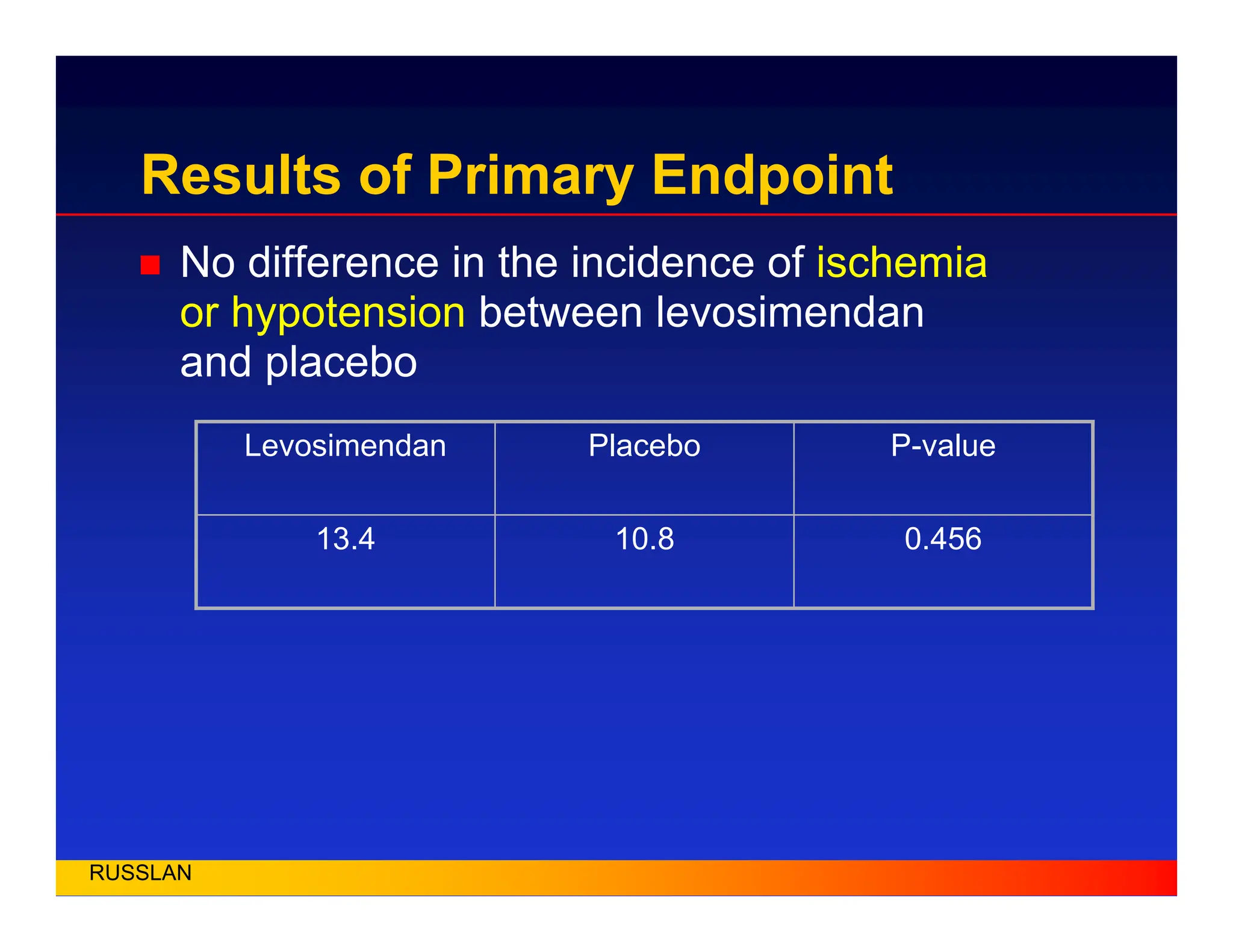
Results of PrimaryEndpoint
„ No difference in the incidence of ischemia
or hypotension between levosimendan
and placebo
RUSSLAN
0.456
10.8
13.4
P-value
Placebo
Levosimendan
14.
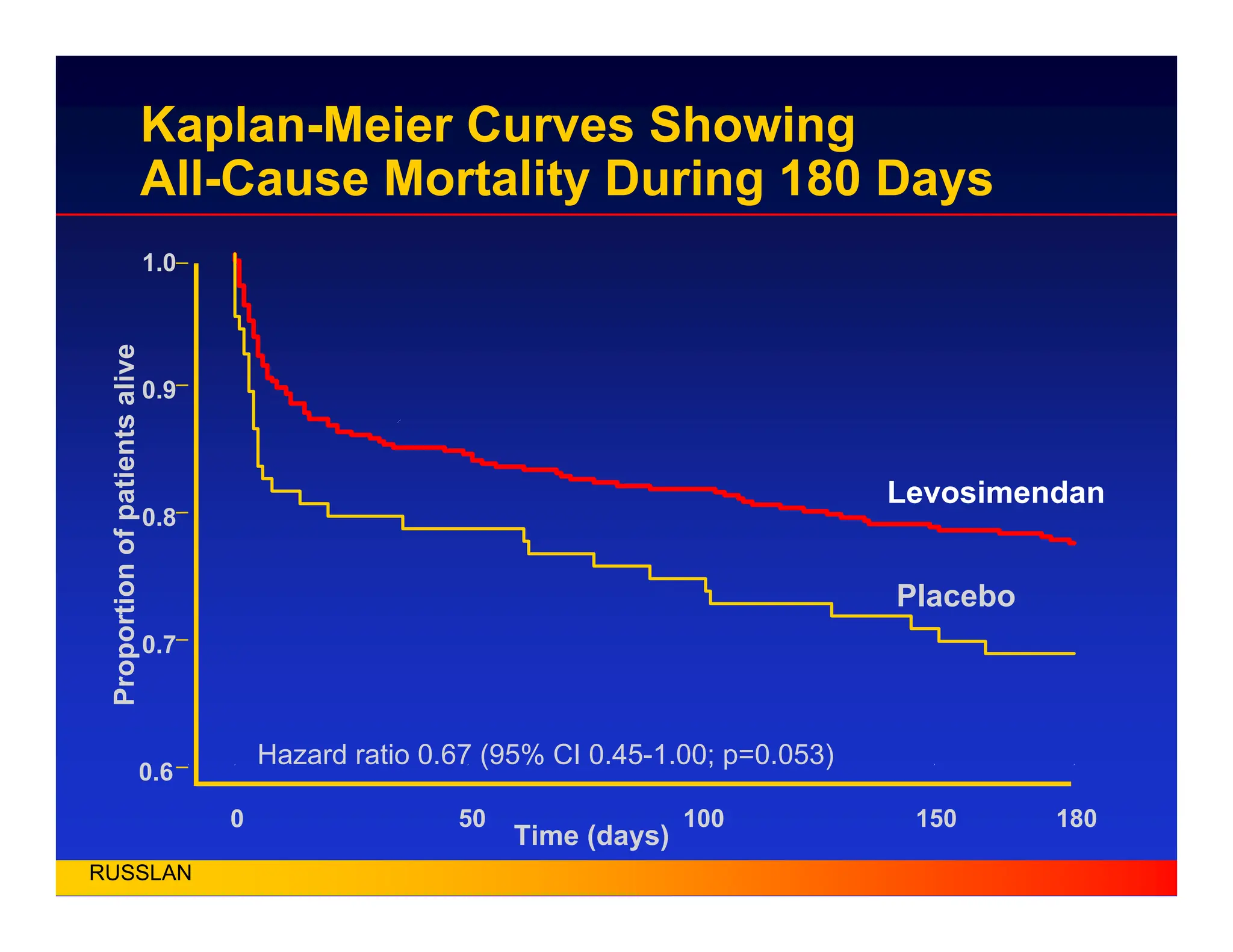
Kaplan-Meier Curves Showing
All-CauseMortality During 180 Days
Time (days)
Proportion
of
patients
alive
0
0.6
0.7
0.8
0.9
1.0
50 100 150 180
Hazard ratio 0.67 (95% CI 0.45-1.00; p=0.053)
Levosimendan
Placebo
RUSSLAN
15.
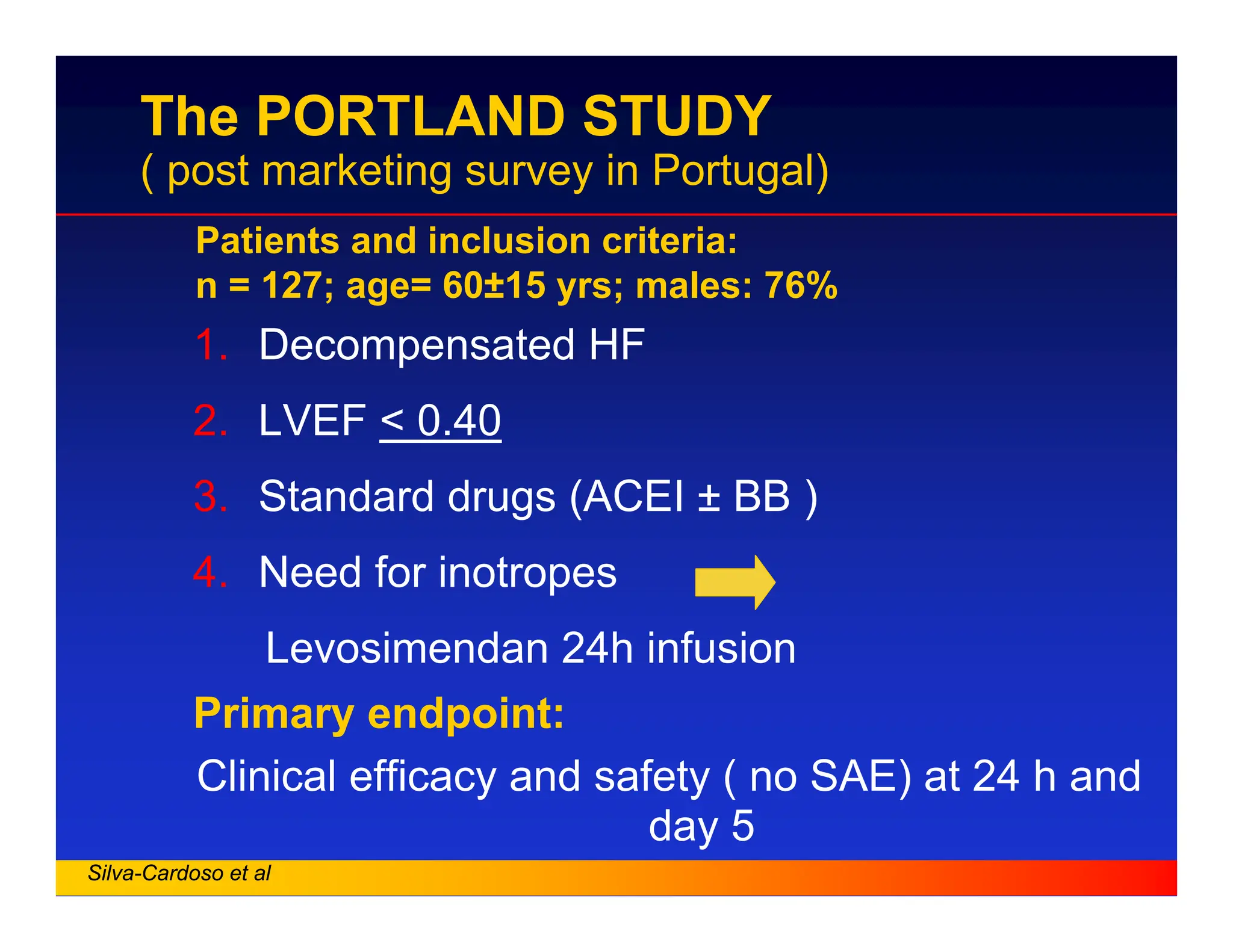
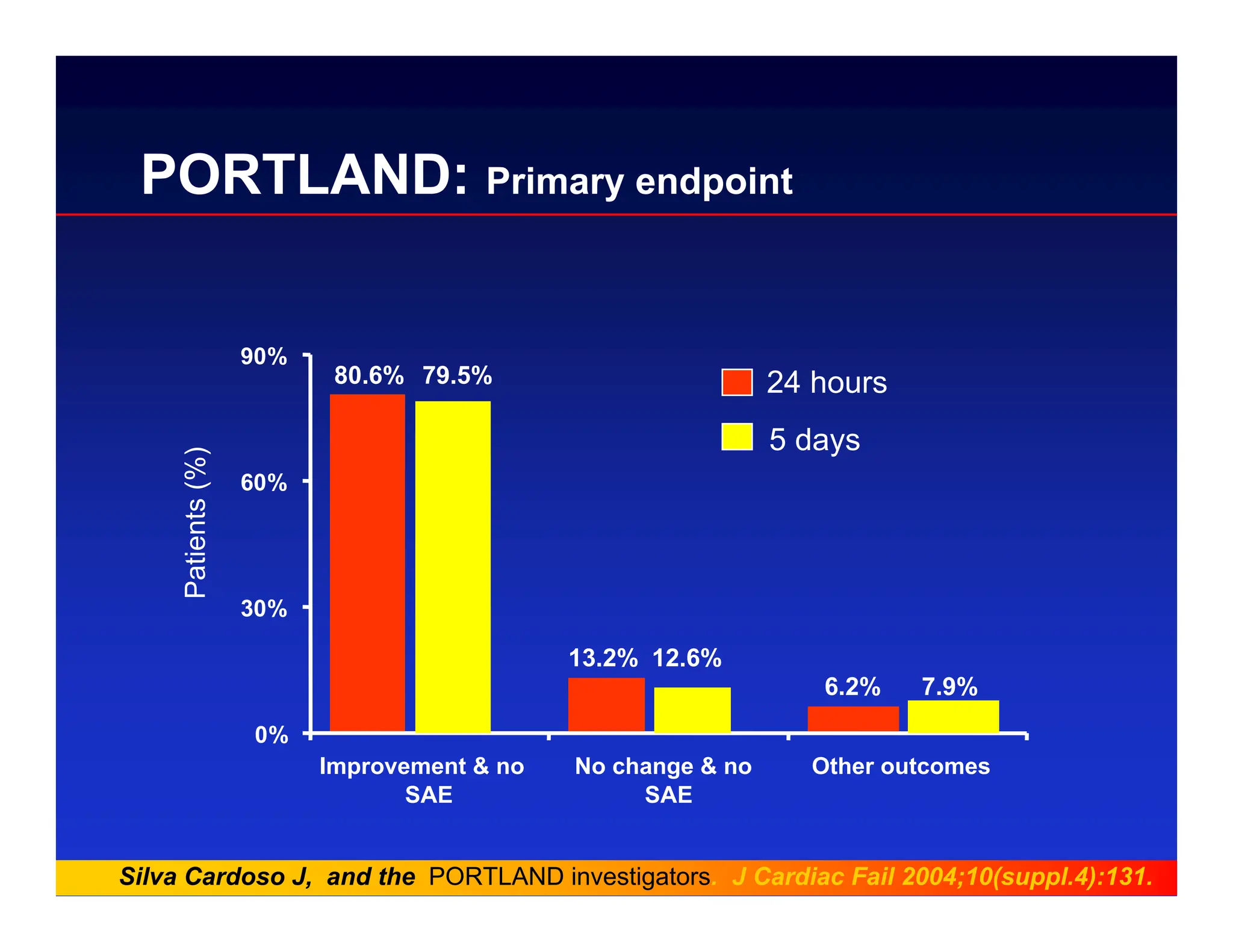
The PORTLAND STUDY
(post marketing survey in Portugal)
1. Decompensated HF
2. LVEF < 0.40
3. Standard drugs (ACEI ± BB )
4. Need for inotropes
Levosimendan 24h infusion
Primary endpoint:
Clinical efficacy and safety ( no SAE) at 24 h and
day 5
Patients and inclusion criteria:
n = 127; age= 60±15 yrs; males: 76%
Silva-Cardoso et al
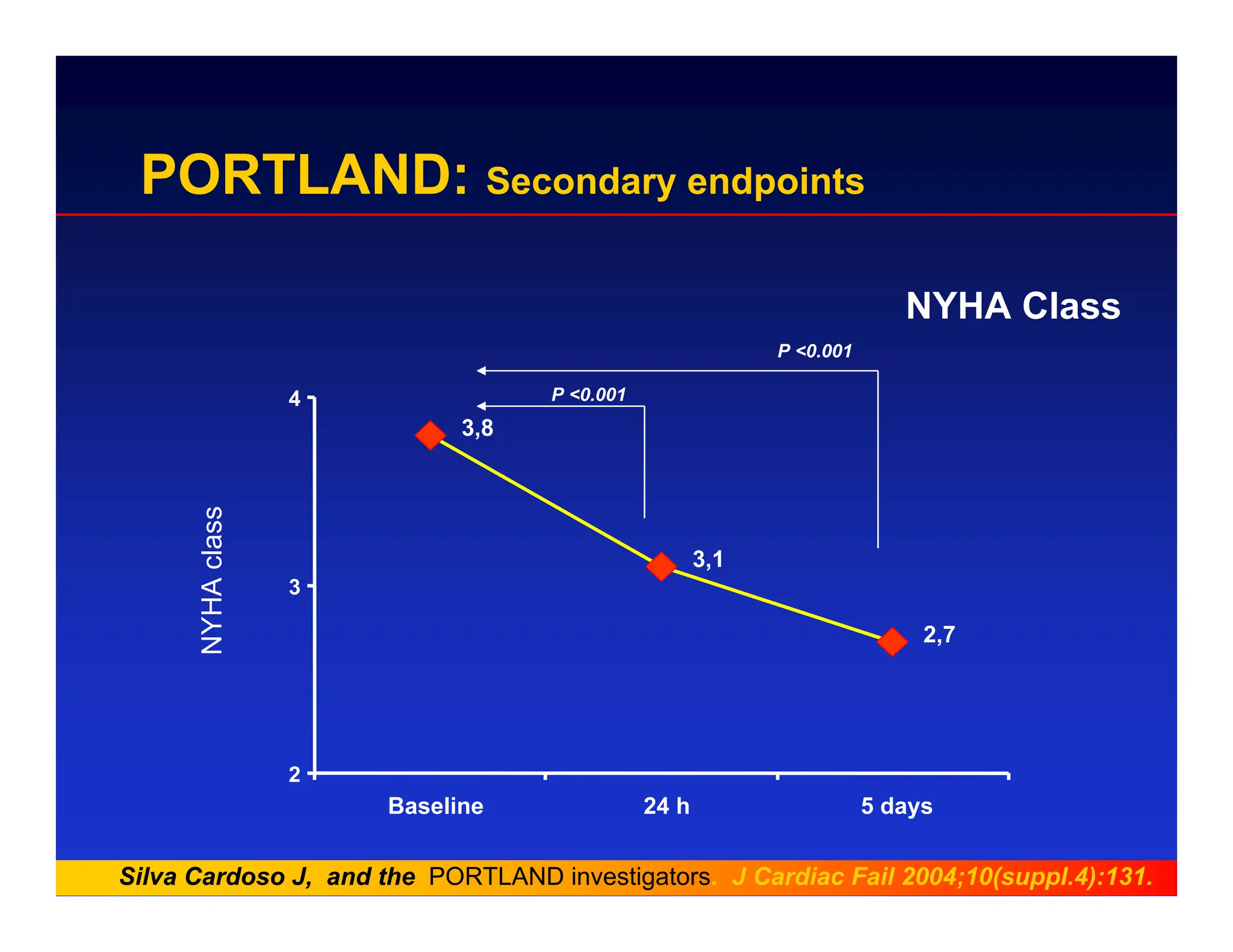
PORTLAND: Secondary endpoints
NYHAClass
NYHA
class
3,8
3,1
2,7
2
3
4
Baseline 24 h 5 days
P <0.001
P <0.001
Silva Cardoso J, and the PORTLAND investigators. J Cardiac Fail 2004;10(suppl.4):131.
19.
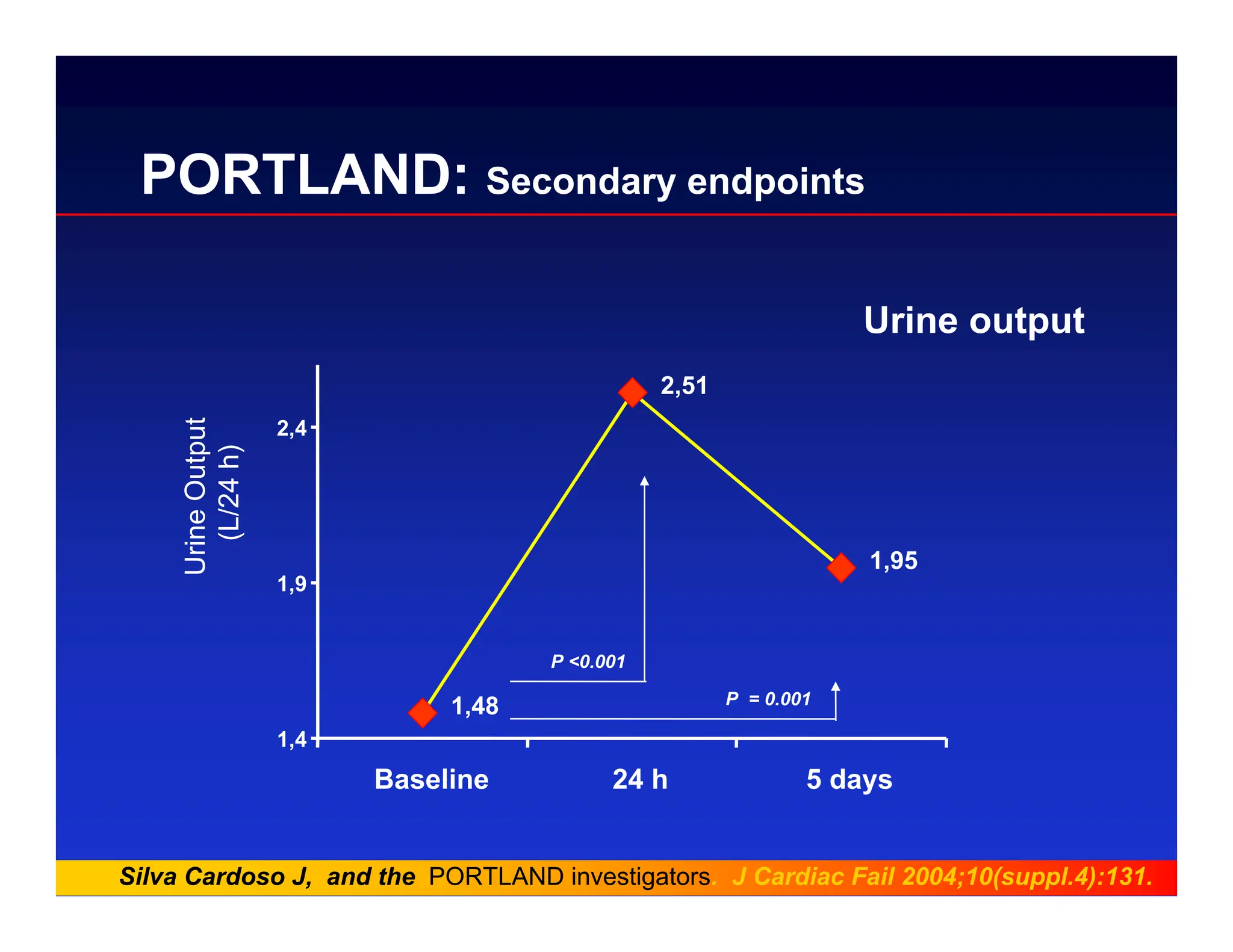
PORTLAND: Secondary endpoints
Urineoutput
1,48
2,51
1,95
1,4
1,9
2,4
Baseline 24 h 5 days
Urine
Output
(L/24
h)
P <0.001
P = 0.001
Silva Cardoso J, and the PORTLAND investigators. J Cardiac Fail 2004;10(suppl.4):131.
20.
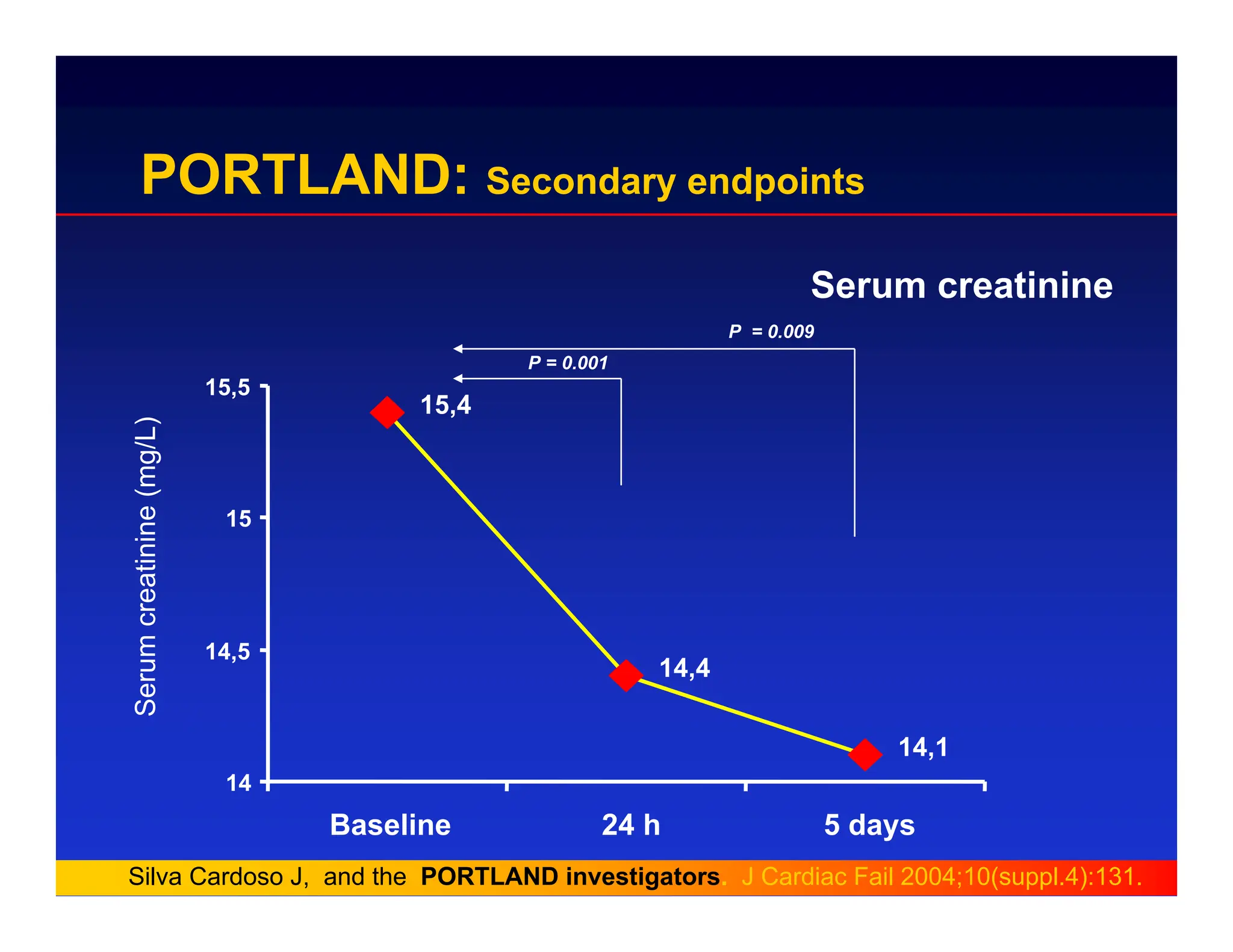
PORTLAND: Secondary endpoints
Serumcreatinine
Serum
creatinine
(mg/L)
15,4
14,4
14,1
14
14,5
15
15,5
Baseline 24 h 5 days
P = 0.001
P = 0.009
Silva Cardoso J, and the PORTLAND investigators. J Cardiac Fail 2004;10(suppl.4):131.
21.
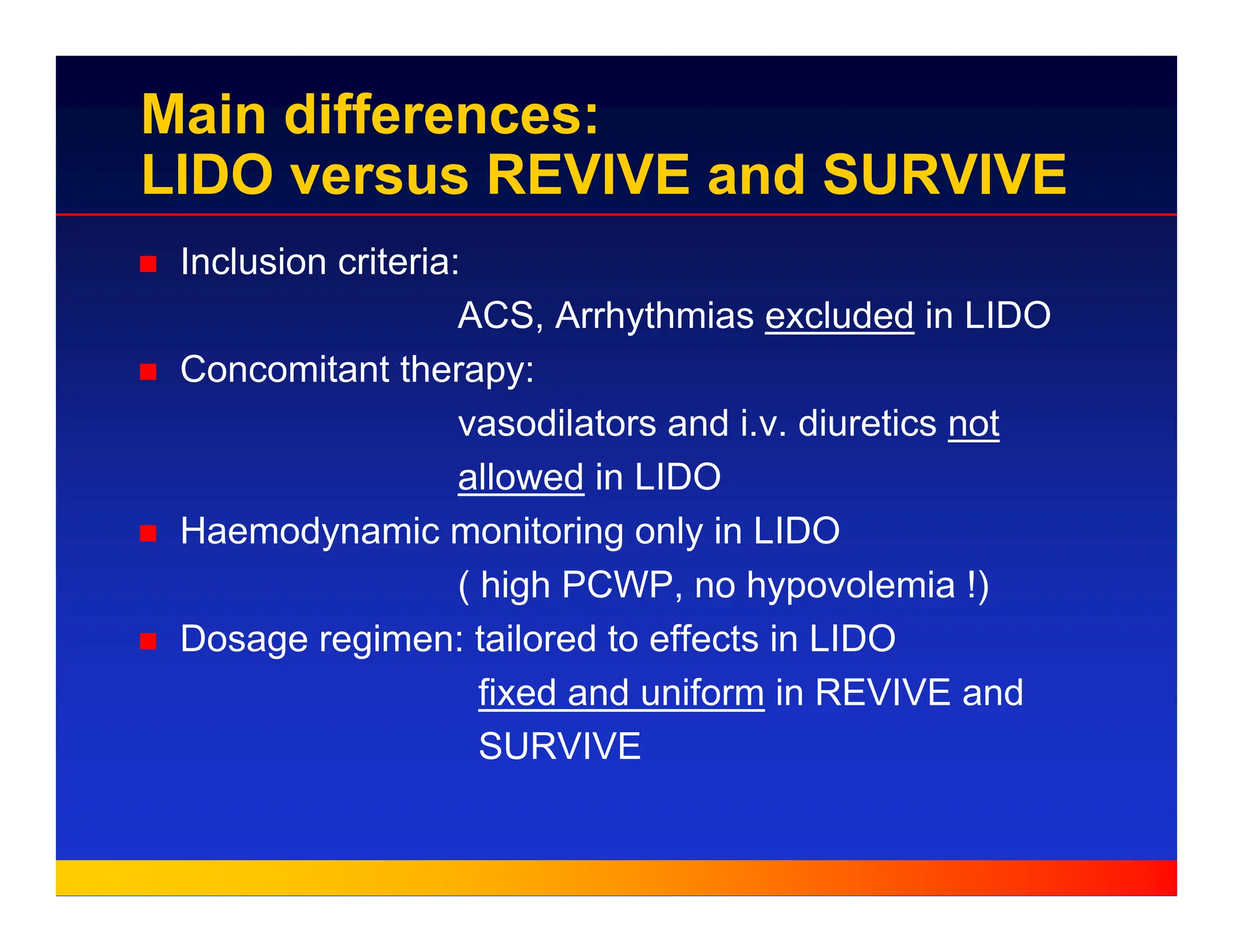
Main differences:
LIDO versusREVIVE and SURVIVE
„ Inclusion criteria:
ACS, Arrhythmias excluded in LIDO
„ Concomitant therapy:
vasodilators and i.v. diuretics not
allowed in LIDO
„ Haemodynamic monitoring only in LIDO
( high PCWP, no hypovolemia !)
„ Dosage regimen: tailored to effects in LIDO
fixed and uniform in REVIVE and
SURVIVE
22.
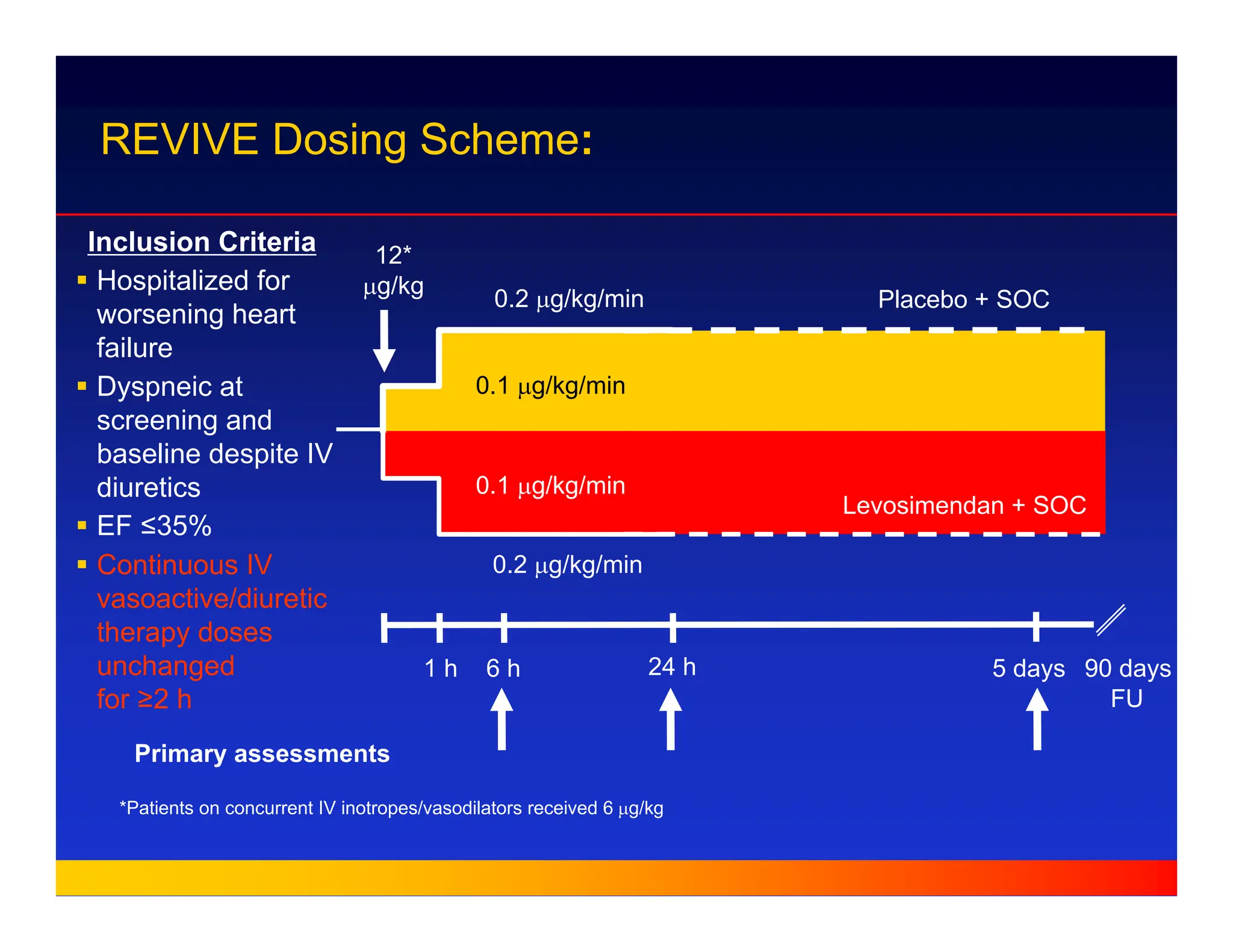
0.1 µg/kg/min
0.1 µg/kg/min
0.2µg/kg/min
0.2 µg/kg/min
Placebo + SOC
Levosimendan + SOC
12*
µg/kg
*Patients on concurrent IV inotropes/vasodilators received 6 µg/kg
REVIVE Dosing Scheme:
1 h 5 days
6 h 24 h
Primary assessments
90 days
FU
Inclusion Criteria
ƒ Hospitalized for
worsening heart
failure
ƒ Dyspneic at
screening and
baseline despite IV
diuretics
ƒ EF ≤35%
ƒ Continuous IV
vasoactive/diuretic
therapy doses
unchanged
for ≥2 h
23.
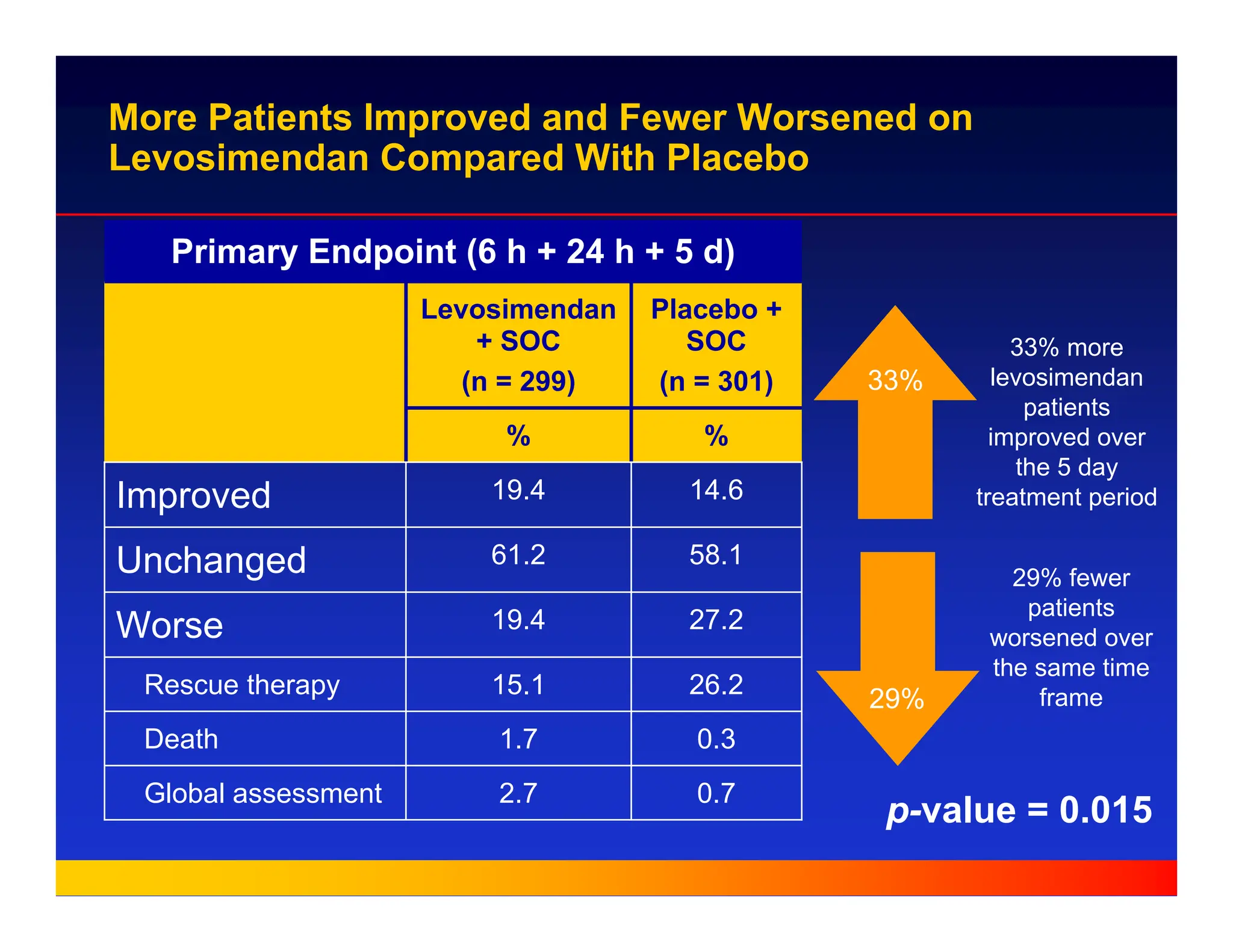
More Patients Improvedand Fewer Worsened on
Levosimendan Compared With Placebo
Primary Endpoint (6 h + 24 h + 5 d)
Placebo +
SOC
(n = 301)
Levosimendan
+ SOC
(n = 299)
26.2
15.1
Rescue therapy
0.7
2.7
Global assessment
%
%
0.3
27.2
58.1
14.6
1.7
19.4
61.2
19.4
Death
Worse
Unchanged
Improved
p-value = 0.015
33% more
levosimendan
patients
improved over
the 5 day
treatment period
29% fewer
patients
worsened over
the same time
frame
33%
29%
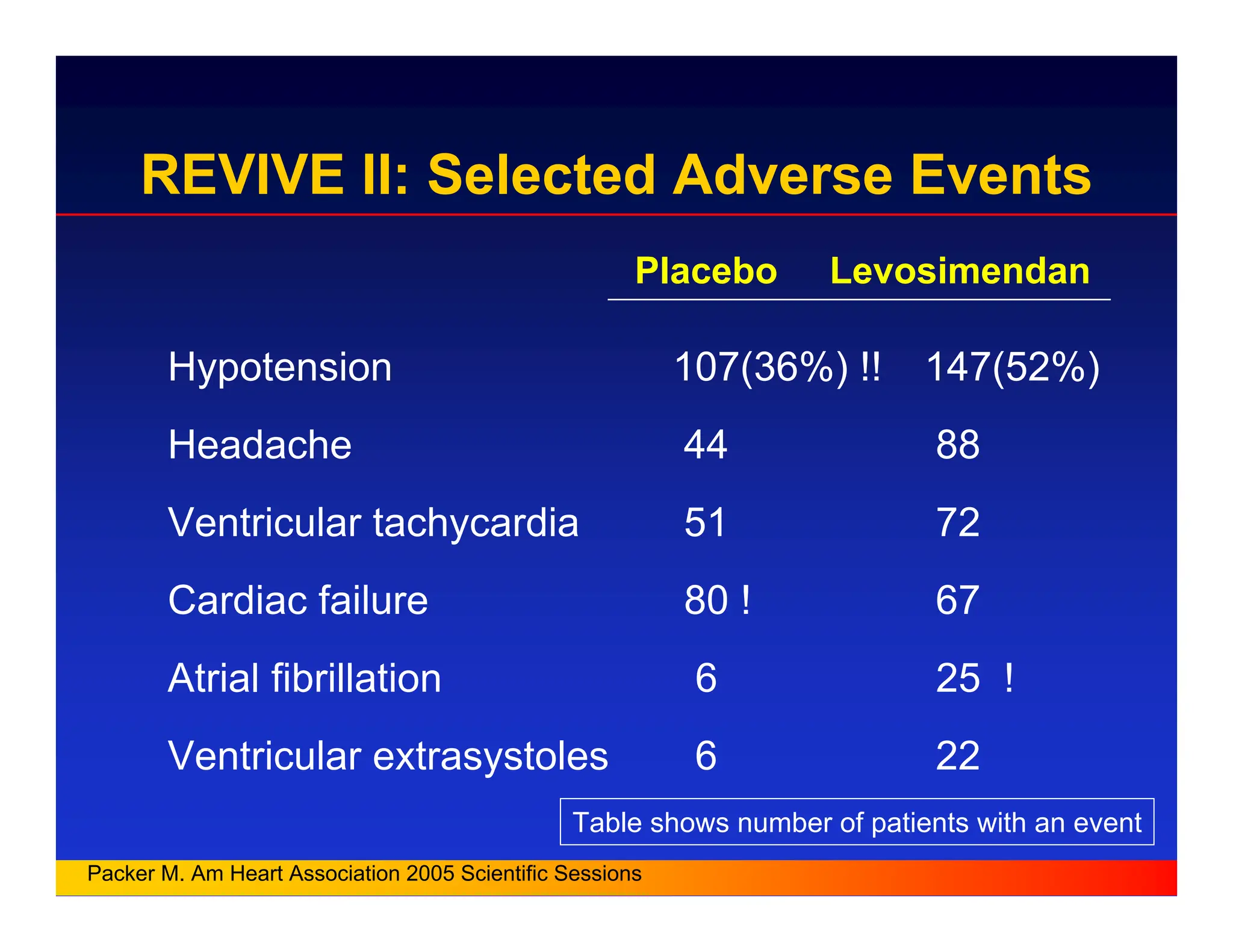
24.
Placebo Levosimendan
Hypotension 107(36%)!! 147(52%)
Headache 44 88
Ventricular tachycardia 51 72
Cardiac failure 80 ! 67
Atrial fibrillation 6 25 !
Ventricular extrasystoles 6 22
Table shows number of patients with an event
Packer M. Am Heart Association 2005 Scientific Sessions
REVIVE II: Selected Adverse Events
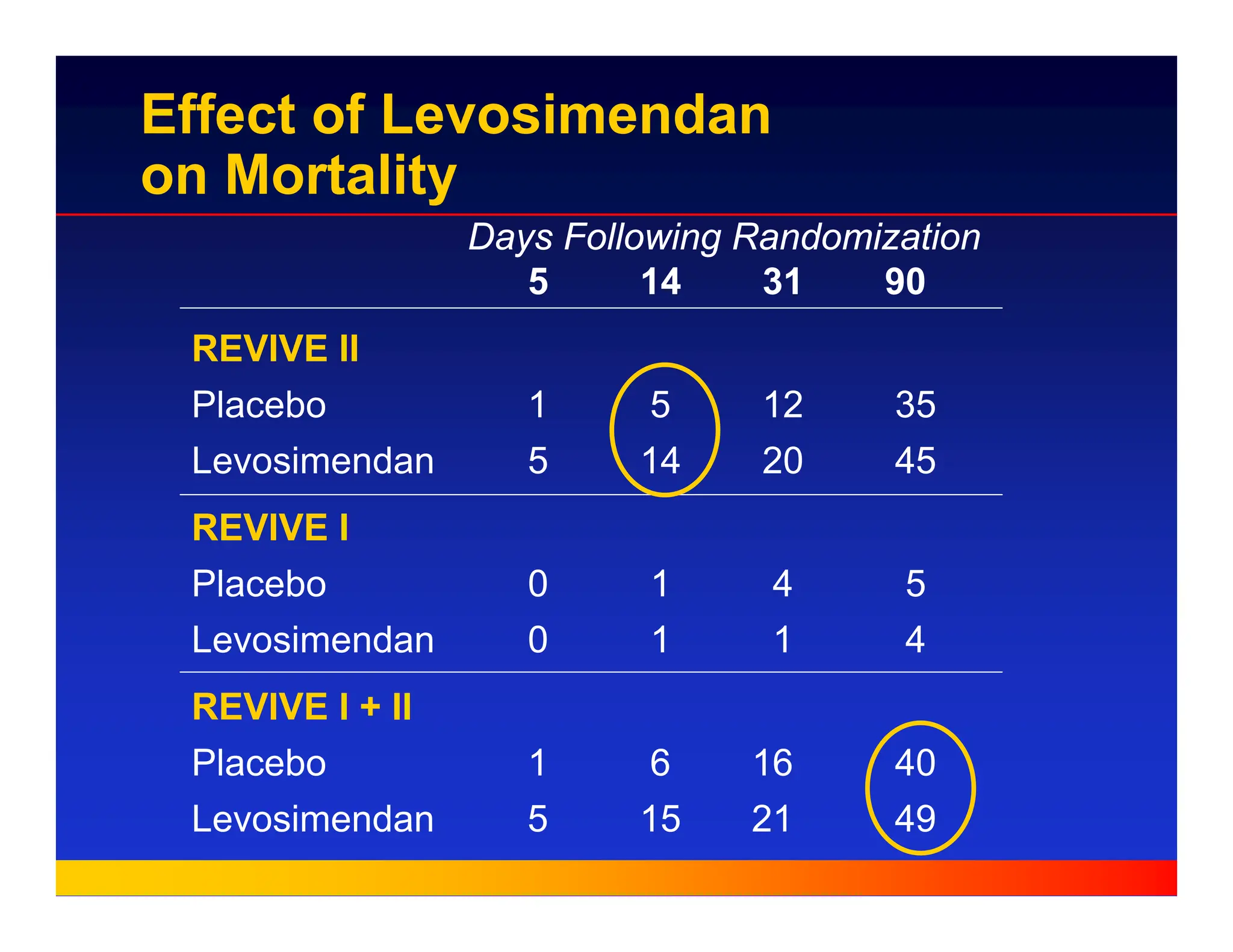
25.
Days Following Randomization
514 31 90
REVIVE II
Placebo 1 5 12 35
Levosimendan 5 14 20 45
REVIVE I
Placebo 0 1 4 5
Levosimendan 0 1 1 4
REVIVE I + II
Placebo 1 6 16 40
Levosimendan 5 15 21 49
Effect of Levosimendan
on Mortality
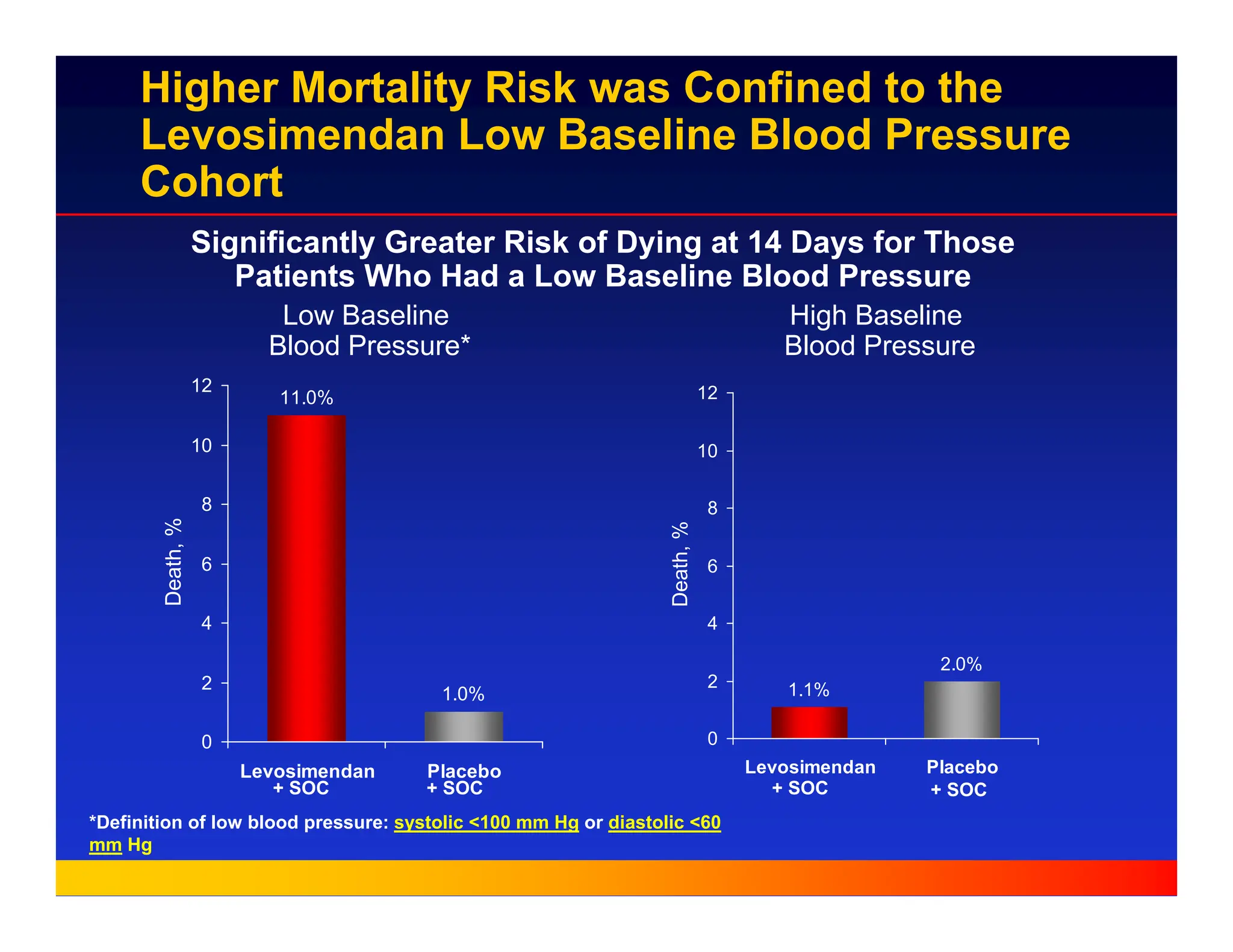
26.
Higher Mortality Riskwas Confined to the
Levosimendan Low Baseline Blood Pressure
Cohort
Significantly Greater Risk of Dying at 14 Days for Those
Patients Who Had a Low Baseline Blood Pressure
11.0%
1.0%
0
2
4
6
8
10
12
Levosimendan Placebo
Death,
%
1.1%
2.0%
0
2
4
6
8
10
12
Levosimendan Placebo
Death,
%
Low Baseline
Blood Pressure*
High Baseline
Blood Pressure
*Definition of low blood pressure: systolic <100 mm Hg or diastolic <60
mm Hg
+ SOC + SOC + SOC + SOC
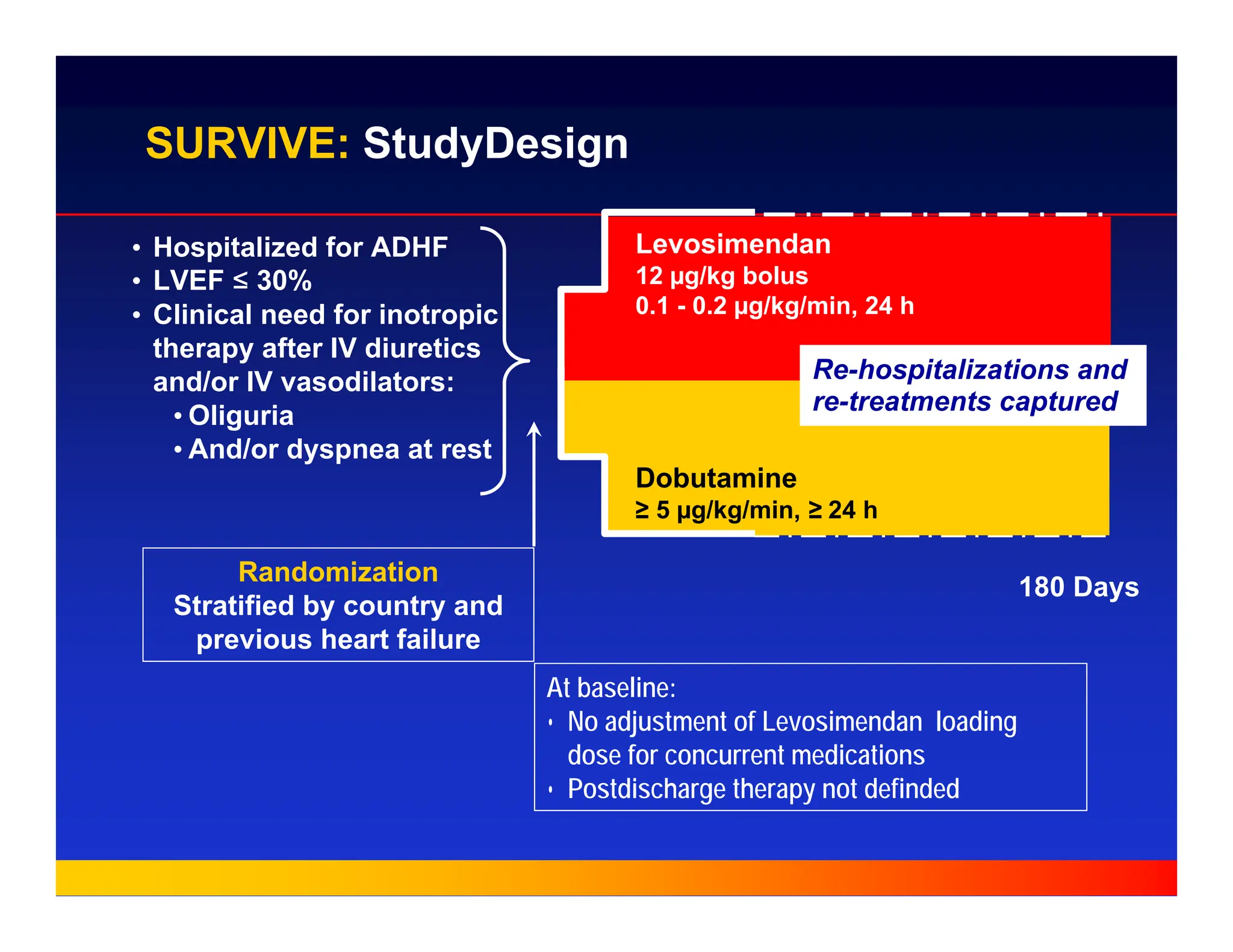
27.
180 Days
SURVIVE: StudyDesign
Levosimendan
12µg/kg bolus
0.1 - 0.2 µg/kg/min, 24 h
Dobutamine
≥ 5 µg/kg/min, ≥ 24 h
Randomization
Stratified by country and
previous heart failure
• Hospitalized for ADHF
• LVEF ≤ 30%
• Clinical need for inotropic
therapy after IV diuretics
and/or IV vasodilators:
• Oliguria
• And/or dyspnea at rest
At baseline:
• No adjustment of Levosimendan loading
dose for concurrent medications
• Postdischarge therapy not definded
Re-hospitalizations and
re-treatments captured
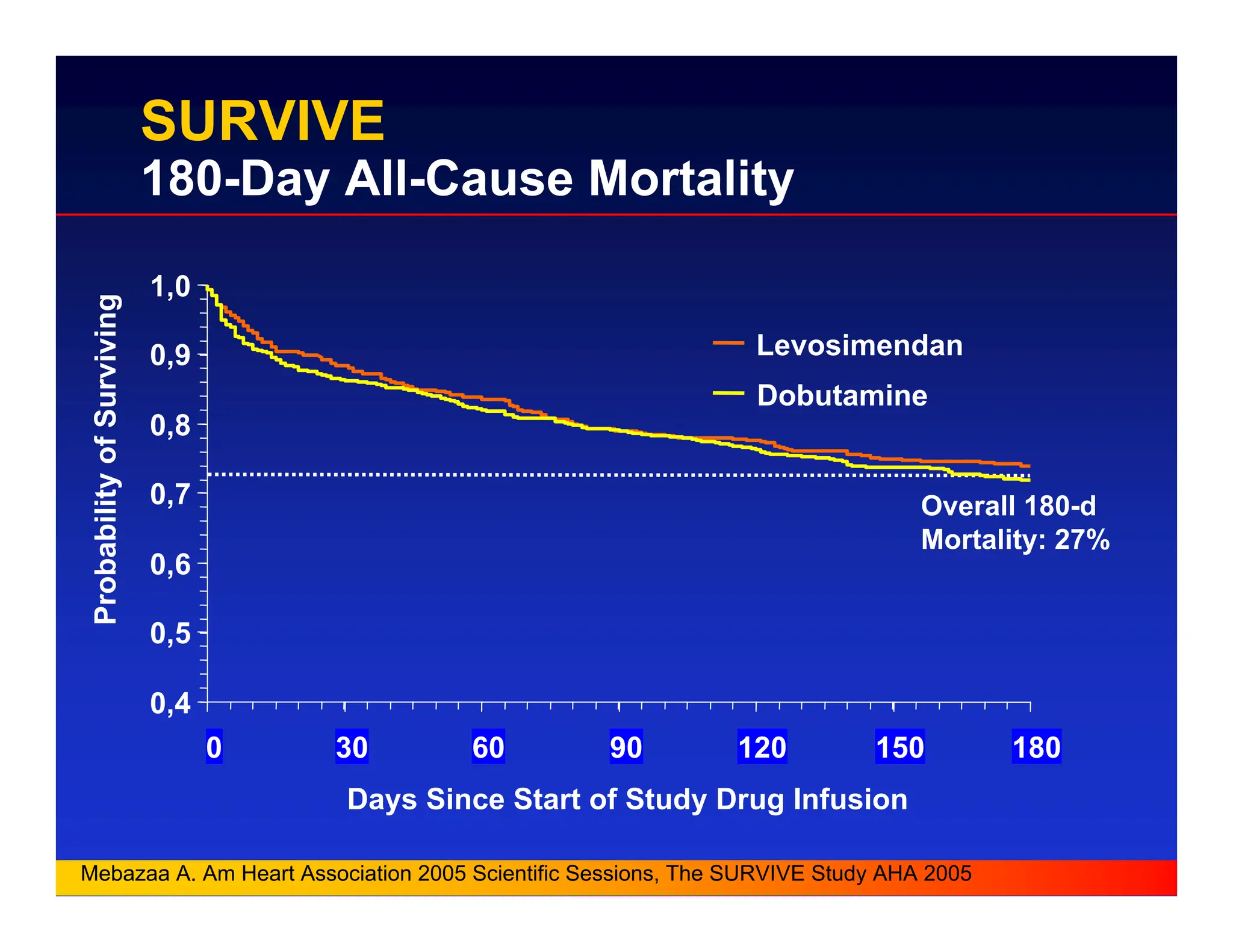
28.
Overall 180-d
Mortality: 27%
0,4
0,5
0,6
0,7
0,8
0,9
1,0
030 60 90 120 150 180
Days Since Start of Study Drug Infusion
Probability
of
Surviving
Levosimendan
Dobutamine
Mebazaa A. Am Heart Association 2005 Scientific Sessions, The SURVIVE Study AHA 2005
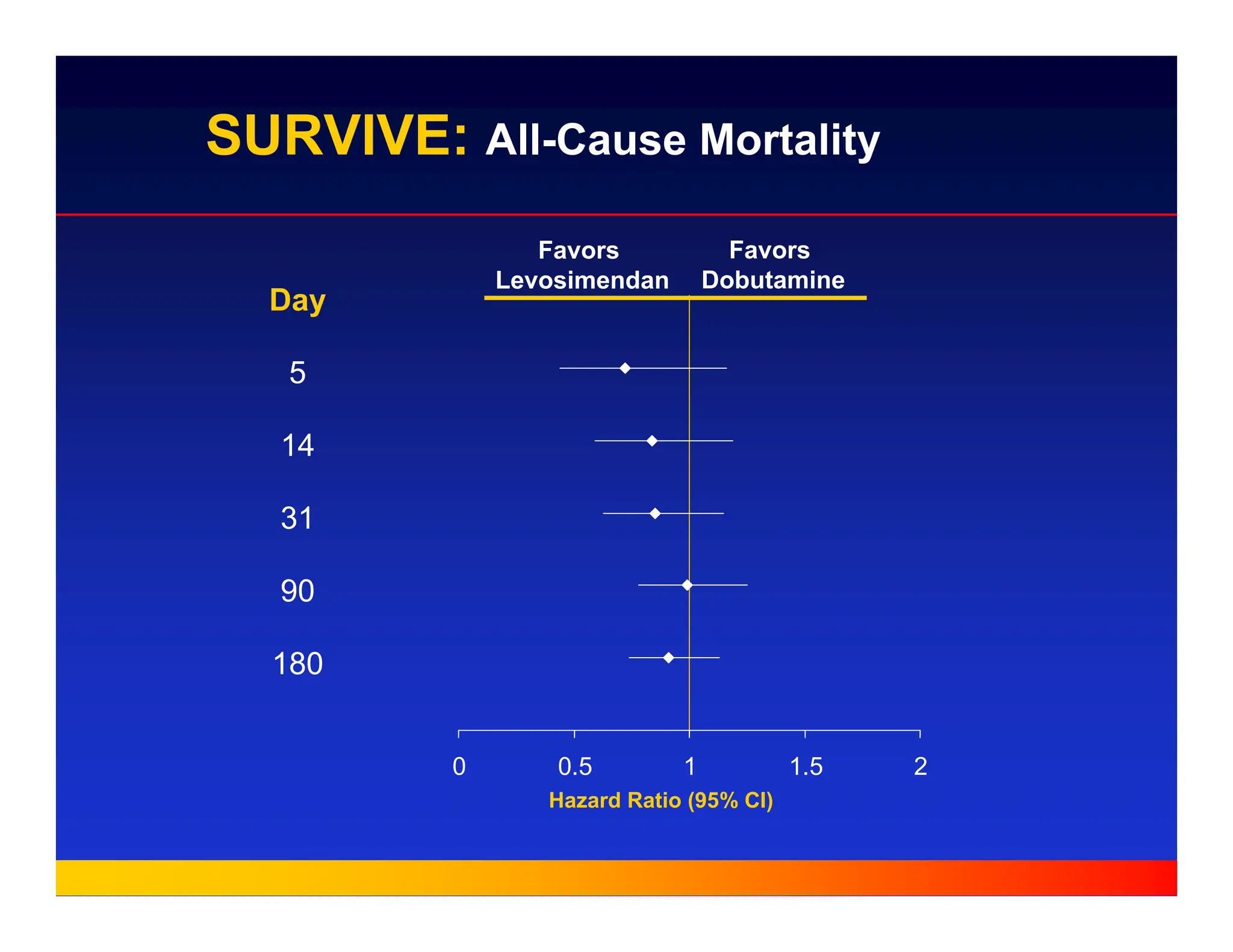
SURVIVE
180-Day All-Cause Mortality
0,1 1 10
HazardRatio (95% CI)
Favors
Levosimendan
Favors
Dobutamine
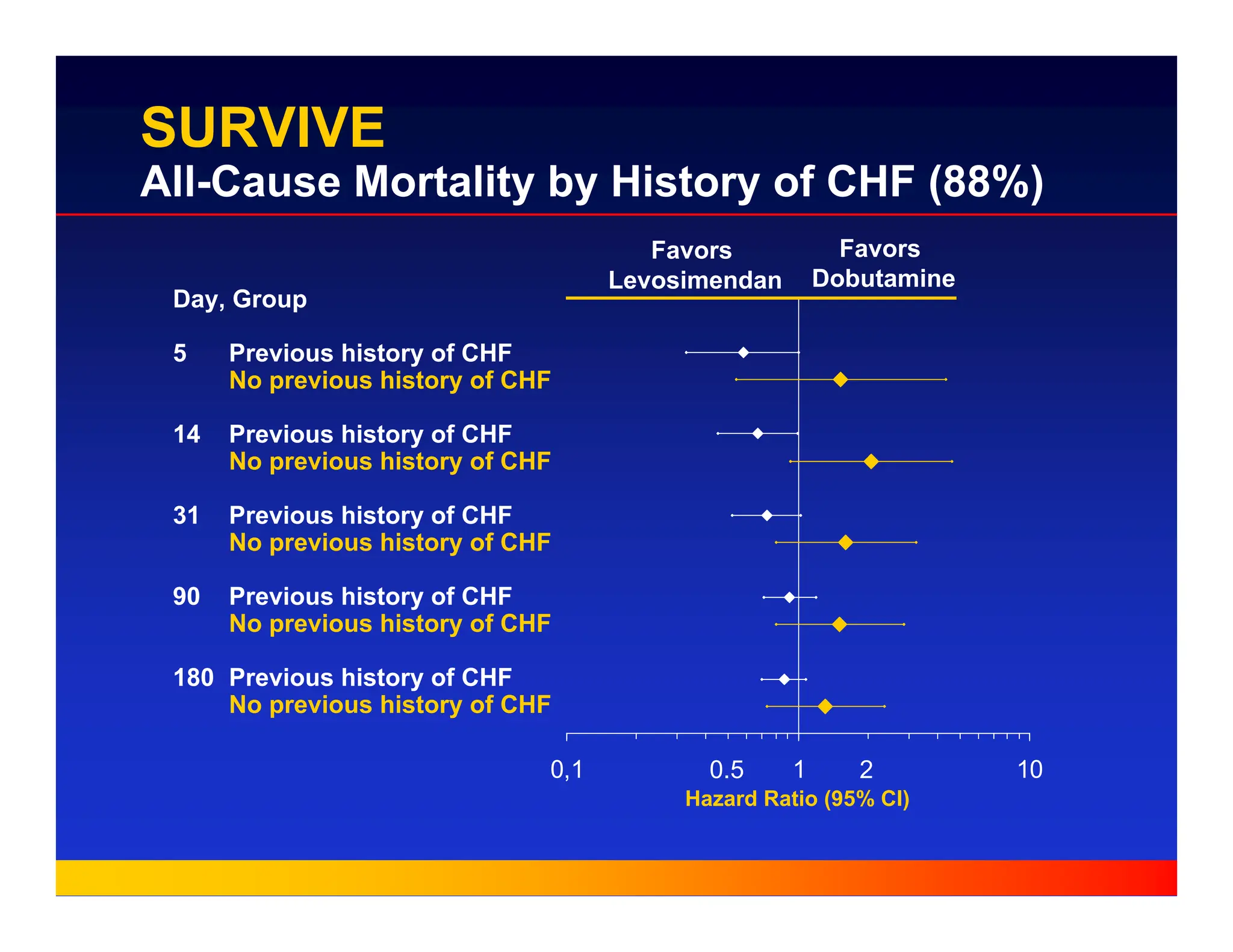
SURVIVE
All-Cause Mortality by History of CHF (88%)
Day, Group
5 Previous history of CHF
No previous history of CHF
14 Previous history of CHF
No previous history of CHF
31 Previous history of CHF
No previous history of CHF
90 Previous history of CHF
No previous history of CHF
180 Previous history of CHF
No previous history of CHF
0.5 2
Dosage of Levosimendan
(European experience)
„ Dose ranges
– Loading dose (10 min infusion)*
6 – 12 µg/kg only if SBP > 100 mmHg
– Continuous infusion (24 hours) **
0.05 – 0.2 µg/kg/min depending on BP
* Loading dose only if rapid effect (<2 hours)
required
** Prolonged infusion > 24 hours leads to
accumulation of long acting metabolites
„ Drug combinations
– Norepinephrine + levosimendan in patients with
hypotension possible
American Journal of Cardiology 2005; Follath
33.
Prerequisites for optimumefficacy and
safety of LEVOSIMENDAN
- Correction of hypovolemia after pretreatment
(vasodilators and high dose diuretics)
– Low JVP, oliguria (CVP< 12 mmHg if measured) Æ
Volume replacement before Levosimendan !
- Serum electrolytes corrected (K+, Mg2+)
– K+ ≥ 4,5 ≤ 5,5 mmol/L, Mg2+ ≥1,0 ≤ 1,3 mmol/L
- Tight BP monitoring for 4 – 6 hours
- Individualised dosage regimen
34.
Arguments pro levosimendan:
-Levosimendan is a 1st line therapeutic choice in acute/decompensated CHF
with high filling pressures, low cardiac output and oliguria,
especially under betablockers
- Symptomatic benefit in REVIVE
- Compared to dobutamine ( most frequently used inotrope ) haemodynamic
and survival advantage documented in the LIDO trial, early benefit
even in SURVIVE
- In routine clinical practice Levosimendan rapidly improves symptoms, renal function
and is well tolerated (PORTLAND)
- High loading doses, to high 24 h infusion rates and concomitant vasodilators /i.v.
diuretics are the most probable explanation for the partly disappointing results in
REVIVE and SURVIVE
There is no single drug for 1st line treatment in all types of acute HF !








































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)







