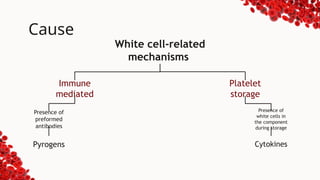
Febrile non-hemolytic transfusion reaction (FNHTR) is an acute reaction characterized by a rise in body temperature and possible accompanying symptoms like chills and tachycardia, with a prevalence of 0.5% to 5% in transfusions. The condition is often caused by immune response mechanisms related to white blood cells and preformed antibodies. Management includes stopping the transfusion, symptomatic treatment, and possibly leukoreduction in future transfusions to prevent recurrence.
















![BLOOD_TRANSFUSIOcjnsdndsN_REACTION_AND_ITS_MANAGEMENT[2].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bloodtransfusionreactionanditsmanagement2-250718043300-5d589afd-thumbnail.jpg?width=640&height=640&fit=bounds)

































