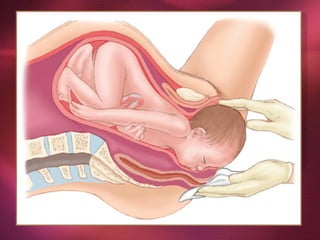
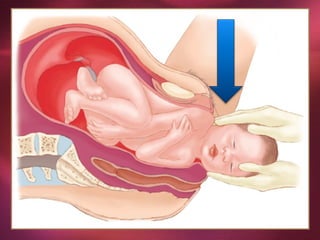
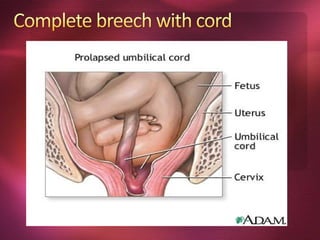
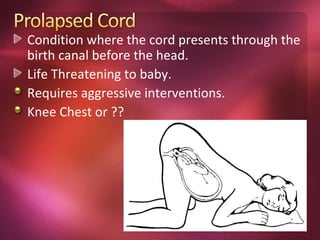
This document provides information about childbirth and caring for pregnant women and newborns during delivery. It discusses the normal process of pregnancy and birth, potential complications, steps to assist with a vaginal delivery in an emergency situation, newborn care procedures, and key questions to ask a woman in labor. The presentation aims to equip healthcare workers with knowledge to handle routine deliveries and recognize issues that may require additional assistance.