Downloaded 58 times


![3
Crest® Oral-B
®
at dentalcare.com Continuing Education Course, Revised January 9, 2012
approach to oral health care that requires the
judicious integration of systematic assessments
of clinically relevant scientific evidence, relating to
patient’s oral and medical condition and history,
with the dentists’ clinical expertise and the
patient’s treatment needs and preferences.
3
Inherent in these definitions is the recognition that
research evidence is a valued component of the
clinical decision-making process, and the intent
is that the use of current best evidence does not
replace clinical skills, judgment, or experience
but provides another dimension to the decision-
making process that also considers the patient’s
preferences.
4-6
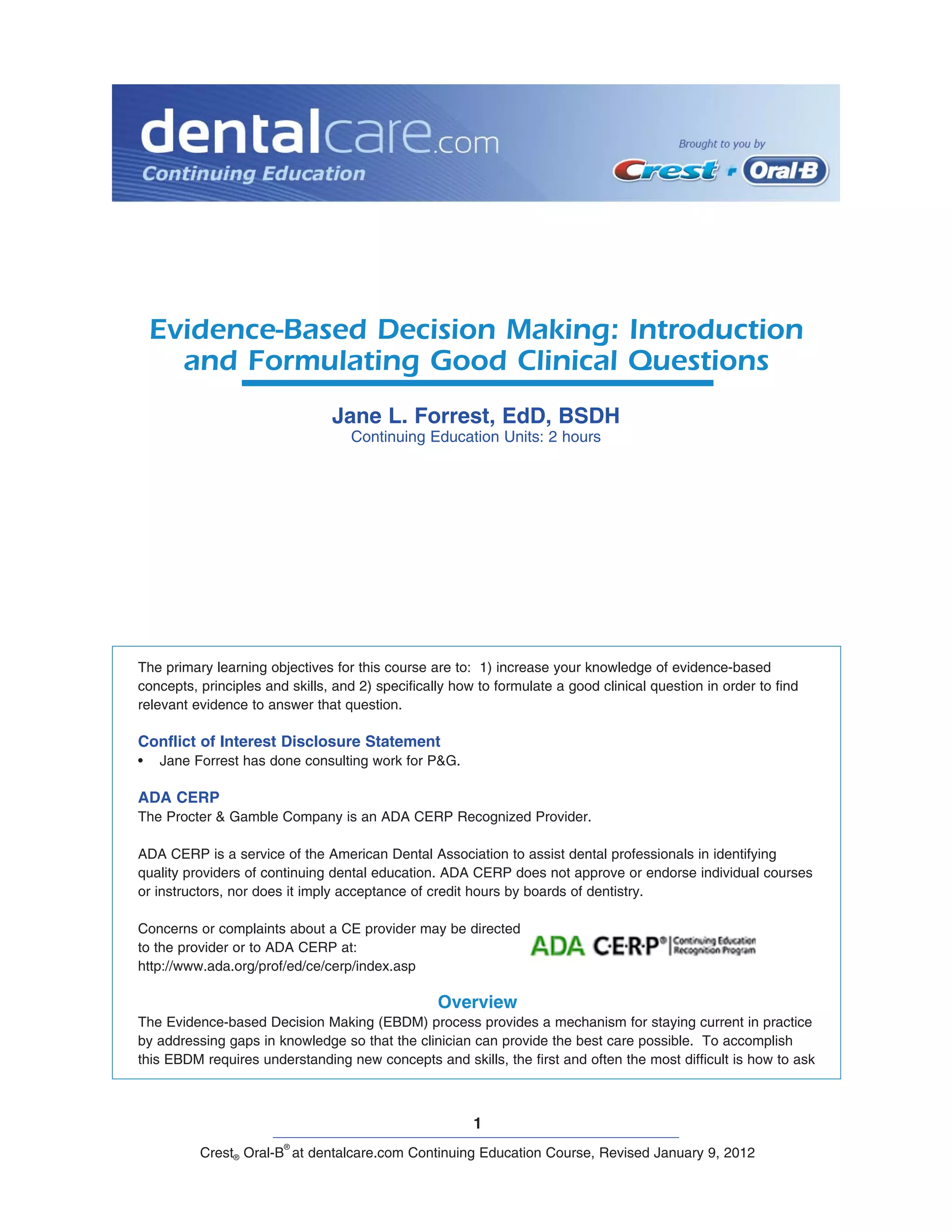
(Figure 1) It is this decision-making
process that we refer to as Evidence-Based
Decision Making (EBDM) and is defined as:
The formalized process of using the
skills for identifying, searching for
and interpreting the results of the
best scientific evidence, which is
considered in conjunction with the
clinician’s experience and judgment,
the patient’s preferences and values,
and the clinical/patient circumstances
when making patient care decisions.
Again, EBDM is not unique to medicine or any
specific health discipline, but represents a concise
way of referring to the application of evidence to
clinical decision-making.
Is Evidence-based practice a new term
for an old concept?
The use of evidence in practice is not new. What
is new is the nature of the clinical evidence
itself in terms of the methods for gathering it
[randomized controlled trials and other well-
designed methods], the statistical tools for
synthesizing and analyzing it [systematic reviews
and meta-analysis], and the ways for ways for
accessing [electronic databases] and applying it
[evidence-based decision-making and practice
guidelines].
7,8,9
In other words, evidence-based practice is not
just a new term for an old concept and as a result
of advances, practitioners need:
1. more efficient and effective online searching
skills to find relevant evidence, and
2. critical appraisal skills to rapidly evaluate and
sort out what is valid and useful, and what is
not.
10
EBDM is the formalized process and structure for
learning these skills with the purpose of closing
the gap between what is known and what is
practiced in order to improve patient care based
on informed decision-making.
Principles of EBDM
Evidence-based decision-making is about solving
clinical problems and involves two fundamental
principles:
1. Evidence alone is never sufficient to make a
clinical decision. Initially, the focus of EBM
emphasized using randomized clinical trials
and other quantifiable methods. However, as
EBM has evolved, so has the realization that
the evidence from clinical research is only one
key component of the decision making process
and does not tell a practitioner what to do.
11
2. A hierarchy of evidence exists to guide clinical
decision-making.
9
EBDM is a structured
process which incorporates a formal set of
rules for interpreting the results of clinical
research and places a lower value on
authority or custom. In contrast to EBDM,
traditional decision-making, relies more on
intuition, unsystematic clinical experience and
pathophysiologic rationale.
9,12
Figure 1. EBDM Process
©2001 Forrest, NCDHR](https://image.slidesharecdn.com/evidence-baseddentistry4-140813192026-phpapp02/85/Evidence-based-dentistry-3-320.jpg)






![10
Crest® Oral-B
®
at dentalcare.com Continuing Education Course, Revised January 9, 2012
Applying the PICO Process
The first step in developing a well-built question is
to identify the patient problem or population [P] by
describing either the patient’s chief complaint or
by generalizing the patient’s condition to a larger
population. The problem is further shaped or
refined by the most important characteristics that
might influence the results such as:
• Level of disease or health status
• Age, race, gender, previous conditions, past
and current medications
In Mr. Logan’s case, we know the chief complaint
is discoloration of his front teeth and that coffee
and tobacco are contributing factors. So, in
addition to the chief complaint, age, and current
habits, previous behaviors may influence the
decision as to which treatment might be most
appropriate.
Identifying the Intervention [I] is the second step
in the PICO process. It is important to identify
what you plan to do for that patient. This may
include the use of a specific diagnostic test,
treatment, adjunctive therapy, medication, or the
recommendation to the patient to use a product
or procedure. The intervention is the main
consideration for that patient.
4
In Mr. Logan’s
case, the intervention being considered is the
Crest Whitestrips™ since he has specifically
asked about them. This also keeps the process
patient-centered.
The third phase of the well-built question is the
Comparison [C], which is the main alternative
(intervention) you are considering.
2
It should be
specific and limited to one alternative choice,
usually the gold standard, in order to facilitate an
effective computerized search. The Comparison
is the only optional component in the PICO
question since there may not be an alternative,
however when there is one, it should be used. In
our case, we have selected the custom trays for
at-home bleaching as the main alternative.
The final aspect of the PICO question is the
outcome [O]. This specifies the result(s) of what
you plan to accomplish, improve, or affect, and it
should be measurable. Examples of outcomes
are relieving or eliminating specific symptoms,
should be stated as a concise short phrase as
illustrated in the following case example.
Case Example
Your new patient, Mr. Jim Logan, is a 48-year
old marketing executive. His chief complaint
is the/discoloration of his front teeth, which he
feels is getting worse as he gets older. He would
like them to be as white as they were when he
was 25 and even brought in a picture to show
you. He would like them whitened within one
week before he attends his 30-year high school
reunion. When reviewing his health history
and behaviors, you learn that Mr. Logan is a
coffee drinker and recently stopped smoking.
Upon examination, you determine his only
treatment needs are preventive care and suggest
you re-evaluate the discoloration after that
appointment since the stain could be removed
during his prophylaxis. If additional treatment is
needed, you can make him custom trays for use
with an at-home whitening/bleaching system.
You present the bleaching procedure options
and related fees to Jim. He questions you about
the differences between them and the Crest
Whitestrips™ that do not require a tray and can
be purchased at the local grocery store. Jim
insists the whitening strips are just as effective
and cost considerably less.
You are not familiar with the latest scientific
literature on the whitening strips to answer
Mr. Logan’s questions thoroughly. You tell
him you know the bleaching procedures you
have suggested are safe, effective, and can
produce the desired outcomes within the desired
time. However, you tell him you will be glad to
investigate the Whitestrips option so each of
you are fully informed about the pros and cons
of each method before selecting a treatment.
With the popularity of these treatment options
and new products introduced quite frequently,
this information will be a valuable addition to the
evidence-based “library” you are creating in your
office. To find the answer, you must define Jim’s
question so it facilitates an efficient search of
the literature. To guide this process, the PICO
Worksheet and Search Strategy form can assist
you. (Table 5)](https://image.slidesharecdn.com/evidence-baseddentistry4-140813192026-phpapp02/85/Evidence-based-dentistry-10-320.jpg)









This document provides an overview and introduction to evidence-based decision making (EBDM) for dental professionals. It defines key terms like evidence-based practice and discusses the need for EBDM to improve patient care and address variations in practice. The document outlines the 5 steps of EBDM and emphasizes that evidence alone is not sufficient, and a hierarchy of evidence exists. It also discusses forming answerable clinical questions as the first step using the PICO framework.












































































