Introduction
• Children differfrom adults in their anatomy,
physiology, and emotions.
• Your approach to pediatric patients must:
− Be based on age
− Accommodate developmental and social issues
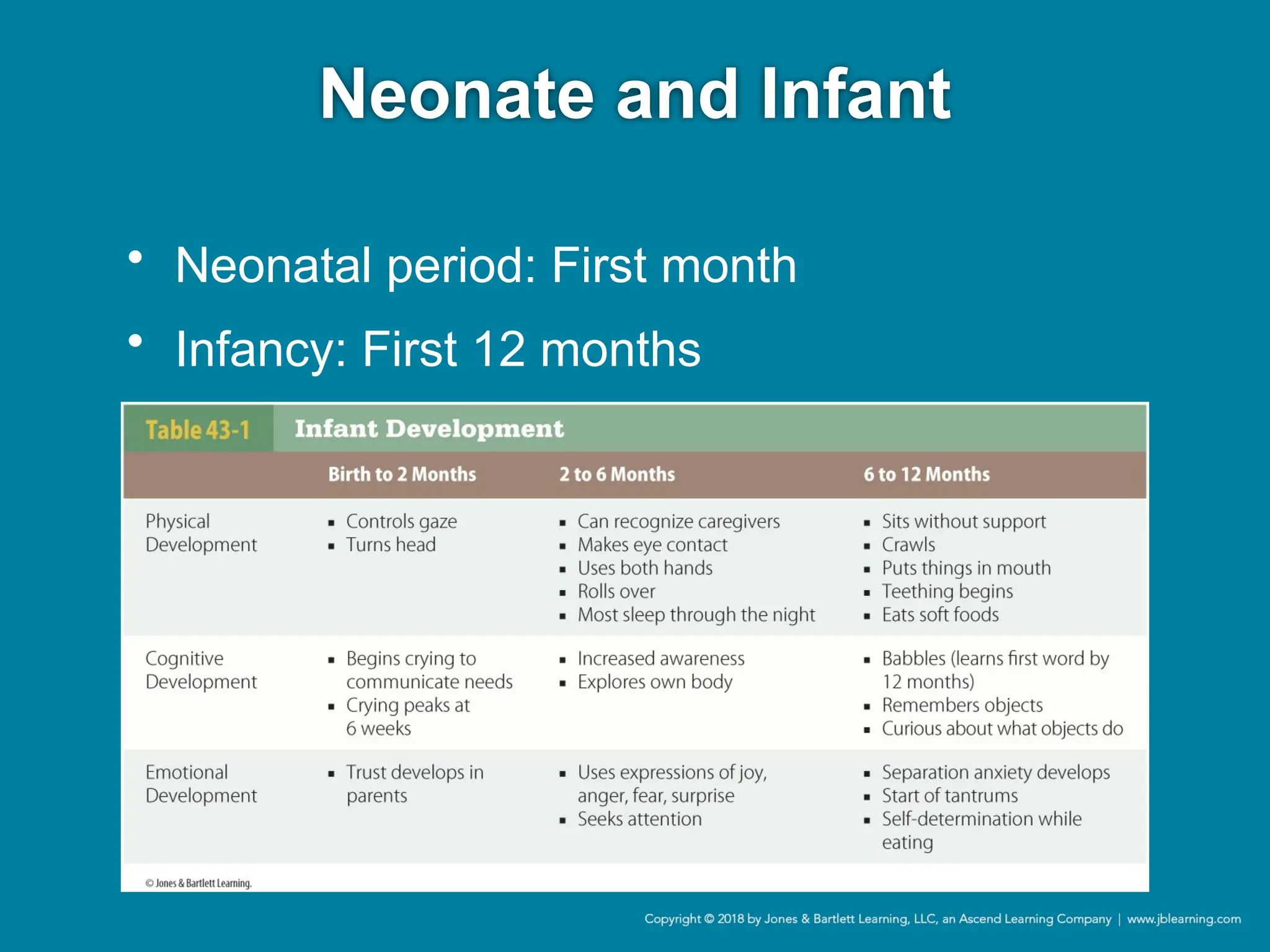
Neonate and Infant
•During assessment:
− Keep child warm.
− Support a young infant’s head and neck.
− Older infants will be calmest in a parent’s arms.
− If child is quiet, listen to heart and lungs first.
Toddler
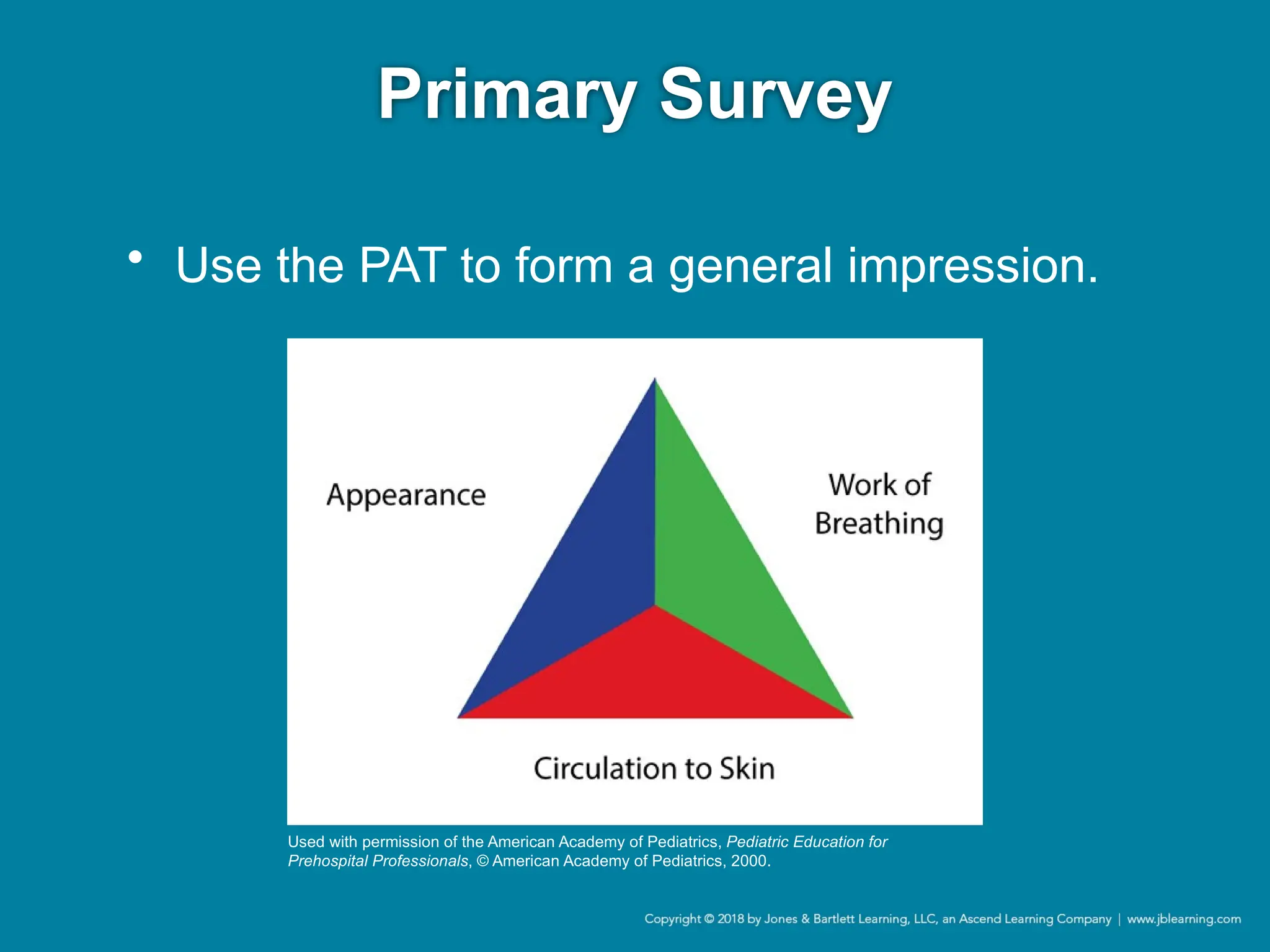
• Use thePediatric Assessment Triangle
(PAT) to assess the child.
• Strategies for examination:
− Examine on parent’s lap.
− Get down to the child’s level.
− Have a parent assist when possible.
− Be flexible.
7.
Preschool-Age Child
• Ages3 to 5
• Becoming verbal and active
• Respect modesty.
• Let child participate.
• Set limits on behavior if the child acts out.
8.
School-Age Child
• Ages6 to 12
• Capable of abstract thought, understand
cause and effect
• By age 8, anatomy and physiology is similar
to adults.
• Explain steps in simple language.
9.
Adolescence
• Ages 13to 18
• Once secondary sexual characteristics
have developed, treat as an adult.
• Address and reassure patient.
• Offer as much control as appropriate.
10.
The Head
• Infants’and young children’s heads are
large relative to the rest of their bodies.
• During infancy, the anterior and posterior
fontanelles are open.
11.
The Neck andAirway
• Short neck, smaller airway
• Epiglottis is long and floppy.
• Keep nares clear with suctioning.
• Avoid hyperextension of neck.
• Keep the airway clear of all secretions.
• Use care when managing the airway.
12.
The Respiratory System
•Smaller tidal
volume, double
metabolic oxygen
demand
• Smaller functional
residual capacity
• Faster breathing
13.
The Respiratory System
•Infants use diaphragm during inspiration.
• Experience muscle fatigue quicker
• Highly susceptible to hypoxia
− Can cause cardiovascular collapse and arrest
14.
The Cardiovascular System
•Children rely on
pulse rate to:
− Compensate for
decreased
oxygenation
− Maintain cardiac
output
15.
The Cardiovascular System
•Limited but vigorous cardiac reserves
• Injured children can be in shock and
maintain blood pressure for long periods.
• Hypotension is an ominous sign.
16.
The Heart
• ECG:Large right-sided forces are normal in
young infants.
• Cardiac output is rate dependent in infants
and young children.
• Mediastinum is more mobile.
17.
The Nervous System
•Neural tissue and vasculature are fragile.
• Brain and spinal cord are not as well
protected.
• Pediatric brain: Nearly twice the blood flow
− Makes even minor injuries significant
− Increases risk of hypoxia
18.
The Spinal Column
•Fulcrum is higher (descends with age).
• Vertebral fractures and spinal cord injuries
in young children are uncommon.
• With a significant MOI:
− Assume cervical spine injury.
− Transport with spinal immobilization.
19.
The Abdomen andPelvis
• Organs are susceptible to injury:
− Proportionally larger solid organs
− Less subcutaneous fat
− Less protective abdominal musculature
20.
The Musculoskeletal System
•Adult height requires bone growth.
• Most growth plates will be closed by late
adolescence.
• Immobilize all sprains or strains.
21.
The Musculoskeletal System
•Slipped capital femoral epiphysis (SCFE)
− Occurs in children and adolescents
− Prominently found in overweight children
− Symptoms include:
• Difficulty walking and noticeable limp
• Inability to bear weight on a limb
• Painful/limited normal flexion and rotation
22.
The Chest andLungs
• Chest wall is quite thin.
• Ribs are more pliable.
• Risk of pneumothorax during bag-mask
ventilation
− Signs are often subtle.
23.
The Integumentary System
•Infants and children have:
− Thinner and more elastic skin
− Higher body surface area (BSA)–weight ratio
− Less subcutaneous tissue
• Contribute to:
− Increased risk of injury and hypothermia
− Increased severity of burns
24.
Metabolic Differences
• Limitedstores of glycogen and glucose
• Hypovolemia and electrolyte derangements
are common.
• Keep warm during transport.
25.
Parents of Illor Injured
Children
• Rapport with caregivers is critical.
• Approach in a calm, professional manner.
• Transport with the child.
• Remember that your first priority is the child.
26.
Pediatric Patient Assessment
•Differs from adult assessment
• Adapt your assessment skills.
• Have age-appropriate equipment.
• Review age-appropriate vital signs.
27.
Scene Size-up
• Onthe way to the scene, prepare for
pediatric:
− Size-up
− Equipment use
− Assessment
• Collect information from dispatch.
28.
Scene Size-up
• Takeappropriate standard precautions.
• Note child’s position.
• Look for clues to MOI or NOI.
• Note pills, medicine bottles, alcohol, drug
paraphernalia, or household chemicals.
• Observe the scene or vehicle for clues.
29.
Scene Size-up
• Otherimportant assessments:
− Cleanliness of home
− Appearance of other children in family
− Presence of medical devices
− Indications of substance abuse
Primary Survey
• Circulationto skin
− Determines adequacy of cardiac output and
core perfusion.
− Pallor, mottling, cyanosis
36.
Primary Survey
• Stayor go
− Use findings from PAT to determine whether the
patient requires urgent care.
• Assess ABCDEs.
• Treat life threats.
• Transport.
− If condition is stable, finish assessment.
Hands-on Primary Survey
•Airway
− Determine whether airway is open and patient
has adequate chest rise with breathing.
− If there is potential obstruction, position airway
and suction as necessary.
Hands-on Primary Survey
•Circulation
− Integrate information from PAT.
− Listen to the heart or feel pulse for 30 seconds.
• Double the number to get pulse rate.
− After checking the pulse rate, do a hands-on
evaluation of skin CTC.
41.
Hands-on Primary Survey
•Disability
− Use the AVPU scale or Pediatric Glasgow Coma
Scale to assess level of consciousness.
• Assess pupillary response.
• Evaluate motor activity.
− Combine this information with PAT to determine
neurologic status.
Hands-on Primary Survey
•Exposure
− Perform a rapid exam of the entire body.
− Avoid heat loss, especially in infants.
− Cover child as soon as possible.
45.
Transport Decision
• Transportimmediately for trauma with:
− Serious MOI
− Physiologic abnormality
− Significant anatomic abnormality
− Unsafe scene
• Attempt vascular access en route.
46.
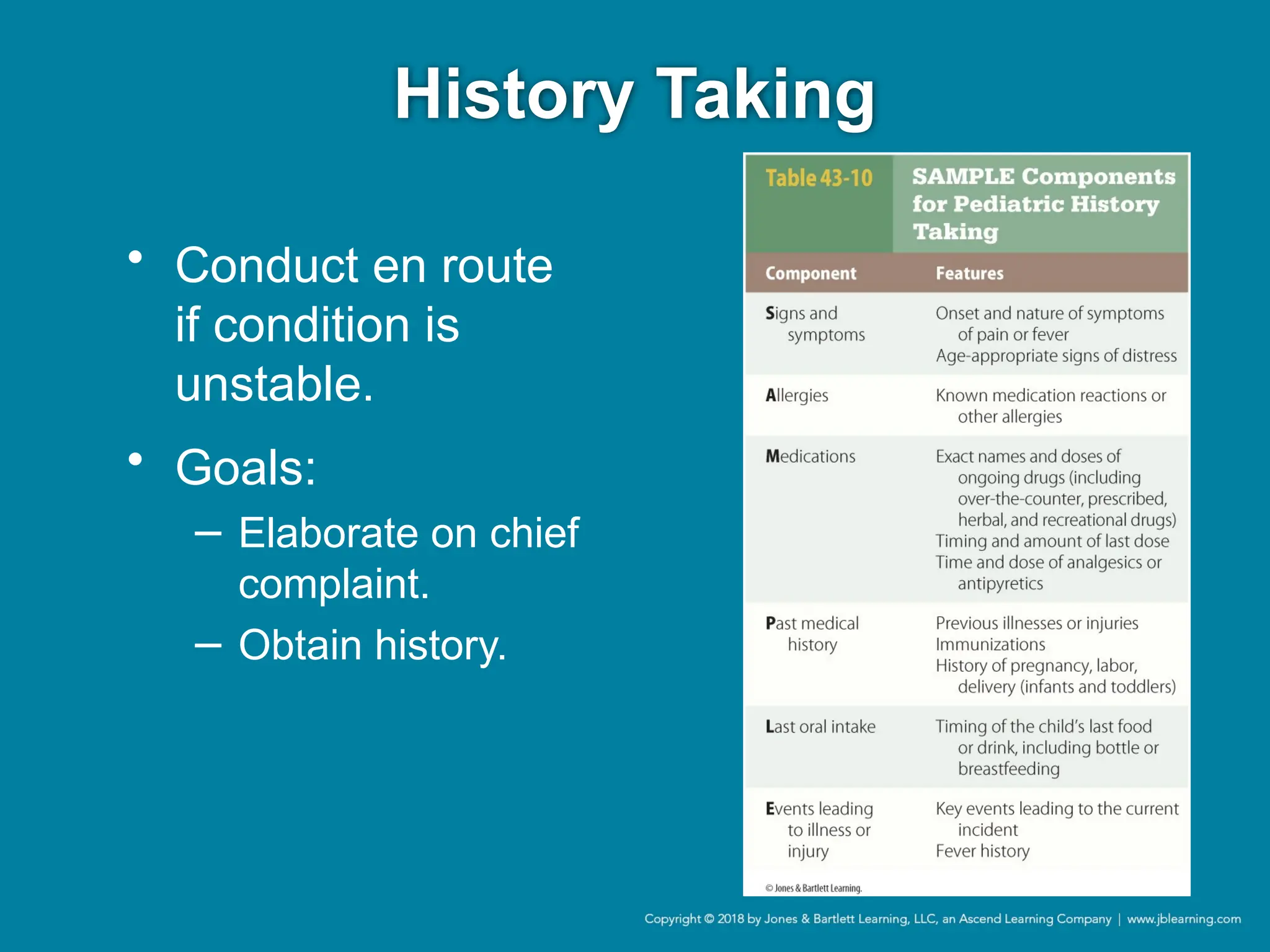
History Taking
• Conducten route
if condition is
unstable.
• Goals:
− Elaborate on chief
complaint.
− Obtain history.
47.
Secondary Assessment
− Head
−Pupils
− Nose
− Ears
− Mouth
− Neck
− Chest
− Back
− Abdomen
− Extremities
− Capillary refill
− Level of hydration
• May include a full-body examination or a
focused assessment
48.
Secondary Assessment
• Attemptto take the
child’s blood
pressure on the
upper arm or thigh.
− Minimal systolic
blood pressure =
70 + (2 × Age in
years)
49.
Secondary Assessment
• Pediatricpain
− When assessing pain:
• Consider developmental age.
• Discuss child’s pain with caregivers.
• Use pain scales with pictures.
Reassessment
• Includes thefollowing:
− PAT
− Patient priority
− Vital signs
− Assessment of interventions
− Reassessment of focused exam areas
52.
Respiratory Emergencies
• Frequentlyencountered
• Respiratory failure and arrest precede
majority of cardiopulmonary arrests.
• Early identification and intervention are
critical.
53.
Respiratory Arrest, Distress,
andFailure
• First determine severity.
− Distress, failure, or arrest
• Keep anatomic and physiologic respiratory
differences in mind.
54.
Respiratory Arrest, Distress,
andFailure
• Respiratory distress
− Increased work of breathing results in adequate
gas exchange.
• Respiratory failure
− Patient can no longer compensate; hypoxia
and/or carbon dioxide retention occur.
• Respiratory arrest
− Patient is not breathing spontaneously.
55.
Respiratory Arrest, Distress,
andFailure
• Determining
severity of illness
will indicate
urgency of
treatment and
transport.
− Obtain SAMPLE
history on scene
or during
transport.
56.
Respiratory Arrest, Distress,
andFailure
• Respiratory distress is most common.
− Requires only supportive care
• With fatigue, distress may progress to
failure.
• Reassess frequently.
57.
Respiratory Arrest, Distress,
andFailure
• Respiratory emergency treatment
− Give supplemental oxygen.
− Perform ECG monitoring.
− Establish IV access.
− Manage the airway.
− Use supraglottic airway devices and intubation
only if bag-mask ventilation fails.
58.
Foreign Body Aspirationor
Obstruction
• Infants and toddlers have a high risk of
foreign body aspiration.
− Mild obstruction:
• Awake
• Stridor
• Increased work of breathing
• Good color
− Severe obstruction
• Cyanotic
• Unconscious
Foreign Body Aspirationor
Obstruction
• Removing a foreign body in unresponsive
infants
− If infant loses consciousness, start CPR.
• Perform 30 chest compressions.
• Look inside mouth; remove object if seen.
• Continue compressions and ventilation.
• Assess for a pulse.
61.
Foreign Body Aspirationor
Obstruction
• Removing a foreign body in children
− Use the Heimlich maneuver.
− If the child becomes unresponsive:
• Position supine; perform 30 chest compressions.
• Look inside mouth; remove object if seen.
• Proceed with laryngoscopy and removal with
Magill forceps.
Anaphylaxis
• Severe anaphylaxis
−Child may be unresponsive due to respiratory
failure and shock.
− Primary survey may reveal:
• Hives
• Swelling of the lips and oral mucosa
• Stridor and/or wheezing
Croup
• Viral infectionof the upper airway
• SAMPLE history usually reveals several days
of cold symptoms and low-grade fever
followed by:
− Barky cough
− Stridor
− Trouble breathing
66.
Croup
• Initial management:
−Position of comfort
− Avoid agitating the child.
− Administer dexamethasone IV or IM.
− Nebulized epinephrine
− Assisted ventilation with bag-mask ventilation
may be necessary.
67.
Epiglottitis
• Inflammation ofthe epiglottis and
supraglottic tissues
• Classic presentation:
− Sick, anxious; sitting in sniffing position
− Drooling
− Increased work of breathing
− Pallor or cyanosis
68.
Epiglottitis
• Symptoms progressrapidly.
• Ask about immunizations, and get the child
to an appropriate hospital.
− Be prepared with a bag-mask device and an ET
tube.
69.
Bacterial Tracheitis
• Bacterialinfection of subglottic area of the
upper airway
• Children typically present with:
− Cough, stridor, respiratory distress
− History of preceding viral infection
• Keep patient as calm and comfortable as
possible.
70.
Asthma
• Most commonchronic childhood illness
• Main components:
− Bronchospasm
− Mucus production
− Airway inflammation
71.
Asthma
• Triggers
− Upperrespiratory
infections
− Allergies
− Exposure to cold
− Changes in the
weather
− Secondhand
smoke
• Clinical signs
− Frequent cough
− Wheezing
− General signs of
respiratory
distress
72.
Asthma
• Initial management:
−Position of comfort
− Supplemental oxygen
− Bronchodilators
− IM dexamethasone
− Epinephrine for severe respiratory distress
73.
Respiratory Syncytial Virus
(RSV)Infection
• Common and contagious virus that causes
bronchiolitis and pneumonia in children
• Transmitted via:
− Direct contact with large droplets
− Indirect contact with contaminated hands or
items
74.
Respiratory Syncytial Virus
(RSV)Infection
• Early signs and symptoms include:
− Sneezing
− Runny nose
− Nasal congestion
− Cough
− Fever
75.
Respiratory Syncytial Virus
(RSV)Infection
• Prevention requires use of personal
protective equipment:
− Gloves
− Alcohol-based foams and gels
• Post-transport vehicle cleaning
• Postexposure treatment is supportive.
76.
Bronchiolitis
• Inflammation orswelling of small airways in
lower respiratory tract due to viral infection
− Highly contagious
− Characteristic findings include:
• Mild to moderate retractions
• Tachypnea
• Diffuse wheezing and crackles
• Mild hypoxia
77.
Bronchiolitis
• Danger of
respiratoryfailure:
− Sleepy
− Severe retractions
− Diminished breath
sounds
− Moderate to
severe hypoxia
• Greatest risk for
respiratory failure:
− First months of life
− Prematurity
− Lung disease
− Congenital heart
disease
− Immunodeficiency
78.
Bronchiolitis
• Management issupportive.
− Position of comfort
− Supplemental oxygen
− Suction thick secretions.
• If suctioning and oxygen administration fail,
nebulized racemic epinephrine should be
given for severe respiratory distress.
79.
Pneumonia
• Disease infectinglower airway and lung
• Signs include:
− Unusually rapid breathing
− Grunting or wheezing
− Hypothermia or fever
• Primary treatment is supportive.
80.
Pertussis
• Also knownas whooping cough
• Highly contagious
• Symptoms similar to common cold
• Keep airway patent, and transport to ED.
81.
Cystic Fibrosis (CF)
•Genetic disease that affects respiratory and
digestive systems
• Chronic mucus production
− Tachypnea, chest pain, crackles
• Assess breathing, and administer
supplemental oxygen as needed.
82.
Bronchopulmonary Dysplasia
• Spectrumof lung conditions found in full-
term and preterm neonates who required:
− Long periods of high-concentration oxygen
− Ventilator support
• Many patients will be on home oxygen.
Oropharyngeal (Oral) Airway
•Keeps the tongue from blocking the airway
− Makes suctioning easier
− Use with patients who are unresponsive.
• Avoid injuring the hard palate as you insert.
86.
Nasopharyngeal (Nasal) Airway
•Usually well tolerated
• Used for conscious patients and patients
with altered levels of consciousness
• Rarely used for children younger than
1 year
87.
Nasopharyngeal (Nasal) Airway
•Several problems are possible:
− Diameter that is too small
− Airway that is too long
− Inserting the airway in responsive patients
• Do not use with facial trauma or moderate
to severe head trauma.
88.
Oxygenation
• All patientswith respiratory emergencies
should receive supplemental oxygen.
• Common methods for pediatric patients
− Blow-by technique
− Nonrebreathing mask
Bag-Mask Ventilation
• Useif airway positioning or adjunct does not
improve respiratory effort.
• May need to try a variety of mask sizes
• Deliver breaths at a rate of 12 to 20
breaths/min for infants and children.
Bag-Mask Ventilation
• Errorsin technique can result in gastric
distention or decreased venous return to
the heart (preload).
• Two-person bag-mask ventilation is usually
more effective.
94.
Supraglottic Airways
• Devicesused to provide:
− Positive pressure ventilation to apneic patients
− Maintain a patent airway in unresponsive
patients who are breathing but need advanced
airway management
Endotracheal Intubation
• Advantages
−Definitive airway
− Decreased risk of aspiration
• High complication rate, which includes:
− Bradycardia
− Increased ICP
− Incorrect placement
97.
Endotracheal Intubation
• Indicationsinclude:
− Cardiopulmonary arrest
− Traumatic brain injury
− Inability to maintain a patent airway
− Need for prolonged ventilation
• Remember the differences between the
adult and pediatric airways.
98.
Endotracheal Intubation
• Pediatricequipment is mandatory.
− Laryngoscope blades sizes 0 to 3
− ET tubes sizes 2.5 to 6.0
• Any size laryngoscope handle can be used.
99.
Endotracheal Intubation
• Appropriatelysized blade extends from the
patient’s mouth to the tragus of the ear.
− Length-based resuscitation tape measure
− General guidelines:
• Premature newborn: Size 0 straight blade
• Full-term newborn to 1 year: Size 1 straight
blade
• 2 years to adolescent: Size 2 straight blade
• Adolescent +: Size 3 straight or curved blade
100.
Endotracheal Intubation
• UncuffedET tube
− Use a 3.5-mm tube for infants up to 1 year.
− Use a 4-mm tube for children between 1 and 2
years.
− Use formula for children older than 2 years:
• 4 + (Age in years ÷ 4) = Uncuffed tube size (in mm)
101.
Endotracheal Intubation
• CuffedET tube
− Use a 3-mm tube for infants and a 3.5-mm tube for
children between 1 and 2 years.
− Use formula for children older than 2 years:
• 3.5 + (Age in years ÷ 4) = Cuffed tube size (in mm)
102.
Endotracheal Intubation
• Appropriatedepth for insertion is 2 to 3 cm
beyond vocal cords.
− Record as the mark at the corner of the child’s
mouth.
• With stylet in place, bend ET tube into a
gentle upward curve.
103.
Endotracheal Intubation
• Preoxygenatebefore intubation.
• Ensure head is in the proper position.
• Insert an airway adjunct if needed.
• Apply a cardiac monitor if one is available.
• Use a pulse oximeter before, during, and
after the intubation.
104.
Endotracheal Intubation
• Havesuction handy.
• If an intubated child deteriorates, use the
DOPE mnemonic to identify the problem.
− Displacement
− Obstruction
− Pneumothorax
− Equipment failure
105.
Endotracheal Intubation
• Complications:
−Unrecognized esophageal intubation
− Induction of emesis, possible aspiration
− Hypoxia from prolonged intubation attempts
− Damage to teeth, soft tissues, and intraoral
structures
106.
Orogastric and Nasogastric
TubeInsertion
• Invasive gastric decompression
− Placement of a nasogastric (NG) tube or
orogastric (OG) tube to decompress the
stomach
− Removes the contents with suction
− Makes assisting ventilation easier
− Contraindicated in unresponsive children
107.
Orogastric and Nasogastric
TubeInsertion
• Needed equipment
− Appropriately sized NG or OG tube
− 30- to 60-mL syringe with funnel-tipped adapter
− Mechanical suction
− Adhesive tape
− Water-soluble lubricant
Orogastric and Nasogastric
TubeInsertion
• Place patient in a supine position.
• If patient is unresponsive, perform ET
intubation before gastric tube placement.
• In a trauma patient, maintain in-line
stabilization of the cervical spine.
• Lubricate the end of the tube.
110.
Orogastric and Nasogastric
TubeInsertion
• OG tube insertion
− Insert tube over tongue.
− Advance tube into hypopharynx, then rapidly
into the stomach.
− Immediately remove tube with coughing,
choking, or change in voice.
111.
Orogastric and Nasogastric
TubeInsertion
• NG tube insertion
− Insert tube gently through the naris.
− Advance the tube into the stomach.
− If unsuccessful, use the OG approach.
112.
Orogastric and Nasogastric
TubeInsertion
• Assessing tube placement
− Aspirate stomach contents.
• If you hear a rush of air over the stomach, the
placement is correct.
− If correct placement cannot be confirmed,
remove the tube.
113.
Orogastric and Nasogastric
TubeInsertion
• Complications
− Placement of tube into the trachea, resulting in
hypoxia
− Vomiting, aspiration of stomach contents
− Airway bleeding or obstruction
− Passage of tube into the cranium
114.
Cardiopulmonary Arrest
• Mostoften associated with respiratory
failure and shock
• About 25% result from sudden
dysrhythmias that require:
− Delivery of high-quality CPR
− Recognition of shockable rhythm
− Prompt defibrillation
115.
Shock
• Inadequate deliveryof oxygen and nutrients
to tissues to meet metabolic demand
• Three types:
− Hypovolemic
− Distributive
− Cardiogenic
116.
Shock
• Compensated shock
−Critical abnormalities of perfusion
− Body is able to maintain adequate perfusion to
vital organs.
− Intervention is needed to prevent child from
decompensating.
117.
Shock
• Decompensated shock
−State of inadequate perfusion
• Child will be profoundly tachycardic and
show signs of poor peripheral perfusion.
− Hypotension is a late and ominous sign.
• Start resuscitation on scene.
118.
Hypovolemic Shock
• Mostcommon cause of shock in infants and
young children
− Loss of volume due to illness or trauma
− Early signs may include:
• Tachycardia
• Pale or mottled skin
• Cool extremities
119.
Hypovolemic Shock
• Management
−Position of comfort
− Supplemental oxygen
− Keep the child warm.
− Direct pressure to stop external bleeding
− Volume replacement
Hypovolemic Shock
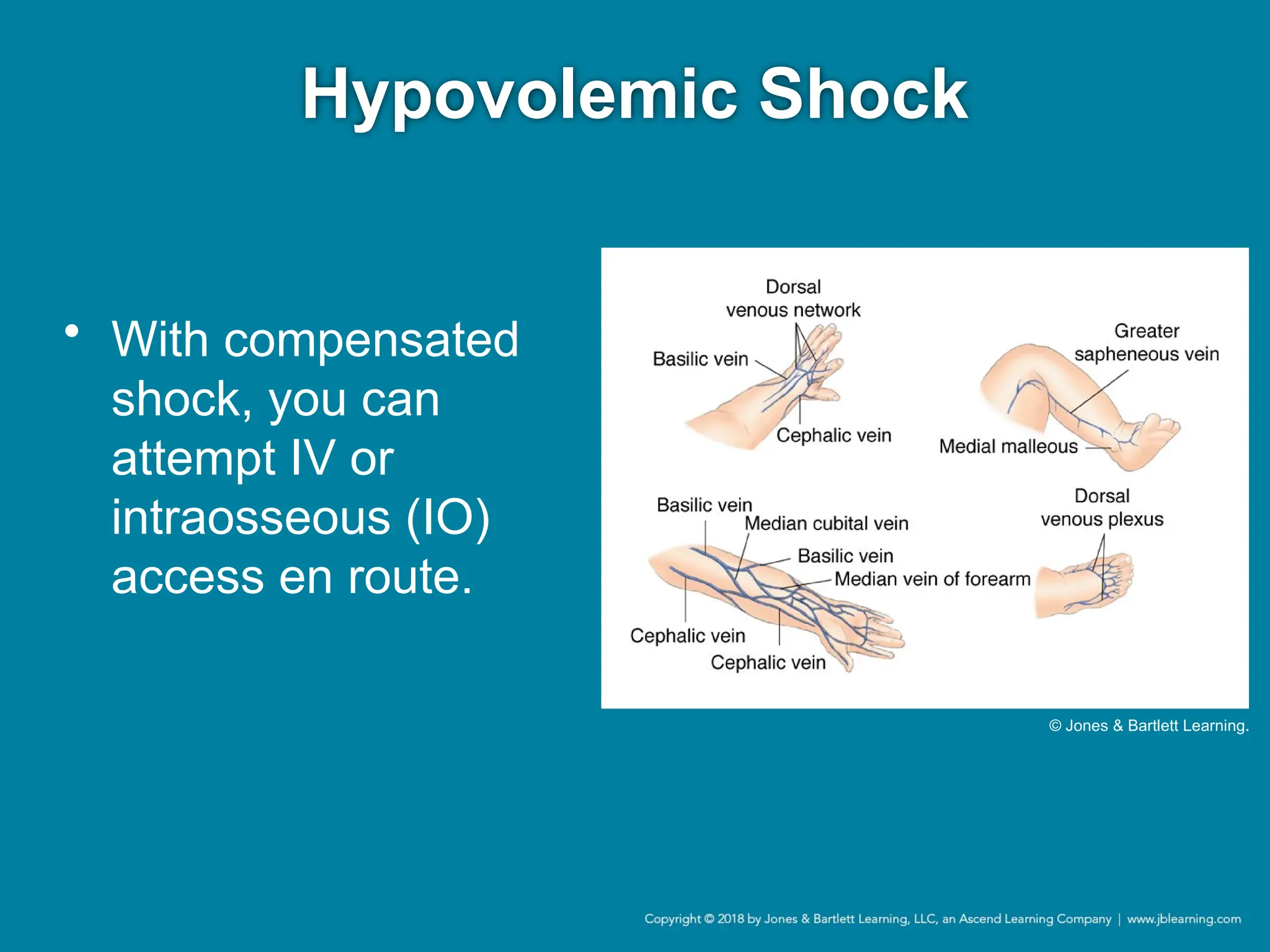
• EstablishIV access.
• Begin fluid resuscitation with isotonic fluids
only.
• In decompensated shock with hypotension,
begin initial fluid resuscitation on scene.
− Evaluate sites for IV access.
• If this is unsuccessful, begin IO infusion.
122.
Hypovolemic Shock
• IOneedles usually
consist of a solid-
bore needle inside
a sharpened
hollow needle.
Courtesy of VidaCare Corporation (www.vidacare.com).
123.
Distributive Shock
• Decreasedvascular tone develops.
− Vasodilation and third spacing of fluids occurs.
− Caused by sepsis in most pediatric cases
• Treatment is volume resuscitation.
− With apparent sepsis and persistent
hypotension, consider vasopressor support.
− Treat anaphylactic shock with IM epinephrine.
124.
Cardiogenic Shock
• Resultof pump failure
• May be present in children with:
− Underlying congenital heart disease
− Myocarditis
− Cardiomyopathy
− Rhythm disturbances
125.
Cardiogenic Shock
• Signsand symptoms may include:
− Listless or lethargic
− Increased work of breathing
− Impaired circulation
− Skin pale, mottled, or cyanotic
− Enlarged liver
− Sweating with feeding
− History of congenital heart disease
126.
Cardiogenic Shock
• Initialmanagement includes:
− Position of comfort
− Supplemental oxygen
− Transport
• Facility must offer pediatric critical care.
− Supplemental oxygen
127.
Cardiogenic Shock
• Erron the side of fluid resuscitation unless
you are sure of diagnosis.
• The following confirms cardiogenic shock:
− Increased work of breathing
− Drop in oxygen saturation
− Worsening perfusion after a fluid bolus
128.
Cardiovascular Emergencies
• Relativelyrare in children
• Often related to respiratory insufficiency,
arrest, or infection
• Identify through primary survey.
129.
Dysrhythmias
• Classified basedon pulse rate
− Too slow (bradydysrhythmias)
− Too fast (tachydysrhythmias)
− Absent (pulseless)
• Signs and symptoms are often nonspecific.
130.
Bradydysrhythmias
• Often secondaryto hypoxia in children
• Initial treatment:
− Airway management
− Supplemental oxygen
− Assisted ventilation as needed.
131.
Bradydysrhythmias
• Try toidentify and treat the underlying cause
of the bradycardia.
• Initiate electronic cardiac monitoring.
− With a sinus bradycardia, the heart rate is
slower than the lower range of normal for the
patient’s age.
− Incidental finding in adolescents
132.
Bradydysrhythmias
• Atrioventricular (AV)block
− First-degree block
• Asymptomatic, often incidental finding
• No intervention is needed.
• Treatment only with signs of cardiovascular
compromise
− Second-degree block
• Progressive prolongation of the PR interval; drop
of the QRS complex
• May progress to third-degree block
Tachydysrhythmias
• Pulse rateis higher than normal for age.
• Subdivided into two types:
− Narrow complex tachycardia: QRS complex is
0.09 second or less
− Wide complex tachycardia: QRS complex is
greater than 0.09 second
135.
Tachydysrhythmias
• Treatment isdirected at underlying cause.
− Treat with antipyretics if child appears well, has
a fever, and monitor shows sinus tachycardia.
− Use fluid resuscitation for a child with sinus
tachycardia and a history of vomiting or
diarrhea.
136.
Tachydysrhythmias
• Narrow complextachycardia
− SVT: The most frequent tachydysrhythmia
requiring treatment
− Identified by:
• Narrow QRS complex
• Absence of P waves
• Unvarying heart rate of more than 220 beats/min
(infant) or more than 180 beats/min (child)
137.
Tachydysrhythmias
• Narrow complextachycardia (cont’d)
− Treatment depends on perfusion and stability.
• If stable, consider vagal maneuvers while
obtaining IV access.
• If poor perfusion, synchronized cardioversion is
recommended.
138.
Tachydysrhythmias
• Wide complextachycardia
− Wide QRS complex tachycardia and palpable
pulse is likely ventricular tachycardia (VT).
− If stable, consider antidysrhythmic medication.
− If unstable, use synchronized cardioversion.
− If pulseless, begin CPR.
Heart Failure
• Heartcannot meet metabolic demands at
normal physiologic venous pressures.
• Signs and symptoms
− Infants: Tachypnea, retractions, grunting
− Children: Profuse sweating, increased work of
breathing during feedings
− Older children: Tachycardia, crackles
144.
Heart Failure
• Treatmentmay include:
− Oxygen
− Diuretics
− Inotropic medications (may be ordered by
medical direction)
− IV fluids (use judiciously)
145.
Myocarditis
• Inflammation ofthe heart
− Results in myocardial dysfunction
− Can lead to heart failure
• Viral infections are common cause.
146.
Myocarditis
• Transport withcardiac monitors.
• Obtain vascular access but use judiciously.
• Patients will often need inotropic support.
• Apply oxygen during transport.
147.
Cardiomyopathy
• Dilated cardiomyopathy
−Progressive dilation of the ventricles and poor
contraction of myocardial muscle fibers
− Typically due to viral infection or toxicity
− Patients can present with fatigue, weakness,
and signs of heart failure
148.
Cardiomyopathy
• Hypertrophic cardiomyopathy
−Heart muscle is unusually thick.
− Heart has to pump harder to get blood to leave.
− Patients can present with chest pain,
dysrhythmias, dyspnea, syncope, and sudden
death.
Assessment and Managementof
Cardiovascular Emergencies
• Begin with PAT, primary survey, and
secondary assessment.
− An abnormal appearance may indicate the need
for rapid intervention.
• Tachypnea is common with a primary cardiac
problem.
• Increased work of breathing and a fast respiratory
rate are common with heart failure.
151.
Assessment and Managementof
Cardiovascular Emergencies
• Determine:
− Likely underlying cause
− Patient’s priority
− Need for treatment or transport
• Repeat PAT and ABCs after intervention.
152.
Neurologic Emergencies
• Canbe benign or life threatening
• Medical history is important, including:
− Previous seizures
− Shunts
− Cerebral palsy
− Recent trauma or ingestions
153.
Altered Mental Status
•Conditions that can interfere with mental
status include:
− Metabolic problems
− Infectious diseases
− Intracranial structural abnormalities
− Trauma
− Hypoxia
− Poisonings
154.
Altered Mental Status
•Use mnemonic AEIOUTIPS to remember
common causes.
• Run through PAT and ABCDEs quickly.
− Pay attention to disability and dextrose issues.
− Check glucose.
155.
Altered Mental Status
•Assess and support airway and breathing.
• If hypoglycemic, give glucose.
• If signs or symptoms suggest an opiate
toxidrome, consider naloxone.
156.
Altered Mental Status
•Transport all patients expeditiously.
• Assess for increased ICP.
− Adding lidocaine prior to intubation may blunt
the increase in ICP associated with intubation.
− Signs include Cushing triad.
157.
Seizures
• Result fromabnormal electrical discharges
in the brain
− May be predisposed, or result from:
• Trauma
• Metabolic disturbances
• Ingestion
• Infection
158.
Seizures
• Physical manifestationof a seizure will
depend on the area of the brain affected.
• Prognosis is linked to the underlying cause.
159.
Seizures
• Types ofseizures
− Generalized seizures involve the entire brain.
− Partial seizures involve only part of the brain.
• Simple partial seizures: No loss of consciousness
• Complex partial seizures: Loss of consciousness
160.
Seizures
• Febrile seizures
−Child must:
• Be age 3 months to 6 years
• Have a fever
• Have no identifiable precipitating cause
− Strongest predictor is a history in a first-degree
relative.
161.
Seizures
• Febrile seizures(cont’d)
− Simple febrile seizures
• Brief, generalized tonic-clonic seizures occurring
without underlying neurologic abnormalities
− Complex febrile seizures
• Longer, focal, or occur with baseline
developmental or neurologic abnormality
162.
Seizures
• Assessment
− Givespecial attention to:
• Compromised oxygenation and ventilation
• Signs of ongoing seizure activity
− Status epilepticus
• Seizure lasting more than 4 to 5 minutes or
consecutive seizures without a return to
consciousness between seizures
163.
Seizures
• Assessment (cont’d)
−As part of history taking, ask about:
• Prior seizures
• Anticonvulsant medications
• Recent illness, injury, or suspected ingestion
• Duration of seizure activity
• Character of the seizure
164.
Seizures
• Management
− Treatmentis limited to supportive care if seizure
has stopped by your arrival.
− Provide 100% supplemental oxygen; bag-mask
ventilation as indicated for hypoventilation.
165.
Seizures
• Management (cont’d)
−For ongoing seizure, open airway.
• Suction for secretions or vomitus.
• Do not attempt ET intubation.
− Measure serum glucose; treat hypoglycemia.
− Consider administering a benzodiazepine.
− Monitor cardiorespiratory status in any postictal
child.
− Reassess frequently for recurrent activity.
166.
Meningitis
• Inflammation orinfection of the meninges
− Viral meningitis: Rarely life threatening
− Bacterial meningitis: Life threatening
• Symptoms vary.
− The younger the child, the more vague.
167.
Meningitis
• May causesepsis
− Characterized by
a rash
• Petechial
• Purpuric
Courtesy of Ronald Dieckmann, MD.
Meningitis
• Perform aglucose check.
• Provide lifesaving interventions as needed,
and transport quickly.
• Patient may need oxygen, airway
management, and ventilation support.
170.
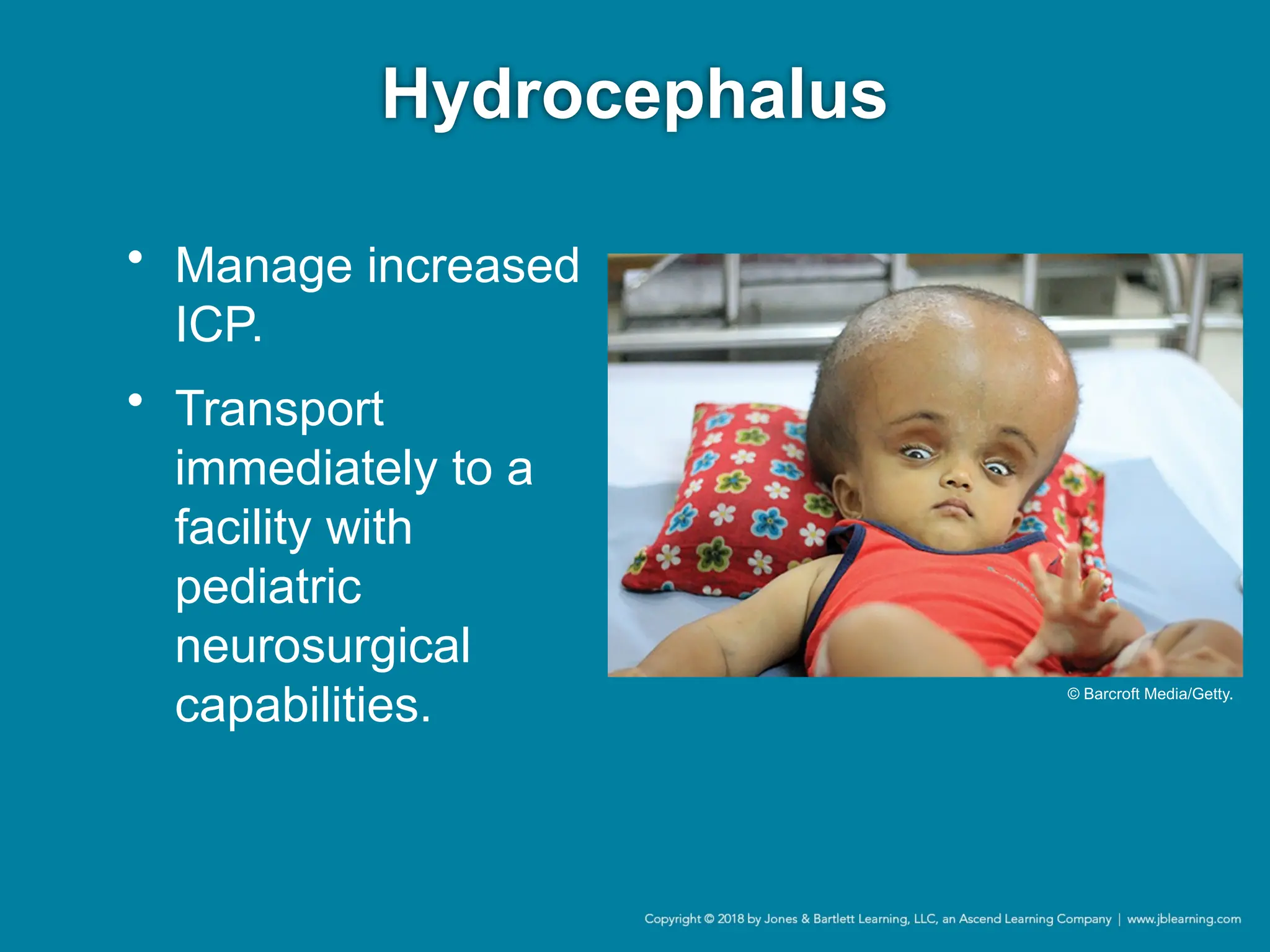
Hydrocephalus
• Results fromimpaired circulation and
absorption of CSF
− Leads to increased ventricles and ICP
• Cerebral shunt often used to decrease ICP
− Ventriculoperitoneal (VP) shunts
− Ventriculoatrial (VA) shunts
171.
Hydrocephalus
• Complications ofcerebral shunts include
infections, blockages, and overdrainage.
• Signs of malfunction include:
− Vomiting
− Headache
− Altered level of consciousness
− Visual changes
Traumatic Brain Injury(TBI)
• Head trauma is common in childhood.
• Small number of children who appear to be
at low risk may have an intracranial injury.
• Evaluate any child with head injury for signs
of potential abuse.
174.
Traumatic Brain Injury(TBI)
• Epidural
hematoma
− Hemorrhage into
space between
the dura and skull
− Child abuse
accounts for
significant number
of cases in infants
and children.
• Subdural
hematoma
− Hemorrhage into
space between
dura and
arachnoid
membranes
− Suspect abuse
until proven
otherwise.
175.
Traumatic Brain Injury(TBI)
• Management includes stabilization of
airway, breathing, and circulation.
• Perform frequent neurologic checks.
176.
Biliary Atresia
• Biliarytract is malformed such that bilirubin
cannot be excreted.
− Leads to liver disease and failure
• Transport children with massive GI bleeds,
obtain IV access, and administer fluid
boluses.
177.
Viral Gastroenteritis
• Infectioncaused by:
− Variety of viruses
− Ingestion of certain foods or substances
• Nausea, vomiting, or diarrhea is likely.
• If you suspect dehydration, administer an
isotonic fluid.
178.
Appendicitis
• Can leadto peritonitis or shock if untreated
• Fever and abdominal pain are common.
• Transport immediately to the ED.
179.
Ingestion of ForeignBodies
• Foreign body lodged in esophagus causes
gagging, vomiting, and difficulty swallowing.
• Difficulty breathing or choking may indicate
airway obstruction.
• Keep child calm and comfortable, and
transport immediately.
180.
Gastrointestinal Bleeding
• Ingested,upper, and lower bleeding may all
present with hematochezia.
− Blood ingested during birth
− Maternal bleeding during breastfeeding
− Ingested blood from epistaxis, after surgery, or
after episodes of forceful vomiting
− Anal fissures from constipation
181.
Intussusception
• Bowel telescopesinto itself.
• Presents with:
− Intermittent severe abdominal pain
− Lethargy
− Bloody or currant jelly–like stools
• Surgical emergency; transport immediately.
182.
Meckel Diverticulum
• Congenitalmalformation of small intestines
• Presents with painless rectal bleeding or
hematochezia
• Presents with the “rule of 2s”
• Transport to the ED for further evaluation.
183.
Pyloric Stenosis and
MalrotationWith Volvulus
• Pyloric stenosis: Pylorus becomes
hypertrophied.
− Presents with projectile vomiting after feedings
− Surgery is curative.
184.
Pyloric Stenosis and
MalrotationWith Volvulus
• Malrotation with volvulus: Twisting of bowel
around mesenteric attachment to the
abdominal wall
− Presents with bilious emesis, pain, and a
distended, rigid abdomen
− Surgical emergency
185.
Assessment and Managementof
Gastrointestinal Emergencies
• Consider the following:
− Age
− Gender
− Whether child was born premature
− Current medication use
− History of similar complaints
186.
Assessment and Managementof
Gastrointestinal Emergencies
• Assess and reassess location and severity
of abdominal pain.
− Premature infants and those with symptoms in
the first weeks of life require further evaluation.
• Give special consideration to patients with
gastrostomy tubes (G-tubes).
187.
Assessment and Managementof
Gastrointestinal Emergencies
• Replacing G-tube:
− Lubricate tube end being inserted.
− Gently press to slide the tube into the stoma.
− Tape replacement into place.
− Transport for definitive replacement.
188.
Assessment and Managementof
Gastrointestinal Emergencies
• To help determine dehydration, ask:
− How many wet diapers has the child had today?
− Is your child tolerating liquids?
− How many times has your child had diarrhea?
− When he or she cries, are there tears present?
• Give nothing to eat or drink until a thorough
assessment can be completed.
189.
Hyperglycemia
• Can resultin severe dehydration and
diabetic ketoacidosis (DKA) if not promptly
treated
• During assessment, you will typically find:
− Dose of insulin was missed.
− Greater proportion of food was eaten.
− Insulin pump malfunctioned.
190.
Hyperglycemia
• During assessment,ask about the following:
− Insulin administration
− Functioning of insulin pump
− Changes in urine output or mental status
− Patterns on recent glucose checks
− Presence of urine ketones
− Any other symptoms
191.
Hyperglycemia
• Provide 100%oxygen or assisted
ventilation if needed.
• Monitor vital signs closely.
• Obtain IV access; administer isotonic fluids.
192.
Hyperglycemia
• If patientreports worsening of a headache
or mental status deteriorates:
− Discontinue fluids.
− Assess and treat for increased ICP.
− Closely monitor the ECG.
193.
Hypoglycemia
• Abnormally lowblood glucose level
− Infants and children have limited glucose stores.
− Can lead to irreversible brain damage
− May occur in patients with diabetes
Hypoglycemia
• Management
− MaintainABCs and establish vascular access.
− Give normal saline at keep-open rate.
• If signs of shock or the child is dehydrated, give a
fluid bolus of normal saline at 20 mL/kg.
• Determine blood glucose level.
• Repeat glucose reading after 10 to 15 minutes.
• Reassess frequently until level stabilizes.
196.
Congenital Adrenal
Hyperplasia (CAH)
•Autosomal-recessive disorder of an enzyme
responsible for the metabolism of cortisol
and aldosterone in the adrenal glands
• Often due to 21-hydroxylase deficiency
197.
Congenital Adrenal
Hyperplasia (CAH)
•Patients sometimes undergo:
− Early pubertal development, pubic hair growth
− Early growth acceleration
− Development of facial hair
− Short stature
− Severe acne
• When child becomes sick, body may not be
able to compensate.
198.
Congenital Adrenal
Hyperplasia (CAH)
•Infants may have vomiting, poor weight
gain, and dehydration.
• If suspected, hydrocortisone and IV boluses
of normal saline are needed.
• Stress-dose steroids should be considered.
199.
Panhypopituitarism
• Hypopituitarism
− Pituitarygland
does not produce
normal amounts of
some or all of its
hormones.
• Panhypopituitarism
− Inadequate
production or
absence of
pituitary hormones
200.
Panhypopituitarism
• When stressedor sick, patients can present
with symptoms similar to CAH.
• Patients require:
− IV fluid boluses with normal saline
− Glucose replacement
− Replacement of steroids with IV hydrocortisone
201.
Panhypopituitarism
• Management bya pediatric endocrinologist
is important.
• Once hormone therapy is initiated, children
can generally live a normal life.
202.
Inborn Errors ofMetabolism
(IEM)
• Group of congenital conditions that cause
either accumulation of toxins or disorders of
energy metabolism in the neonate
• Characterized by:
− Failure to thrive
− Vague signs such as poor feeding
203.
Inborn Errors ofMetabolism
(IEM)
• Grouped into two categories:
− Disorders that result in toxic accumulations
• Maple syrup urine disease, phenylketonuria
− Disorders of energy production or use
• Hereditary fructose intolerance, galactosemia
204.
Inborn Errors ofMetabolism
(IEM)
• Symptoms can vary and include:
− Loss of milestones in development
− Recurring vomiting and diarrhea
− Skin problems
− Dental deformities
− Deafness
− Blindness
205.
Inborn Errors ofMetabolism
(IEM)
• Dietary restrictions and replacements can
control many of these disorders.
• Boluses of glucose and the use of 10%
dextrose (D10) fluids may be necessary.
206.
Hematologic, Oncologic, and
ImmunologicEmergencies
• Common in pediatrics
• Immunosuppression may be due to:
− Congenital diseases of the immune system
− Chronic steroid use
− Chemotherapy
207.
Hematologic, Oncologic, and
ImmunologicEmergencies
• May present with severe illness, shock
• Special considerations include:
− Sepsis
− Acute chest syndrome with sickle cell crisis
− Stroke with sickle cell crisis
− Tumor lysis syndrome
− Increased overall risk of infection
208.
Hematologic, Oncologic, and
ImmunologicEmergencies
• Quickly assess for signs of sepsis and
decompensation.
• Examination should include:
− Lung, circulatory, and neurologic examination
− Evaluation of the extremities for swollen joints
209.
Hematologic, Oncologic, and
ImmunologicEmergencies
• Because some patients have indwelling
catheters, evaluate catheter site for:
− Erythema
− Swelling
− Tenderness
• Can be signs of central line infections
210.
Sickle Cell Disease
•Genetically inherited autosomal-recessive
disorder of red blood cells
− Results in misshapen red blood cells, causing
poor oxygen-carrying capability and potential
lodging of the cells in blood vessels or spleen
− Leads to ischemia and painful crises
211.
Sickle Cell Disease
•Infants may
present with:
− Fussiness
− Irritability
− Crying
− Poor feeding
− Nonspecific
findings
• Older children
may report:
− Pain in specific
locations,
including joints,
back, and chest
212.
Sickle Cell Disease
•Opioids manage the pain from
vasoocclusive episodes.
− Medications sometimes inadequate
− Ask about any medication taken since onset of
present pain.
Bleeding Disorders
• Abnormalityin clotting of the blood
• Development of a thrombosis can occur.
• Symptoms depend on the following:
− Location of clot
− Size of clot
− Whether clot becomes dislodged
215.
Bleeding Disorders
• Considerhow to best control bleeding.
• Fluid replacement with boluses of isotonic
fluids is necessary until patient is at a
hospital.
• Bleeding may be
− Drug induced
− Inherited
− Acquired
Thrombocytopenia
• Treatment includes:
−Treating the underlying cause if present
− Transfusing platelets if bleeding cannot be
controlled
− Transport for consultation with a hematologist
218.
Hemophilia
• Significant decreasein:
− One of the clotting factors
− Proteins in blood that work to help blood to clot
• Child can experience hemorrhage after
minor trauma.
219.
Hemophilia
• Not curable,but treated with replacement of
the missing factor
• When injuries occur, extra factor is often
needed.
• Recognize signs of internal bleeding.
220.
Hemophilia
• Be alertfor signs of cerebral bleeding,
which may include:
− Headache
− Slurred speech
− Altered mental status
• Be alert for signs of GI bleeding
221.
von Willebrand Disease
•Bleeding disorder in which the patient is
missing the von Willebrand factor (a protein
essential for platelet adhesion)
− Prevents blood clotting
• Most people with disease are undiagnosed.
222.
von Willebrand Disease
•Range from mild (nosebleeds) to severe
uncontrolled bleeding tendencies
• Treatment
− Control bleeding.
− Transport to a hospital with hematology
services.
223.
Leukemia/Lymphoma
• Two formsof leukemia are recognized:
− Acute lymphoblastic leukemia
− Acute myelogenous leukemia
• Few symptoms displayed at onset.
224.
Leukemia/Lymphoma
• Treatment ofleukemia/lymphoma involves:
− Use of IV chemotherapy
− Radiation therapy
• These patients may require supportive care
and pain management en route to a facility.
225.
Toxicologic Emergencies
• Toxicexposures
account for a
significant number
of pediatric
emergencies.
− Ingestion
− Inhalation
− Injection
− Application
226.
Assessment of Toxicologic
Emergencies
•Evaluation follows standard assessment
sequence.
• Attend to ABCDEs as indicated.
− Treat documented hypoglycemia.
• If child is stable, obtain additional history
and perform secondary assessment.
227.
Assessment of Toxicologic
Emergencies
•Look for toxidromes by assessing:
− Mental status
− Pupillary changes
− Skin CTC
− GI activity
− Abnormal odors
• Reassess frequently.
228.
Management of Toxicologic
Emergencies
•Begin with supportive care and ABCDEs.
• Other options include:
− Reduce absorption by decontamination.
− Enhance elimination.
− Provide an antidote.
229.
Management of Toxicologic
Emergencies
•If you are unsure about an exposure, call
the national Poison Center hotline.
− Available 24 hours a day
− 1-800-222-1222
230.
Decontamination
• With skin
exposure,remove
all clothing and
wash skin.
• With ocular
exposure, wash
out the eyes.
• For ingested
toxins, options to
reduce gastric
absorption include:
− Dilution
− Gastric lavage
− Activated charcoal
231.
Decontamination
• For substancesthat are renally excreted,
diuresis may be beneficial.
• Dialysis is required for some overdoses:
− Salicylates
− Lithium
− Methyl alcohol
− Ethylene glycol
− Barbiturates
232.
Decontamination
• If inhaled,assess respiratory status.
− Bronchodilators may be needed for bronchial
irritation and bronchospasm.
− Monitoring of oxygen saturations and intubation
may be necessary.
233.
Enhanced Elimination
• Catharticsare sometimes combined with
activated charcoal.
− Work by speeding up elimination
− Not recommended for young children
234.
Antidotes
• Available foronly a
few poisons
• Reverse or block
effects of ingested
toxins
• Dose depends on
child’s weight
235.
Psychiatric and Behavioral
Emergencies
•As a paramedic, you will encounter children
with behavioral and psychiatric problems.
• Increased calls for behavioral emergencies
236.
Psychiatric and Behavioral
Emergencies
•Problems begin as simple complaints not
recognized by health care providers.
− Improperly treated problems persist into
adulthood.
− Children often have coexisting problems along
with traditional mental health disorders.
237.
Safety
• Safety isyour first priority.
• Approach the child calmly, and explain you
are there to help.
• Address patient directly.
• Answer questions honestly.
238.
Safety
• Some childrenmust be mechanically
restrained.
− May be a task for EMS or law enforcement
− Carefully document the reason.
− Keep restraints in place until arrival at the ED.
239.
Assessment and Managementof
Psychiatric and Behavioral
Emergencies
• Mental health problems in children are
difficult to diagnose.
• Causes are:
− Organic
− Genetic
− Environmental
240.
Assessment and Managementof
Psychiatric and Behavioral
Emergencies
• Abnormal findings are often related to:
− Adjustment disorders
− Stress
• Assessment of any child must include
suicide risk.
241.
Assessment and Managementof
Psychiatric and Behavioral
Emergencies
• PAT will give you a general impression of
mental status and cardiovascular stability.
• Assessment is based on observation and
history.
• Treat problems or injuries with standard
protocols.
242.
Fever Emergencies
• Feveris a common pediatric complaint.
− Symptom of infectious or inflammatory process
− Can have multiple causes
• General impression and primary survey will
help determine severity.
243.
Fever Emergencies
• Recordtemperature.
• Life-threatening signs may include:
− Respiratory distress
− Seizures
− Petechial or purpuric rash
− Bulging fontanelle in an infant
244.
Fever Emergencies
• Historytaking and secondary assessment
will help determine the underlying cause
and severity of illness.
− Perform on scene if child is stable.
− Perform en route if seriously ill.
245.
Fever Emergencies
• Mayrequire little intervention
− Support ABCs.
− Provide temperature control.
− Transport to an appropriate medical facility.
246.
Child Abuse andNeglect
• Child abuse: Any improper or excessive
action that injures or harms a child or infant
− Physical abuse
− Sexual abuse
− Emotional abuse
− Neglect
247.
Child Abuse andNeglect
• Abandonment
− Occurs when a parent or guardian leaves a
child without regard to the child’s health, safety,
or welfare
− Parents have relinquished consent authority;
EMS providers should render care without
consent.
248.
Risk Factors forAbuse
• Risk factors for abuse
− Younger children
− Children who require extra attention
− Lower socioeconomic status
− Divorce, financial problems, and illness
− Drug and alcohol abuse
− Domestic violence in the home
249.
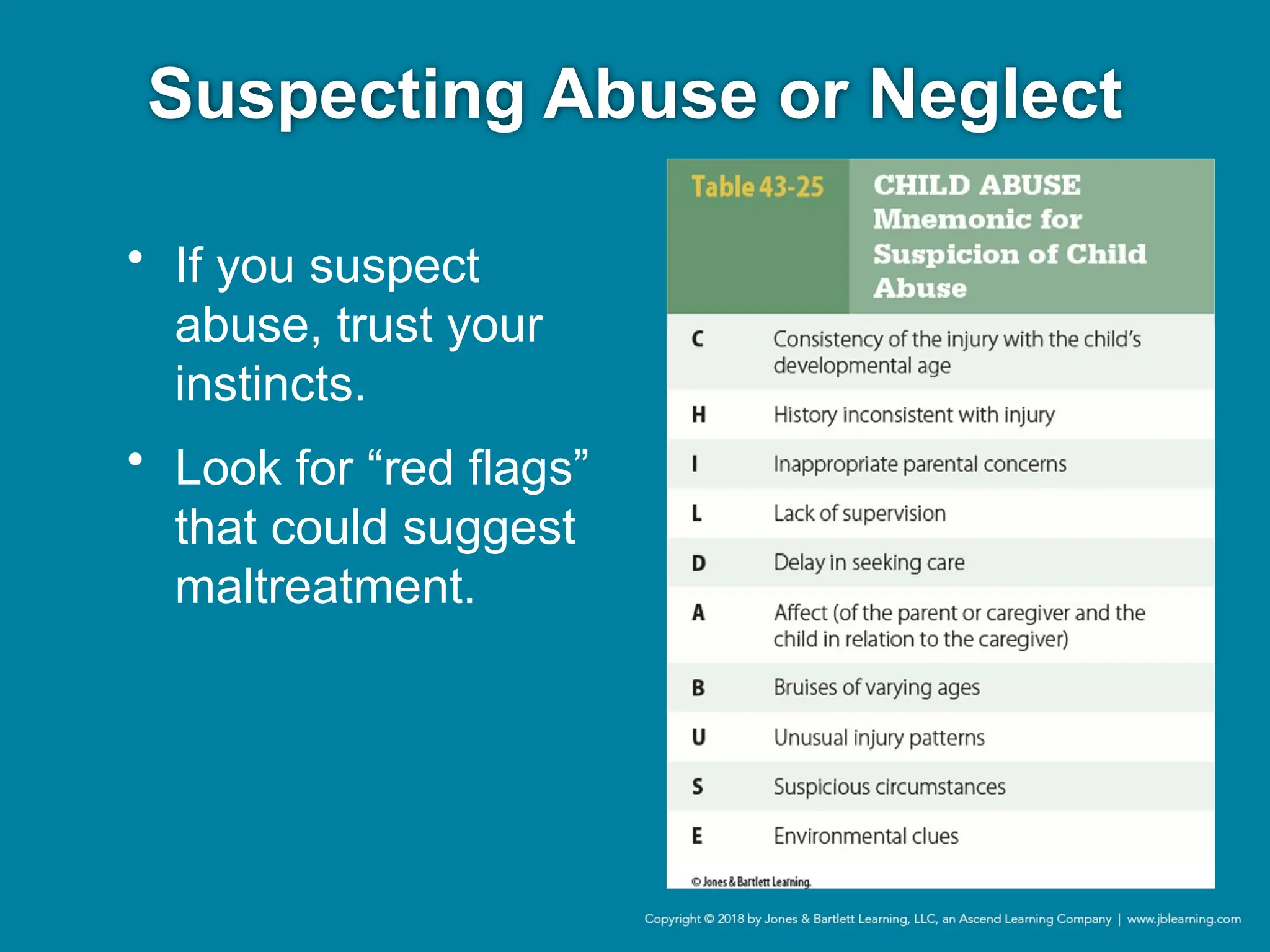
Suspecting Abuse orNeglect
• If you suspect
abuse, trust your
instincts.
• Look for “red flags”
that could suggest
maltreatment.
250.
Assessment and Management
ofAbuse and Neglect
• Carefully document what you see.
− Child’s environment
− Condition of home
− Interactions among caregivers, child, EMS crew
• Prehospital personnel are legally obligated
to report suspicion of abuse.
251.
Assessment and Management
ofAbuse and Neglect
• Involve police early to secure the scene.
• Approach ED staff with concerns.
• Be aware of local regulations.
• Focus on assessment and management.
252.
Assessment and Management
ofAbuse and Neglect
• Be alert for a
history that is
inconsistent with
the clinical picture.
• Look for bruises.
− Different stages of
healing
− Concerning
locations
Courtesy of Moose Jaw Police Service.
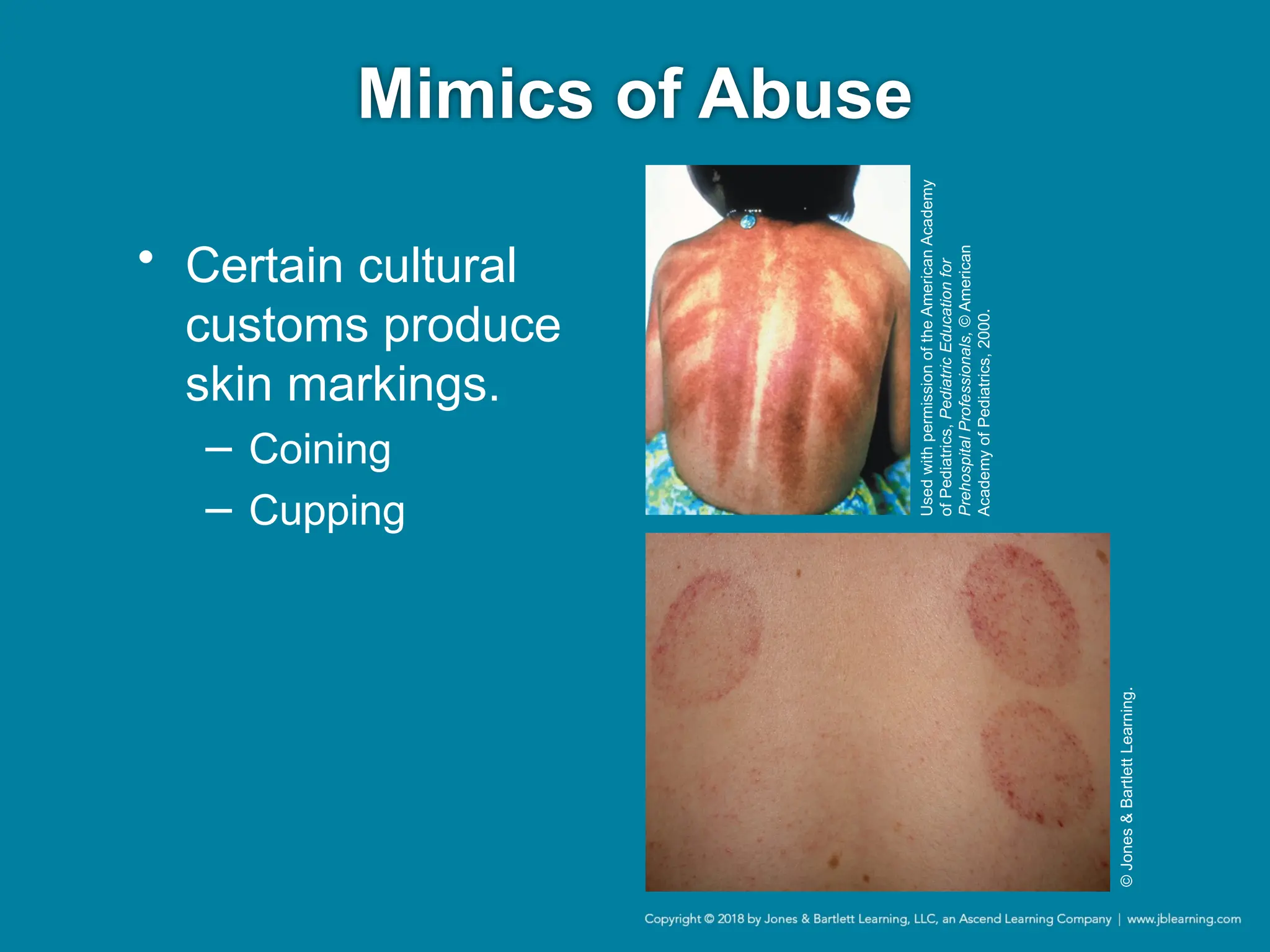
Mimics of Abuse
•Medical conditions can mimic bruises.
− Purpura
− Petechiae
• Exposure to sun can cause reactions with
certain medications or fruits.
− Phytophotodermatitis
Sudden Infant DeathSyndrome
(SIDS)
• Sudden unexpected infant death (SUID)
− Death of an infant younger than 1 year that
occurs unexpectedly, the cause of which is not
immediately obvious before investigation
257.
Sudden Infant DeathSyndrome
(SIDS)
• Most SUIDs are one of three types:
− Sudden infant death syndrome (SIDS)
− Unknown cause
− Accidental suffocation and strangulation in bed
258.
Assessment and Management
ofSIDS
• Be alert to other potential causes of death.
• Decision to start or stop resuscitative efforts
can be difficult.
• Thorough scene size-up and history are
important.
259.
Brief Resolved Unexplained
Event(BRUE)
• Episode during which an infant:
− Becomes pale or cyanotic;
− Chokes, gags, or has an apneic spell; or
− Loses muscle tone
• Causes range from benign to serious
diagnoses.
260.
Brief Resolved Unexplained
Event(BRUE)
• Provide life support with signs of
cardiorespiratory compromise or altered
mental status.
• Transport all infants with a history of BRUE.
261.
Pediatric Trauma Emergencies
•Anatomy and physiology make injury
patterns and responses different from those
seen in adults.
• Developmental stage will affect response.
262.
Pathophysiology of Traumatic
Injuries
•Blunt trauma is the MOI in most pediatric
injury cases.
− Less muscle and fat mass leads to less
protection against forces transmitted.
263.
Pathophysiology of Traumatic
Injuries
•Falls are common.
• Injury will reflect child’s anatomy and height
of fall.
− Falls from a standing position usually result in
isolated long bone injuries.
− High-energy falls result in multisystem trauma.
− Injuries from bicycle handlebars typically
produce intraabdominal compression injuries.
264.
Pathophysiology of Traumatic
Injuries
•Motor vehicle crashes can result in a variety
of injury patterns depending on restraints
and position in car.
− For unrestrained passengers, assume
multisystem trauma.
− Suspect spinal fractures with chest or
abdominal bruising in a seat belt pattern.
265.
Assessment and Management
ofTraumatic Injuries
• Begin with a thorough scene size-up.
• Use PAT to form a general impression.
− If findings are grossly abnormal, move to ABCs.
• Initiate life support interventions.
266.
Assessment and Management
ofTraumatic Injuries
• Pneumothorax may be present with
penetrating trauma of the chest or upper
abdomen.
− Perform needle decompression.
− Signs and symptoms may include:
• Tachycardia
• Jugular vein distention
• Pulsus paradoxus
Assessment and Management
ofTraumatic Injuries
• Any trauma patient should be considered at
risk for developing shock.
• Once ABCs are stabilized, continue
assessment of disability with AVPU.
269.
Assessment and Management
ofTraumatic Injuries
• Place a cervical collar, and immobilize on a
long backboard as indicated.
• Perform rapid exam to identify all injuries.
• Cover the child with blankets.
• Treat any fractures.
270.
Transport Considerations
• Sometraumas are load-and-go because of
severe injuries and unstable condition.
• For these situations:
− Perform lifesaving steps on scene or en route.
− Transfer quickly per local trauma protocols.
History Taking andSecondary
Assessment
• If patient is stable:
− Obtain additional history.
− Perform a more thorough physical exam.
• Look for bruises, abrasions, other subtle signs of
injury that may have been missed.
273.
Fluid Management
• Airwaymanagement and ventilatory support
take priority over circulation management.
− Tachycardia is usually the first sign of circulatory
compromise in a child.
− Hypotension is a late finding.
274.
Fluid Management
• Establishingvascular access
− Large-bore IV catheters should be inserted into
a large peripheral vein.
− 20- or 22-gauge needles may be considered
“large bore.”
− Definitive care can only be provided at the ED.
− To maintain perfusion, administer a bolus of 20
mL/kg of isotonic crystalloid solution.
275.
Pain Management
• Painis often undertreated in children.
− Use tools to elicit child’s self-report of pain level.
− Use a calm, reassuring voice, distraction
techniques, and medications when appropriate.
− Children who are in shock and
hemodynamically unstable are not good
candidates for narcotics or sedatives.
276.
Pathophysiology, Assessment,
and Managementof Burns
• Assessment and management are similar to
that of adults, with a few key differences.
− Higher skin surface–body mass ratio
− Worrisome patterns of injury or suspicious
circumstances should raise concerns of abuse.
277.
Assessment and Management
ofBurns
• Scene safety is important.
• Estimate the percentage of BSA burned.
− Adolescents: Use rule of nines.
− Younger children: Modify to account for larger
head size.
− Infants: Head and trunk each account for 18%
of BSA; arms 9%; legs 13.5% each.
278.
Assessment and Management
ofBurns
• Burns suggestive of abuse:
− Mechanism or pattern observed does not match
history or child’s capabilities.
• Remove burning clothing and support
ABCs.
− Give 100% supplemental oxygen.
279.
Assessment and Management
ofBurns
• Clean burned areas minimally.
• Avoid lotions or ointments.
• Cover burn and patient as needed.
• Analgesia is a crucial part of management.
• Transport to an appropriate medical facility.
280.
Children with SpecialHealth
Care Needs
• Includes children with physical,
developmental, and learning disabilities
• Broad range of causes
281.
Tracheostomy Tubes and
ArtificialVentilators
• Tracheostomy:
− Surgical creation of a
stoma through which
a tracheostomy tube
can be placed for
long-term ventilatory
needs
Courtesy
of
Cindy
Bissell.
282.
Tracheostomy Tubes and
ArtificialVentilators
• Caregivers are a source of valuable
information.
• Child may depend on a home ventilator and
supplemental oxygen.
• Most common problem is obstruction of
tube with secretions.
• With respiratory distress, assess tube
position and suction tube.
Central Venous Catheters
•May be inserted for long-term IV access for
medications or nutrition
• Complications include infections,
obstruction, and dislodged or broken
catheters.
Ventricular Shunts
• Shuntobstructions and infections are
medical emergencies.
− Transport for neurosurgical evaluation.
− Maintain continuous cardiopulmonary
monitoring during transport.
287.
Assessment and Managementof
Children With Special Health Care
Needs
• Follow standard assessment sequence.
• Ask questions to establish baseline
neurologic function and physiologic status.
• Meet child at his or her developmental level.
• Work with parents to restore child to his or
her own physiologic baseline.
288.
Transport of ChildrenWith
Special Health Care Needs
• Transport to the child’s medical home.
− If this is not possible, take along any medical
records and assistive devices.
− Most important, take the caregiver!
289.
An Ounce ofPrevention
• Emergency care for children involves a
team approach by health professionals.
• To be an effective child safety advocate,
you must be knowledgeable about local and
national prevention programs.
290.
Emergency Medical Services
forChildren
• Federally funded program created to reduce
child disability and death
− Works with local communities and hospitals to
improve care in and out of the ED
− Supports training in pediatric-specific
emergency care
291.
Prevention of Injuries
•Most injuries are preventable.
• Tracking injury patterns helps target areas
for intervention and prevention.
#2 Lecture Outline
I. Introduction
A. Children differ from adults in their anatomy, physiology, and emotions and experience a range of illnesses and injuries.
1. Children perceive their illness or injury differently than adults.
2. Young children may not be able to report what is bothering them.
3. Fear or pain may hamper assessment.
4. Stressed or frightened parents and caregivers may also pose challenges.
5. Your approach to pediatric patients must be based on their age and accommodate their unique developmental and social issues.
#3 Lecture Outline
II. Developmental Stages
A. Neonate and infant
1. Neonatal period: First month of life
2. Infancy: First 12 months of life
3. Respect caregiver’s perception that “something is wrong.”
a. Watch for persistent crying, irritability, and lack of eye contact.
b. May be a symptom of a serious problem, such as:
i. Bacterial infection
ii. Cardiac problem
iii. Depressed mental status
iv. Electrolyte disturbance
4. Nonspecific concerns about behavior, feeding, sleep pattern, or arousability can indicate a serious underlying illness or injury.
5. Increased mobility can lead to injury.
6. Consider possible abuse with behaviors that do not match developmental stage.
#4 Lecture Outline
7. Considerations for patient assessment:
a. Choose the best location.
b. Keep child warm.
c. Support a young infant’s head and neck.
d. Older infants in stable condition will be calmest in a parent’s arms.
e. Warm hands, stethoscope.
f. Be opportunistic with exam, use a soft voice, smile.
g. If child is quiet, listen to heart and lungs first.
h. A pacifier or gloved finger to suck on may quiet a crying child.
i. Jingling keys or shining a penlight may distract an older infant.
j. No small objects
i. Risk of aspiration
#5 Lecture Outline
B. Toddler
1. Toddler period includes ages 1 to 2 years.
a. Includes the “terrible twos”
b. Not capable of reasoning
c. Poorly developed sense of cause and effect
d. Language development is occurring rapidly
e. Growing ability to crawl, walk, run, and climb
f. Painful procedures may make lasting impressions.
#6 Lecture Outline
2. Use the Pediatric Assessment Triangle (PAT) to assess the child.
3. Strategies for examining a toddler include the following:
a. Examine a toddler in stable condition on parent’s lap.
i. Avoids separation anxiety
b. Get down to the child’s level.
c. Talk to the child.
d. Have a parent assist when possible.
e. Use play and distraction when possible.
f. Offering choices helps child feel in control.
g. Consider saving upsetting or painful steps for last.
h. Be flexible—full head-to-toe exam may not be possible.
#7 Lecture Outline
C. Preschool-age child
1. Ages 3 to 5 years
2. Rapidly becoming verbal and active
a. Can understand directions
b. Generally able to tell you what hurts
c. Choose words carefully; preschoolers are literal.
d. Use plain language, provide lots of reassurance; fears are common.
3. Curious, want to cooperate
4. Respect modesty by keeping them covered.
5. Let child participate or hold equipment that is safe.
6. Offer simple choices.
7. Avoid procedures on the dominant hand or arm.
8. Set limits on behavior if the child acts out.
#8 Lecture Outline
D. School-age child (middle childhood)
1. Ages 6 to 12 years
2. Capable of abstract thought; understand cause and effect.
3. School is important; focus on popularity and peer pressure.
a. Children with chronic illness or disabilities can be self-conscious.
4. Understanding of death may increase anxiety.
5. They may have their own ideas about medical care.
6. By age 8 years, anatomy and physiology are similar to those of adults.
a. Breasts develop between ages 8 and 13 years.
b. Menstrual period begins between ages 9 and 16 years.
c. Testicles increase in the size around age 10 years.
d. May be self-conscious about body image
7. Ask child to describe history and symptoms.
8. Explain steps in simple language; answer questions.
9. Offer appropriate choices and control, reassurance, encouragement.
10. Provide simple explanations about causes and treatment of pain.
11. Respect modesty.
12. Asking about school, pets, and so on may provide a distraction.
13. Rewarding the child after completing a procedure can help.
#9 Lecture Outline
E. Adolescence
1. Ages 13 to 18 years
2. Can be difficult; teens are struggling with independence, as well as social and personal issues.
3. Once secondary sexual characteristics have developed (breasts or facial/axillary hair), treat an adolescent as an adult.
a. With respect CPR and foreign body airway obstruction procedures
4. During assessment, address and reassure the patient.
a. Alienating the patient may interfere with assessment and treatment.
b. Encourage questions and involvement.
c. Address all concerns and fears.
d. Provide accurate information.
e. Respect patient privacy.
f. If possible, address the adolescent without a caregiver present.
i. Especially about sensitive topics such as sexuality or drug use
ii. Patient may want friends present.
5. Let patient have as much control as appropriate.
#10 Lecture Outline
III. Pediatric Anatomy, Physiology, and Pathophysiology
A. Anatomic and physiologic differences can create difficulties with your assessment if you do not understand them.
B. The head
1. Infants’ and young children’s heads are large relative to the rest of their bodies.
a. An infant’s head is two-thirds its adult size.
b. Large surface area means more mass relative to the rest of the body.
c. Important factor in the incidence of head injuries
i. Tend to lead with their head in a fall
2. Take care when positioning the airway.
a. Seriously injured, younger than 2 years: Place a thin layer of padding under the shoulders or upper torso to obtain neutral position.
b. Seriously ill, younger than 2 years: Place a folded sheet under occiput to obtain sniffing position
3. Keep covered for warmth.
4. During infancy, the anterior and posterior fontanelles are open.
a. Areas where the infant’s skull bones have not fused together
b. Allow compression of the head during birth and rapid growth of the brain
c. Posterior fontanelles close by age 4 months.
d. Anterior fontanelles close by age 2 years.
e. Important anatomic landmark when assessing a sick or injured infant
i. Bulging suggests increased intracranial pressure (ICP).
ii. Sunken fontanelles suggest dehydration.
#11 Lecture Outline
C. The neck and airway
1. Children have short, stubby necks.
a. Can be difficult to feel carotid pulse or see jugular veins
2. Airway is much smaller than an adult airway.
a. More prone to obstruction by:
i. Foreign body inhalation
ii. Inflammation with infection
iii. Disproportionately large tongue
3. During the first few months of life, infants are obligate nose breathers.
a. Nasal obstruction with mucus can result in significant respiratory distress.
4. Epiglottis:
a. Long and floppy
b. U-shaped
c. Narrow
d. Extends at a 45° angle into the airway
e. Difficult to visualize the vocal cords during intubation
5. Narrowest part of a young child’s airway occurs at the level of the cricoid cartilage.
a. Below the vocal cords, rather than at the vocal cords as in adults
b. Influences your choice of ET tubes
6. Remember the following:
a. Keep nares clear with suctioning in infants younger than 24 months.
b. Tracheal cartilage is softer and more collapsible; avoid hyperextension of neck.
i. May result in reverse hyperflexion, kinking of the trachea
ii. May displace the tongue posteriorly, obstructing the airway
c. Keep the airway clear of all secretions.
i. Even a small amount of particulate matter may cause obstruction.
d. Use care when managing the airway.
i. Jaw is smaller.
ii. Soft tissues are delicate and prone to swelling.
e. Correct positioning can often maintain airway and negate the use of adjuncts.
#12 Lecture Outline
D. The respiratory system
1. Tidal volume is slightly smaller than in adults, but metabolic oxygen demand is doubled.
2. Functional residual capacity is smaller.
a. Smaller oxygen reserves
3. Functional residual capacity: Volume of air in the lungs following exhalation
a. Also referred to as oxygen reserve
4. Infants breathe faster than older children.
a. Lungs can better handle oxygen exchange as child ages.
b. 30 to 60 breaths/min is normal for newborns.
c. Rate for teens is closer to adult range.
5. Higher respiratory rate and oxygen demand raise risk for effects from inhaled toxins.
#13 Lecture Outline
6. Infants use the diaphragm, not chest muscles, during inspiration.
a. Any pressure on the abdomen of an infant or young child can block diaphragm movement, cause respiratory compromise.
7. Young children experience muscle fatigue quicker.
a. Can lead to respiratory failure if a child has had to breathe hard for long periods
8. Infants and children are highly susceptible to hypoxia because of:
a. Decreased functional residual capacity
b. Increased oxygen demand
c. Easily fatigued respiratory muscles
9. Infants and children will develop hypoxia rapidly with apnea and ineffective bagging.
a. Can cause cardiovascular collapse and arrest
b. Use a larger bag if needed.
c. Use only enough pressure to achieve visible chest rise.
d. Bag’s volume should have no less than 450–500 mL.
e. Maintain a pediatric oxygen saturation level of greater than 94%.
f. Take special precautions with children who have uncorrected cardiac disease or certain congenital defects.
i. Increased oxygenation could harm these patient groups.
ii. Clarify the baseline oxygenation rate with parent.
#14 Lecture Outline
E. The cardiovascular system
1. Children rely mainly on pulse rate to maintain adequate cardiac output and compensate for decreased oxygenation.
#15 Lecture Outline
2. Limited but vigorous cardiac reserves.
a. Proportionally larger circulating blood volume compared with adults
b. Absolute blood volume is less, approximately 70 mL/kg.
3. Injured children can maintain blood pressure for longer periods than adults, even though they are in shock (hypoperfusion).
a. Proportionally larger volume of blood loss must occur in children before hypotension develops.
4. Suspect shock when an infant or child presents with tachycardia.
5. Bradycardia usually indicates severe hypoxia.
a. Manage aggressively.
6. Hypotension is an ominous sign.
a. Often indicates impending cardiopulmonary arrest
7. Signs of vasoconstriction can include:
a. Weak peripheral pulses
b. Delayed capillary refill (in children younger than 6 years)
c. Pale, cool extremities
#16 Lecture Outline
8. The heart
a. Circulation in the fetus is very different than in the newborn.
i. Large right-sided forces on the ECG are normal in young infants.
b. During the first year of life, the ECG axis and voltages shift to reflect left ventricular dominance.
c. Cardiac output is rate dependent in infants and young children.
i. Relatively poor ability to increase stroke volume is reflected in their normal pulse rates and in rate response to physiologic stress and hypovolemia.
d. Mediastinum is more mobile than adults.
i. High risk of injury to mediastinal organs
ii. May not be immediately evident on exam
e. Cardiac tamponade can present with muffled heart tones.
f. Cardiac contusions can cause dysrhythmias.
#17 Lecture Outline
F. The nervous system
1. Continually develops throughout childhood
2. Neural tissue and vasculature are fragile, easily damaged, and prone to bleeding from injury.
3. Brain and spinal cord are not as well protected.
4. Subarachnoid space is relatively smaller.
a. Less cushioning effect for the brain
b. Head momentum may cause bruising and damage.
i. Eg, “shaken baby syndrome”
5. Pediatric brain requires nearly twice the cerebral blood flow as an adult’s.
a. Makes even minor injuries significant
b. Increases risk of hypoxia
i. Hypoxia and hypotension exacerbate head injuries.
6. Brain continues to develop rapidly after birth.
a. Responses become more organized and purposeful.
#18 Lecture Outline
7. The spinal column
a. In young children, the cervical spine fulcrum is higher because head is heavier.
i. Closer to C1-C2
b. Fulcrum descends to “adult level” as the child develops.
i. Around C5 through C7
c. Infant who sustains blunt head trauma involving acceleration-deceleration forces is at high risk for a fatal, high cervical spinal injury.
d. School-age child will likely sustain a lower cervical spinal injury, may be paralyzed.
8. Vertebral fractures and spinal cord injuries in young children are uncommon.
a. Spinal ligaments and joint capsules are more lax.
i. Increased mobility and cord injury in the absence of identifiable vertebral bony fracture or dislocation
b. Vertebral bodies are aligned anteriorly and can slide forward.
i. Potential for cord damage with significant forward flexion.
9. Thoracic and lumbar spinal injuries are relatively uncommon.
a. Seen in children in association with specific mechanisms:
i. Seat belt-associated lumbar spine injuries (often associated with abdominal injury)
ii. Compression fracture due to axial loading in a fall
b. With a significant MOI:
i. Assume cervical spine injury.
ii. Transport with spinal immobilization.
#19 Lecture Outline
G. The abdomen and pelvis
1. The abdominal organs of an infant or child are susceptible to injury.
2. Abdominal wall is thin.
a. Organs closer to the surface
3. Children have:
a. Proportionally larger solid organs
b. Less subcutaneous fat
c. Less protective abdominal musculature
4. Abdominal distention in a healthy infant is due to two factors:
a. Weak abdominal muscles
b. Larger solid organs
5. Liver and spleen extend below rib cage in young children.
a. Less protected by rib cage
b. Rich blood supply, so injuries can result in significant blood loss
6. Kidneys are also more vulnerable to injury.
a. More mobile
b. Less well supported
c. Lower ribs do not shield them from injury.
d. Less protection due to:
i. Underdevelopment of abdominal wall
ii. Lack of fat surrounding organs
7. Duodenum and pancreas are likely to be damaged in handlebar injuries.
8. The organs become more proportional in size and better protected as child grows.
9. Pelvic fractures are uncommon.
a. Generally seen only with high-energy MOIs
#20 Lecture Outline
H. The musculoskeletal system
1. Reaching adult height requires active bone growth.
2. Growth plates (ossification centers) of a child’s bones:
a. Made of cartilage
b. Relatively weak
c. Easily fractured
3. Bones of growing children are weaker than their ligaments and tendons.
a. Makes fractures more common than sprains.
4. Joint dislocations without associated fractures are not common.
5. Most growth plates will be closed by late adolescence.
6. Growth plate fractures
a. Can be seen with low-energy MOIs
#21 Lecture Outline
7. Slipped capital femoral epiphysis (SCFE) is a problem in the hip that affects the epiphysis of the femur.
a. Occurs in children and adolescents
b. Prominently found in overweight children
c. Considered a pediatric disease
d. A gradual-onset condition unless there are signs of trauma
e. Symptoms include:
i. Difficulty in walking and a noticeable limp
ii. Inability to bear weight on limb
iii. Painful and limited normal flexion and rotation
8. Stabilize all sprains or strains, and suspect fractures.
a. Growth plate injuries may result in poor bone growth.
#22 Lecture Outline
I. The chest and lungs
1. Chest wall is quite thin.
a. Less musculature and subcutaneous fat to protect ribs and organs
2. Ribs are more pliable and flexible than an adult’s.
a. Can lead to significant intrathoracic injury with minimal external findings
3. Have fewer rib fractures and flail chest events.
4. Injuries to thoracic organs may be more severe.
a. More vulnerable to:
i. Pulmonary contusions
ii. Cardiac tamponade
iii. Diaphragmatic rupture
5. Lungs are prone to pneumothorax from excessive pressures during bag-mask ventilation.
6. Look for signs of chest injuries with suspected chest trauma.
a. Note that signs of pneumothorax or hemothorax in children are often subtle.
b. May not see signs such as jugular vein distention
c. May be difficult to determine tracheal deviation
d. Be suspicious of bruising to the chest and torso in nonambulatory children.
i. Highly suspicious for nonaccidental trauma
#23 Lecture Outline
J. The integumentary system
1. Infants and children have:
a. Thinner, more elastic skin
b. Higher body surface area (BSA)–weight ratio
c. Less subcutaneous tissue
2. These factors contribute to:
a. Increased risk of injury following exposure to temperature extremes
b. Increased risk of hypothermia (can complicate resuscitative efforts) and dehydration
c. Increased severity of burns
i. Burns that would be minor or moderate in adults are severe in children.
#24 Lecture Outline
K. Metabolic differences
1. Limited stores of glycogen and glucose are rapidly depleted.
a. Be suspicious of hypoglycemia.
b. Check blood glucose levels with lethargy, seizures, or decreased activity.
2. Highly susceptible to hypothermia due to lowered glucose.
a. BSA-to-weight ratio further increases risk.
3. Significant hypovolemia and electrolyte derangements are more common as a result of severe vomiting and diarrhea.
4. Keep the child warm during transport.
#25 Lecture Outline
IV. Parents of Ill or Injured Children
A. The majority of children will have at least one caregiver present, meaning you will be dealing with more than one patient.
1. Serious illness or injury to a child is one of the most stressful situations for caregivers.
a. They may react with anger or fear.
2. Establishing a rapport with caregivers is vital.
a. Source of important information and assistance.
b. Children look to their parents when they are frightened and often mimic their response.
3. Approach caregivers in a calm, quiet, professional manner.
a. Enlist their help in caring for the child.
b. Explain what you are doing.
c. Provide honest reassurance and support.
d. Do not blame the parent.
e. Transport at least one caregiver with the child.
4. Comfort an emotional parent, but remember that your first priority is the child.
a. Do not let a distraught or aggressive parent interfere with your care.
b. Enlist the help of other family members or law enforcement if needed.
#26 Lecture Outline
V. Pediatric Patient Assessment
A. Differs somewhat with pediatric patients.
1. Adapt your assessment skills.
2. Use age-appropriate equipment.
3. Review age-appropriate vital signs.
#27 Lecture Outline
B. Scene size-up
1. Prepare for a pediatric scene size-up, equipment use, and assessment.
a. Collect information from dispatch.
i. Age and sex of the child
ii. Location of the scene
iii. Nature of illness (NOI) or MOI
#28 Lecture Outline
b. Take appropriate standard precautions.
i. Observe for hazards.
ii. Resist the temptation to hastily approach the patient because you know the patient is a child.
c. Note child’s position.
d. Look for clues to MOI or NOI.
e. When a child is unable to communicate or is unresponsive, assume MOI was significant enough to cause head or neck injuries.
i. Immobilize spine with a cervical collar.
ii. Place a pad under head and/or shoulders to facilitate airway management.
f. Note any pills, medicine bottles, alcohol, drug paraphernalia, or household chemicals that would suggest toxic exposure or possible ingestion.
g. Observe the scene or vehicle for clues to the potential severity of any injuries.
#29 Lecture Outline
h. Other important assessments:
i. Orderliness, cleanliness, and safety of the home
ii. General appearance of other children in the family
iii. Presence of any medical devices used for the child
iv. Indications of parental substance abuse
i. Determine whether additional resources are necessary.
#30 Lecture Outline
C. Primary survey
1. Use the PAT to form a general impression.
a. Helps you form a “from-the-doorway” impression and distinguish between sick and not-sick patients.
i. Standardized approach with three elements—appearance, work of breathing, and circulation
(a) Paints an accurate clinical picture of cardiopulmonary status and level of consciousness
(b) Conducted prior to assessing ABCDEs
(c) Does not require touching the patient
(d) Rapid, hands-off systematic approach to observing an ill or injured child
(e) Helps establish urgency for treatment or transport
#31 Lecture Outline
b. Appearance
i. Often the most important factor in determining the severity of illness, need for treatment, and response to therapy
ii. Reflects adequacy of ventilation, oxygenation, brain perfusion, body homeostasis, and CNS function
iii. TICLS (tickles) mnemonic highlights the most important features of a child’s appearance:
(a) Tone
(b) Interactiveness
(c) Consolability
(d) Look or gaze
(e) Speech or cry
iv. Observe from a distance, allowing child to interact with caregiver.
v. Use TICLS mnemonic while observing from the doorway.
vi. Delay touching the patient until you have formed a general impression; your touch may agitate the child.
vii. Unless a child is unconscious or critically ill, take your time in assessing appearance by observation.
#32 Lecture Outline
viii. Abnormal appearance may result from numerous physiologic abnormalities:
(a) Inadequate oxygenation or ventilation
(b) Inadequate brain perfusion
(c) Systemic abnormalities or metabolic derangements
(d) Acute or chronic brain injury
ix. A child with a grossly abnormal appearance is seriously ill and requires immediate life-support interventions and transport.
(a) The remainder of PAT plus hands-on assessment (ABCDEs) may help identify the cause, severity, and need for treatment and transportation.
#33 Lecture Outline
c. Work of breathing
i. Often a better assessment of oxygenation and ventilation status than auscultation or respiratory rate
ii. Reflects child’s attempt to compensate for abnormalities in oxygenation and ventilation
iii. Includes listening for abnormal airway sounds and looking for signs of increased breathing effort.
iv. Some abnormal airway sounds can be heard without a stethoscope and can indicate the likely physiology and anatomic location of the breathing problem.
(a) Snoring, muffled or hoarse voice, or stridor can indicate obstruction at the level of the oropharynx, glottis or supraglottic structures, or glottis or subglottic structures, respectively.
(b) May result from croup, bacterial upper airway infections, lodged foreign body, bleeding, or edema
v. Lower airway obstruction is suggested by abnormal grunting or wheezing.
vi. Grunting is a form of auto-PEEP.
(a) Distends the alveoli to promote maximum gas exchange
(b) Involves exhaling against a partially closed glottis
(c) Short, low-pitched sound
(d) Best heard at the end of exhalation
(e) Often mistaken for whimpering
(f) Suggests moderate to severe hypoxia
(g) Seen pneumonia and pulmonary edema
(h) Reflects poor gas exchange because of fluid in the lower airways and air sacs
vii. Wheezing.
(a) Often occurs during exhalation only
(b) Can occur during inspiration and expiration during severe asthma attacks
(c) Often heard only by auscultation, though severe obstruction may result in audible wheezing.
#34 Lecture Outline
viii. Abnormal positioning and retractions are physical signs of increased work of breathing.
ix. Sniffing position: Trying to align the axes of the airways to improve patency and increase airflow.
(a) Often reflects a severe upper airway obstruction
x. Child who refuses to lie down or leans forward on outstretched arms (tripoding) is creating the optimal mechanical advantage to use accessory muscles of respiration.
xi. Retractions:
(a) To observe, expose the chest.
(b) More useful measure of work of breathing in children than in adults because a child’s chest wall is less muscular, so inward excursion of skin and soft tissue between the ribs is more apparent.
(c) May be evident in the supraclavicular area, the intercostal area or substernal area.
xii. Head bobbing: Form of retractions seen only in infants
(a) Use of neck muscles to help breathing during severe hypoxia
(b) Neck extends during inhalation; head falls forward during exhalation.
xiii. Nasal flaring:
(a) Indicates moderate to severe hypoxia
xiv. Combine the characteristics of work of breathing to make your general assessment of oxygenation and ventilation status.
(a) Abnormal airway sounds
(b) Abnormal positioning
(c) Retractions
(d) Nasal flaring
xv. Together with appearance, work of breathing suggests:
(a) Severity of illness
(b) Likelihood that the cause is in the airway or is a respiratory process
#35 Lecture Outline
d. Circulation to skin
i. Determines adequacy of cardiac output and core perfusion.
ii. Reflects overall status of core circulation.
iii. Three characteristics considered:
(a) Pallor
(b) Mottling
(c) Cyanosis
iv. Pallor may be the initial sign of poor circulation or the only visual sign with compensated shock.
(a) Indicates reflex peripheral vasoconstriction that is shunting blood toward the core
(b) May also indicate anemia or hypoxia
v. Mottling reflects vasomotor instability in the capillary beds demonstrated by patchy areas of vasoconstriction and vasodilation.
(a) May also be a physiologic response to a cold environment
vi. Cyanosis is the most extreme visual indicator of poor perfusion or poor oxygenation.
(a) Acrocyanosis, blue hands or feet in an infant younger than 2 months, is distinct from cyanosis.
(1) Normal finding when a young infant is cold
(b) True cyanosis is seen in the skin and mucous membranes.
(1) Late finding of respiratory failure or shock
vii. Combine the three pieces of PAT to estimate severity of illness and the likely underlying pathologic cause.
#36 Lecture Outline
e. Stay or go
i. Use PAT findings to determine whether patient is stable or requires urgent care.
ii. If unstable:
(a) Assess ABCDEs.
(b) Treat life threats.
(c) Transport immediately.
iii. If stable, perform the entire patient assessment process.
#37 Lecture Outline
2. Hands-on primary survey
a. Complete primary survey:
i. Assess ABCDEs and mental status.
ii. Prioritize care and need for transport.
b. Manage threats to ABCs as you find them.
c. ABC steps are the same as with adults.
d. Also assess disability (D) and exposure (E).
e. Estimate child’s weight.
i. Much of your care will depend on child’s size.
ii. Best method is pediatric length-based resuscitation tape measure.
(a) Also provides medication doses and equipment sizes
(b) Estimates weight and height in pediatric patients weighing up to 75 pounds (34 kg).
#38 Lecture Outline
f. Airway
i. Determine whether the airway is open and patient has adequate chest rise with breathing.
ii. If there is potential obstruction from the tongue or soft tissues, position the airway and suction as necessary.
iii. Do not keep the suction tip or catheter in the back of a child’s throat too long because young patients are extremely sensitive to vagal stimuli and the pulse rate may plummet.
#39 Lecture Outline
g. Breathing
i. Involves:
(a) Calculating the respiratory rate.
(b) Auscultating breath sounds.
(c) Checking pulse oximetry.
ii. Count the number of chest rises in 30 seconds and then doubling that number.
iii. Healthy infants may show periodic breathing or variable respiratory rates with short periods of apnea (less than 20).
(a) Counting for only 10 to 15 seconds may give a falsely low respiratory rate.
iv. Know the normal values for the child’s age and put the respiratory rate in context with the rest of the primary survey.
(a) Rapid respiratory rates may reflect high fever, anxiety, pain, or excitement.
(b) Normal rates may occur in a child who has been breathing rapidly with increased work of breathing and is becoming fatigued.
v. Auscultate breath sounds with a stethoscope over the midaxillary line to hear abnormal lung sounds during inhalation and exhalation.
vi. If you cannot determine whether the sounds are being generated in the lungs or upper airway, hold the stethoscope over the nose or trachea and listen.
(a) Listen for adequacy of air movement.
(b) Diminished breath sounds may signal severe respiratory distress.
(c) Auscultation over the trachea may help distinguish stridor from other sounds.
vi. Check pulse oximetry while the child breathes ambient air.
(a) Greater than 94% saturation while breathing room air indicates good oxygenation.
vii. Evaluate pulse oximetry reading in the context of PAT and primary survey.
(a) A child with a normal pulse oximetry reading may be expending increasing amounts of energy and increasing work of breathing to maintain oxygen saturation.
#40 Lecture Outline
h. Circulation
i. Integrate information from PAT.
(a) Cool extremities and delayed capillary refill are common in a child in a cool environment.
ii. Listen to the heart or feel pulse for 30 seconds; double the number to get pulse rate.
iii. Interpret the pulse rate within the context of the overall history and primary survey.
iv. Tachycardia may indicate early hypoxia or shock or a less serious condition such as fever, anxiety, pain, or excitement.
v. Feel for the pulse to ascertain the rate and quality of pulsations.
vii. Start CPR if there is no pulse or a rate less than 60 beats/min with signs of poor perfusion despite oxygenation/ventilation.
viii. After checking the pulse rate, do a hands-on evaluation of skin CTC.
(a) Check whether the hands and feet are warm or cool to the touch.
(b) Evaluate capillary refill time.
(c) Many factors affect capillary refill time:
(1) Body temperature
(2) Position
(3) Preexisting medical conditions
(4) Medication
(5) Age
(6) Cold exposure, frostbite
(7) Vasoconstriction
(8) Injuries to bones and muscles of extremities
(d) To assess capillary refill in newborns and young infants press the forehead, chin, or sternum.
(e) Suspect poor peripheral circulation if the capillary refill takes more than 2 seconds or the nail bed remains blanched.
ix. Abnormal heart sounds are considered normal variants in the pediatric population.
(a) S3 is considered a benign finding, as long as patient has no other signs.
(b) Split S2 is considered benign when the split is associated with respiratory patterns.
(1) If the split S2 is fixed regardless of the respiratory pattern, further evaluation is necessary.
(2) This finding is typically associated with a septal defect.
(c) The point of maximum impulse is not always palpable in infants.
#41 Lecture Outline
i. Disability
i. Use the AVPU scale or Pediatric Glasgow Coma Scale to assess level of consciousness.
ii. Assess pupillary response.
iii. Evaluate motor activity.
iv. Combine this information with PAT results to determine neurologic status.
#43 This table shows the Pediatric Glasgow Coma Scale.
#44 Lecture Outline
j. Exposure
i. Proper exposure is needed to complete the primary survey.
(a) At least partial undress to assess the work of breathing and circulation.
ii. Perform a rapid exam of the entire body to look for unsuspected injuries and anatomic abnormalities.
iii. Avoid heat loss, especially in infants.
#45 Lecture Outline
3. Transport decision
a. Immediate transport or continued assessment and treatment on scene.
i. Immediate transport for trauma with:
(a) Serious MOI
(b) Physiologic abnormality
(c) Potentially significant anatomic abnormality
(d) Scene is unsafe
ii. Manage all life threats, and begin transport.
iii. Attempt vascular access en route.
iv. If the call is for an illness, the decision to stay or go depends on the following factors:
(a) Expected benefits of treatment
(b) EMS system regulations
(c) Comfort level
(d) Transport time
#46 Lecture Outline
D. History taking
1. If the child is unstable conduct history taking and secondary assessment en route to the ED.
a. Goals:
i. Elaborate on chief complaint.
ii. Obtain patient history.
#47 Lecture Outline
E. Secondary assessment
1. May include a full-body examination or a focused assessment and a complete set of baseline vital signs.
a. Full-body examination
i. For infants, toddlers, and preschool-age children start at the feet and end at the head.
ii. For older children and adolescents, use the head-to-toe approach.
iii. Tailor the exam to the child’s age and developmental stage.
b. General principles when assessing a child:
i. Remain calm, patient, and gentle.
ii. Be honest; if something will hurt, say so, but do not elaborate.
iii. Keep children and parents together to ease fear of separation.
iv. Do not neglect a child’s pain.
2. The extent of the examination will depend on the situation and may include the following:
a. Head
i. Look for bruising, swelling, and hematomas.
ii. Significant blood can be lost between the skull and scalp of a small infant.
iii. Fontanelle
(a) Assess the anterior fontanelle in patients younger than 2 years.
(b) Bulging suggests elevated ICP caused by meningitis, encephalitis, or intracranial bleeding.
(c) Sunken appearance suggests dehydration.
b. Pupils
c. Nose
i. Inspect for drainage of blood or fluid.
ii. Note if nasal flaring is present.
iii. Young infants prefer to breathe through their nose, so nasal congestion with mucus can cause respiratory distress.
iv. Gentle bulb suction of the nostrils may bring relief.
d. Ears
i. Look for drainage from the ear canals.
ii. Leaking blood suggests a skull fracture.
iii. Check for bruises behind the ear.
iv. Pus may indicate an ear infection or perforation of the eardrum.
e. Mouth
i. In the trauma patient, look for active bleeding and loose teeth.
ii. Listen for hoarseness and note the presence of drooling.
iii. Note the smell of the breath.
f. Neck
i. Examine the trachea for swelling or bruising.
ii. Note the use of accessory muscles and the presence of a stoma.
iii. Suspect bacterial or viral meningitis if the child cannot move his or her neck and has a high fever.
g. Chest
i. Examine for penetrating injuries, lacerations, bruises, or rashes.
ii. Note the presence of vascular access devices.
iii. In a trauma patient feel the clavicles and every rib for tenderness or deformity.
iv. An infant with rib fractures will often display paradoxical crying.
h. Back
i. Inspect for lacerations, penetrating injuries, bruises, or rashes.
i. Abdomen
i. Inspect for distention.
ii. Palpate gently; watch for guarding or tensing of the abdominal muscles.
iii. Note tenderness or masses.
iv. Look for seat belt abrasions or bruising.
v. Be suspicious of bruising on the abdomen of a nonambulatory child.
(a) Finding is highly suspicious for nonaccidental trauma.
vi. In an infant, a common finding is a range of active tinkling bowel sounds when the stethoscope is placed on the belly.
vii. Percussing an infant’s abdomen might yield a more tympanic sound.
j. Extremities
i. Assess for symmetry.
ii. Compare both sides for color, warmth, size of joints, swelling, and tenderness.
iii. Put each joint through full range of motion while watching for signs of pain, unless there is obvious deformity suggesting a fracture.
k. Capillary refill (in children younger than 6 years)
l. Level of hydration
i. Assess skin turgor.
(a) Note the presence of tenting.
ii. In infants, note whether the fontanelles are sunken or flat.
iii. Ask parent how many diapers the infant has soiled over the last 24 hours.
iv. Determine whether the child is producing tears when crying.
v. Note the condition of the mouth.
(a) Is the oral mucosa moist or dry?
#48 Lecture Outline
3. Attempt to take the child’s blood pressure on the upper arm or thigh.
a. Make sure the cuff has a width two-thirds the length of the upper arm or thigh.
b. One formula for determining the lower acceptable limit in children ages 1 to 10 years: Minimal systolic blood pressure = 70 + (2 × Age in years).
#49 Lecture Outline
4. Pediatric pain
a. Assessment recognized as part of vital signs assessment.
b. Management of pain and anxiety should be a routine part of field care.
c. Inadequate treatment of pain has many adverse effects on the child and family.
i. Misery for the child and caregivers
ii. Interferes with your ability to accurately assess physiologic abnormalities
iii. Children who do not receive appropriate analgesia may be more likely to have exaggerated pain responses to painful procedures.
d. Consider developmental age when assessing pain.
i. The ability to identify pain improves with the age of the child.
ii. In infants and preverbal children, it may be difficult to distinguish crying and agitation due to hypoxia, hunger, or pain.
iii. Further assessment and discussion with caregivers about their perceptions of the child’s pain are essential to identify pain in this age group.
iv. Use pain scales with pictures.
(a) Example: Wong-Baker FACES scale
e. Use distraction techniques with toys or stories, visual imagery, and music.
f. Sucrose pacifiers may reduce pain in neonates.
#50 Lecture Outline
g. Consider pharmacologic methods for reducing pain:
i. Acetaminophen
ii. Opiates
iii. Benzodiazepines
iv. Nitrous oxide
h. Weigh the benefit against the risks of medication administration:
i. Respiratory depression
ii. Bradycardia
iii. Hypoxemia
iv. Hypotension
5. Do not discount the possibility of child abuse when assessing a child.
a. Increase your index of suspicion for abuse when there is/are:
i. Conflicting information from the parents or caregivers
ii. Bruises or other injuries inconsistent with the MOI described
iii. Injuries inconsistent with the child’s age and developmental abilities
b. Observe and note the parents’ or caregivers’ interaction with the child.
i. Do they appear to be appropriately concerned, angry, or indifferent?
ii. Does the child seem comforted by their presence or scared by them?
#51 Lecture Outline
F. Reassessment
1. Includes the following:
a. PAT
b. Patient priority
c. Vital signs
d. Assessment of the effectiveness of interventions
e. Reassessment of the focused exam areas
#52 Lecture Outline
VI. Pathophysiology, Assessment, and Management of Respiratory Emergencies
A. You will frequently encounter respiratory problems in children.
1. Respiratory failure and arrest precede the majority of cardiopulmonary arrests.
2. Early identification and intervention can stop the progression from respiratory distress to cardiopulmonary failure.
B. Respiratory arrest, distress, and failure
1. Infants have limited ability to compensate for respiratory insults and often expend huge amounts of energy to breathe.
2. Older children have developed compensatory skills so they can compensate for days, with adequate oxygen saturation.
3. If the child in respiratory arrest can be resuscitated before cardiac arrest occurs, survival is likely.
#53 Lecture Outline
4. First determine severity.
a. Distress, failure, or arrest
b. Keep anatomic and physiologic respiratory differences in mind.
#54 Lecture Outline
5. Respiratory distress:
a. A compensated state in which increased work of breathing results in adequate pulmonary gas exchange
b. Classified as mild, moderate, or severe
i. Signs of respiratory distress
(a) Pallor or mottled color
(b) Irritability, anxiety, restlessness
(c) Respiratory rate faster than normal for age
(d) Retractions
(e) Abdominal breathing
(f) Nasal flaring
(g) Inspiratory stridor
(h) Grunting
(i) Mild tachycardia
6. Respiratory failure: Patient can no longer compensate by increased work of breathing.
a. Hypoxia and/or carbon dioxide retention occur.
b. Signs may include:
i. Decreased or absent retractions
ii. Altered mental status
iii. Abnormally low respiratory rate
c. Assist ventilations if tidal volume or respiratory effort is inadequate.
7. In respiratory arrest: patient is not breathing spontaneously.
a. Administer immediate bag-mask ventilation with supplemental oxygen to prevent cardiopulmonary arrest.
#55 Lecture Outline
8. Determining whether the patient is in respiratory distress, failure, or arrest will indicate the urgency for treatment and transport.
a. Obtain SAMPLE history on scene or during transport, depending on patient’s stability.
#56 Lecture Outline
9. Respiratory distress is most common and requires only supportive care.
a. Position of comfort, supplemental oxygen
b. Choice of oxygen delivery method depends on the severity of illness and developmental level.
c. As a child becomes fatigued, respiratory distress may progress to respiratory failure.
#57 Lecture Outline
10. Respiratory emergency treatment:
a. Supplemental oxygen.
b. Perform ECG monitoring.
c. Establish IV access.
d. The child’s airway should be managed in the least invasive way possible.
i. Supraglottic airway devices and intubation should be performed only if bag-mask ventilation fails.
#58 Lecture Outline
C. Upper airway emergencies
1. Foreign body aspiration or obstruction
a. Infants and toddlers have a high risk of foreign body aspiration.
b. Small objects and food items can obstruct a young child’s narrow trachea.
i. Frequent items: Peanuts, hot dogs, grapes, balloons, small toys
c. Swallowed foreign bodies can cause respiratory distress.
d. Tongue: Frequently causes mild upper airway obstruction with decreased level of consciousness and diminished muscle tone.
e. Nostrils: Obstructions remain in the nose for a day or two before the child has pain and a foul-smelling nasal discharge.
i. Frequent items: Pencil erasers, candy, and beans
f. Suspect foreign body aspiration with a sudden onset of respiratory distress accompanied by coughing, gagging, stridor, or wheezing.
g. An awake patient with stridor, increased work of breathing, and good color on the PAT has mild upper airway obstruction.
i. Auscultation may reveal fair to good air entry.
ii. Presence of unilateral wheezing can indicate a foreign body lodged in a main stem bronchus.
h. A patient with severe airway obstruction is likely to be cyanotic and unconscious.
i. Poor air entry.
ii. You may not hear stridor owing to minimal airflow through the trachea.
i. Typical SAMPLE history: Previously healthy child with a sudden onset of coughing, choking, or gagging while eating or playing
j. Initial management of mild airway obstruction:
i. Position of comfort
ii. Providing supplemental oxygen as tolerated
iii. Transport to an appropriate facility.
iv. Avoid agitating the child.
j. In cases of a severe airway obstruction, the patient is unable to cough or make any sound.
#59 Lecture Outline
k. Removing a foreign body airway obstruction in responsive infants
i. Deliver five back slaps and five chest thrusts:
(a) Hold the infant facedown, body resting on your forearm. Support the head and face with your hand; keep the head lower than the rest of the body.
(b) Deliver five back slaps between the shoulder blades with the heel of your hand.
(c) Place your free hand behind the head and back, and bring the infant upright on your thigh, sandwiching the infant’s body between your two hands and arms. The head should remain below the level of the body.
(d) Give five quick chest thrusts in the same location and manner as for chest compressions, using two fingers placed on the lower half of the sternum.
(e) Check the airway. If you can see the foreign body, remove it. If not, repeat the cycle as often as necessary. Do not stick your fingers in the mouth to remove an object unless you can see the object.
(f) If the infant becomes unresponsive, begin CPR with compressions, remembering to look in the airway before ventilations each time.
#60 Lecture Outline
l. Removing a foreign body airway obstruction in unresponsive infants
i. If the infant loses consciousness, start CPR beginning with 30 chest compressions (15 compressions if two rescuers are present).
ii. After 30 compressions, look inside the mouth.
iii. If you see the object, remove it. If not, attempt to give 2 breaths.
iv. Continue compressions, always looking in the mouth, and attempting ventilations until the obstruction is relieved.
v. Then, assess for a pulse.
#61 Lecture Outline
m. Removing a foreign body airway obstruction in children
i. The abdominal thrust maneuver (Heimlich maneuver)
(a) Most effective method with a responsive adult or child
(b) Use until the obstructing object is expelled or child becomes unresponsive.
ii. If the child becomes unresponsive:
(a) Position supine and perform 30 chest compressions (15 compressions if two rescuers are present).
(b) Then look inside the mouth.
(c) If you see the object, remove it. If not, attempt to give 2 breaths.
(d) If the first breath does not produce visible chest rise, reopen the airway and reattempt to ventilate.
(e) If both breaths fail to produce visible chest rise, continue chest compressions.
(f) If you are unable to relieve a severe airway obstruction in an unresponsive patient with these basic techniques, proceed with direct laryngoscopy for the removal of the foreign body.
(g) Insert the laryngoscope blade into the mouth. If you see the foreign body, carefully remove it from the upper airway with Magill forceps.
#62 Lecture Outline
2. Anaphylaxis
a. Potentially life-threatening allergic reaction
b. Triggered by exposure to an antigen
c. Food—especially nuts, shellfish, eggs, and milk—and bee stings are among the most common causes.
i. Can also occur with antibiotics and other medications
d. Exposure to the antigen stimulates the release of histamine and other vasoactive chemical mediators from white blood cells, leading to multiple organ system involvement.
e. Onset of symptoms generally occurs immediately after exposure.
i. May include hives, respiratory distress, circulatory compromise, and gastrointestinal symptoms
f. Mild anaphylaxis: May experience only hives and some wheezing.
#63 Lecture Outline
g. Severe anaphylaxis
i. Child may be unresponsive due to respiratory failure and shock.
ii. May have increased work of breathing due to upper airway edema or bronchospasm and poor circulation
iii. Primary survey will usually reveal hives.
iv. Other findings:
(a) Swelling of the lips and oral mucosa
(b) Stridor and/or wheezing
#64 Lecture Outline
h. “Gold standard” treatment for anaphylaxis is epinephrine.
i. Alpha-agonist effect decreases airway edema by vasoconstriction and improves circulation by increasing peripheral vascular resistance.
ii. Beta-agonist effect causes bronchodilation, resulting in improved oxygenation and ventilation.
iii. Give IM.
iv. Dose may be repeated as necessary every 5 to 15 minutes.
v. If several doses are needed, the child may require a continuous IV epinephrine drip.
i. In addition to epinephrine, treatment should include:
i. Supplemental oxygen
ii. Fluid resuscitation
iii. Diphenhydramine (Benadryl)
iv. Bronchodilators
j. Many children with a history of anaphylaxis will have been treated with IM epinephrine by a caregiver before EMS activation.
k. Given the short half-life of this drug, the child should be transported, even if asymptomatic on your arrival.
#65 Lecture Outline
3. Croup (laryngotracheobronchitis)
a. Viral infection of the upper airway
b. Transmitted by respiratory secretions.
c. Primarily affects children between ages 6 months to 6 years
d. Most cases occur in fall and winter.
e. Causes edema and progressive airway obstruction.
f. The hallmark sign of croup—stridor.
g. SAMPLE history usually reveals several days of cold symptoms and low-grade fever, followed by barky cough, stridor, and trouble breathing.
h. The cough and respiratory distress are often worse at night.
i. Severity ranges from mild to severe.
i. Mild: Absence of stridor at rest, minimal respiratory distress, and an occasional cough
ii. Moderate: Behavior and mental status are normal but inspiratory stridor and retractions are present at rest and the amount of respiratory distress is increased.
iii. Severe: Mental status changes are present accompanied by significant respiratory distress and decreasing air entry.
#66 Lecture Outline
j. Initial management:
i. Position of comfort
ii. Avoid agitating the child.
iii. The use of humidified oxygen or mist therapy is not indicated.
iv. A steroid, such as dexamethasone, may be administered IV or IM.
v. Nebulized epinephrine is the treatment of choice with any of the following:
(a) Stridor at rest
(b) Moderate to severe respiratory distress
(c) Poor air exchange
(d) Hypoxia
(e) Altered appearance
k. Croup and respiratory failure
i. Nebulized epinephrine alone may not be adequate.
ii. Assisted ventilation with bag-mask ventilation may be necessary.
l. Advanced airway placement
i. Rarely needed
ii. Choose an ET tube one-half to one size smaller than normal for age or size to accommodate the subglottic edema.
m. Children requiring nebulized epinephrine or assisted ventilation need to be transported immediately.
#67 Lecture Outline
4. Epiglottitis
a. Life-threatening condition that causes the epiglottis and supraglottic tissues to swell
b. Can affect any age group, but most prevalent in 2- to 7-year olds.
c. Incidence fallen sharply due to routine administration of Haemophilus influenzae type b vaccine to children.
d. Classic presentation:
i. Sick, anxious, and sitting upright in the sniffing position.
ii. Drooling.
iii. Increased work of breathing.
iv. Pallor or cyanosis.
e. Signs of a significant airway obstruction:
i. Stridor heard on auscultation over the neck
ii. Muffled voice
iii. Decreased or absent breath sounds
iv. Hypoxia
f. SAMPLE history will reveal a sudden onset of high fever and sore throat.
#68 Lecture Outline
g. Symptoms progress rapidly.
h. Ask about immunizations.
i. Get the child to an appropriate hospital with a maintainable airway.
j. Minimize on-scene time, and do not attempt procedures that might agitate the child.
k. Allow the patient to assume a position of comfort; provide supplemental oxygen only if tolerated.
l. Do not attempt to look in the mouth or insert an IV line because this can agitate the child and worsen his or her respiratory distress.
m. Be prepared with a bag-mask device and an ET tube one to two sizes smaller than anticipated in the event of complete obstruction during transport.
n. Some uncommon conditions can also cause upper airway obstruction, including:
i. Retropharyngeal abscess
ii. Peritonsillar abscess
iii. Tracheitis
iv. Diphtheria
#69 Lecture Outline
5. Bacterial tracheitis
a. An acute bacterial infection of the subglottic area of the upper airway complicated by copious thick, pus-filled secretions
b. Typically presents with cough, stridor, and respiratory distress with a history of a preceding viral infection
c. Toddlers are at increased risk of complications due to their relatively narrow airway diameter.
d. Patients are often febrile and may prefer the sniffing position.
e. Place in a position of comfort; provide supplemental oxygen as tolerated.
f. Do not look in the mouth.
g. Do not insert an IV line.
h. Try to keep the patient as calm and comfortable as possible.
i. Have bag-mask device, ET tube one to two sizes smaller than anticipated.
j. Alert the receiving facility of the potential need to intubate a difficult airway.
#70 Lecture Outline
D. Lower airway emergencies
1. Asthma
a. Most common chronic illness of childhood
i. Incidence and mortality of this disease are increasing.
ii. Even infants can have reactive airway disease caused by specific triggers.
b. Three main components:
i. Bronchospasm
ii. Mucus production
iii. Airway inflammation
c. As the obstruction becomes more severe, the following occur:
i. Air trapping
ii. Inadequate ventilation
iii. Worsening of hypoxemia
iv. Hypoventilation with respiratory acidosis
#71 Lecture Outline
d. Triggers for asthma attacks:
i. Upper respiratory infections
ii. Environmental allergies
iii. Exposure to cold
iv. Changes in the weather
v. Secondhand smoke
e. Clinical signs:
i. Frequent cough
ii. Wheezing
iii. General signs of respiratory distress
f. Primary survey will vary based on the degree of obstruction and the presence or absence of respiratory fatigue.
g. Mild to moderate respiratory distress
i. Child will be awake and alert, sometimes preferring a seated posture.
ii. Although increased work of breathing may be evident by retractions and nasal flaring, circulation will seem normal.
h. Signs of severe respiratory distress and impending respiratory failure include:
i. Decreasing alertness
ii. Tripod position
iii. Deep retractions
iv. Cyanosis
i. Primary survey will reveal:
i. Inability to speak in full sentences
ii. Increased respiratory rate
iii. Prolonged expiration phase
iv. Wheezes noted on auscultation
j. Expiratory wheezing alone may be heard with mild to moderate asthma attacks.
k. Wheezing may be heard on inspiration and expiration with moderate to severe disease.
l. Decreased air movement and the absence of wheezes suggest severe lower airway obstruction and respiratory fatigue.
i. Immediate treatment is needed to prevent respiratory arrest.
m. SAMPLE history should reveal the frequency and severity of previous asthma attacks, as reflected by ED visits and hospitalizations.
n. Factors that increase the risk of asthma-related death:
i. A history of near-fatal asthma requiring intubation and mechanical ventilation
ii. Hospitalization or an emergency care visit for asthma in the past year
iii. Currently using or having recently stopped using oral corticosteroids
iv. Not currently using inhaled corticosteroids
v. Overuse of short-acting beta-agonists
vi. Poor adherence with asthma medications
vii. Food allergy in a patient with asthma
o. Medication history should identify any preventive treatment and any rescue medications administered by the caregiver before your arrival.
i. Inhaled steroids are the most common controller medications.
ii. Inhaled albuterol is the most common beta-2 agonist drug used as a rescue medication.
#72 Lecture Outline
p. Initial management:
i. Position of comfort; supplemental oxygen
ii. Gold standard treatment: Bronchodilators
q. Bronchodilators may be delivered by nebulizer or MDI with a spacer-mask device.
i. Unit doses of 2.5 mg of albuterol premixed with 3 mL of normal saline
(a) Often used for nebulization
(b) Acceptable starting dose for most young children
ii. For a larger child or a child of any age who is in severe distress, consider 5 mg of albuterol as the initial dose.
r. Moderate to severe respiratory distress: Give treatments as often as needed during transport, including back-to-back nebulizer treatments.
s. Moderate to severe respiratory distress may also benefit from inhaled ipratropium (Atrovent).
t. Studies have shown that the combination of albuterol and ipratropium is more effective than albuterol given alone.
u. The dose of ipratropium given is based on the patient’s weight:
i. Less than 10 kg (22 pounds): A 0.25-mg unit dose nebulized or one puff by MDI
ii. More than 10 kg (22 pounds): A 0.5-mg unit dose nebulized or two puffs by MDI
v. IM dexamethasone at 0.6 mg/kg (maximum dose of 16 mg) given early (particularly within the first hour of presentation) can:
i. Shorten acute exacerbations of asthma
ii. Prevent or shorten hospitalizations
w. If a child is in severe respiratory distress, has an altered mental status, or has markedly diminished air movement on auscultation, a dose of epinephrine may be required.
i. Dose is 0.01 mg/kg of 1 mg/mL (1:1,000) epinephrine injected IM.
ii. Single doses should not exceed 0.3 mg.
iii. Initiate bronchodilator therapy immediately after administering the epinephrine.
x. Assisted ventilation is problematic for patients with an asthma exacerbation.
i. High inspiratory pressures force air into the lungs, but exhalation is compromised by bronchospasm, mucus production, and inflammation.
ii. Leads to air trapping and a high risk of pneumothorax and cardiovascular collapse
iii. Should be undertaken only if the patient has respiratory failure and has failed to respond to IM epinephrine and high-dose bronchodilators
iv. If performed, use slow rates to allow time for adequate exhalation: Goal is adequate oxygenation.
#73 Lecture Outline
4. Respiratory syncytial virus (RSV) infection
a. Leading cause of lower respiratory tract infections in infants, older people, and immunocompromised people
b. Common and contagious virus that causes bronchiolitis and pneumonia in children.
c. In the community setting, outbreaks generally occur in late fall, winter, and early spring.
d. Transmitted via:
i. Direct contact with large droplets, which do not travel more than 3 feet (1 m)
ii. Indirect contact with contaminated hands or contaminated items.
e. Research has shown that RSV on hands will die within 1 hour; however, it can survive on other surfaces for as long as 30 hours.
f. Incubation period ranges from 2 to 8 days.
g. Most EDs can identify RSV with a nasal swab.
#74 Lecture Outline
h. Signs and symptoms:
i. Sneezing
ii. Runny nose
iii. Nasal congestion
iv. Cough
v. Fever
i. The disease progresses to the lower respiratory tract, leading to:
i. Pneumonia
ii. Bronchiolitis
iii. Tracheobronchitis
j. Hypoxemia and apnea are often seen in infants and are usually the leading cause for a child’s hospitalization.
#75 Lecture Outline
k. Prevention of RSV transmission relies on proper use of personal protective equipment.
i. Gloves and good handwashing.
ii. Use of alcohol-based foams or gels is acceptable.
iii. Post-transport cleaning of the vehicle is important, but special cleaning solutions are not required.
l. Postexposure treatment consists of supportive care.
i. If you have been exposed, your designated infection control officer will monitor your health status.
ii. Health care providers in whom RSV infection develops should be placed on work restrictions.
#76 Lecture Outline
5. Bronchiolitis
a. Inflammation or swelling of the small airways (bronchioles) in the lower respiratory tract due to viral infection
b. Most common source is RSV; also a newer virus, metapneumovirus, and some other respiratory viruses.
c. Transmission generally occurs by inhaling droplets of infected mucus or respiratory secretions.
d. Highest frequency in winter
e. Primarily affects infants and children younger than 2 years
f. Highly contagious
g. Severity ranges from mild to moderate respiratory distress with hypoxia and respiratory failure.
h. Younger infants are at particularly high risk for episodes of apnea associated with RSV infection, which may not be associated with severe respiratory distress.
i. Can be difficult to distinguish from asthma.
i. One clue is age: Asthma is rare in children younger than 1 year.
ii. An infant with a first-time wheezing episode in late fall or winter likely has bronchiolitis.
j. Characteristic findings:
i. Mild to moderate retractions
ii. Tachypnea
iii. Diffuse wheezing
iv. Diffuse crackles
v. Mild hypoxia
#77 Lecture Outline
k. Child is in danger of respiratory failure:
i. Sleepy
ii. Severe retractions
iii. Diminished breath sounds
iv. Moderate to severe hypoxia (oxygen saturation less than 90%)
l. Greatest risk for respiratory failure and arrest:
i. First months of life
ii. History of prematurity
iii. Underlying lung disease
iv. Congenital heart disease
v. Immunodeficiency
#78 Lecture Outline
m. Management is supportive.
i. Position of comfort
ii. Supplemental oxygen
iii. Suction thick nasal and oral secretions.
n. Because the bronchioles are usually too deep in the airway to be surrounded by any smooth muscle, aerosol bronchodilators rarely help.
i. One definition of bronchiolitis is wheezing that is unresponsive to bronchodilators.
o. Although bronchodilator therapy has not proved effective in the majority of cases, nebulized racemic epinephrine (0.5 mL of a 2.25% solution for inhalation) should be administered to children in severe respiratory distress if suctioning and oxygen administration fail to result in clinical improvement.
p. CPAP should be administered, if available, for severe respiratory distress.
q. Assist breathing with bag-mask ventilation, supraglottic devices, or ET intubation if needed.
#79 Lecture Outline
6. Pneumonia
a. Infection of the lower airway and the lung
b. Commonly seen in infants, toddlers, and preschoolers.
c. Often caused by a virus in infants and toddlers
d. Incidence of bacterial pneumonia increases as children get older.
e. Recent history of a cough or cold, or a lower airway infection.
f. Maintain a high index of suspicion when called for children with any drop in oxygen saturation, particularly when accompanied by a fever or abnormal breath sounds.
g. Often present with unusually rapid breathing, or with grunting or wheezing sounds.
h. Additional signs and symptoms:
i. Nasal flaring
ii. Tachypnea
iii. Crackles
iv. Chest pain
v. Hypothermia or fever
i. May have unilateral diminished breath sounds.
j. Infants may not tolerate pneumonia as well as older children or adults.
k. Primary treatment is supportive.
i. Monitor airway and breathing status.
ii. Administer supplemental oxygen if required.
l. Take standard precautions.
i. Consider placing a mask on the child if tolerated.
m. Vascular access is generally not indicated.
#80 Lecture Outline
7. Pertussis
a. Also known as whooping cough
b. Highly contagious, potentially deadly disease
c. Caused by a bacterium that is spread through respiratory droplets
d. Less common in the United States due to vaccinations, though immunization rates have fallen
e. Signs and symptoms are similar to a common cold: coughing, sneezing, and a runny nose.
f. Coughing becomes more severe and is characterized by the distinctive whoop sound heard during the inspiratory phase.
i. The cough can be so severe that it can cause postcough vomiting, conjunctival hemorrhage, and cyanotic hypoxia.
ii. In very young infants, pertussis can also present with apnea.
g. Keep the airway patent, and transport to the ED.
h. Follow standard precautions, including wearing a mask and eye protection.
#81 Lecture Outline
E. Other respiratory conditions
1. Cystic fibrosis (CF)
a. Genetic disease that primarily affects the respiratory and digestive systems
b. Most common life-shortening hereditary disease among people of European descent
c. Chronic production of copious amounts of thick mucus in the respiratory and digestive tracts
i. Susceptible to recurrent respiratory infections that require hospitalization
ii. Requires a strict regimen of aerosol treatments, mucus management, and pulmonary exercise
d. May present with tachypnea, chest pain, and crackles.
e. Provide supplemental oxygen as needed.
f. Vascular access is generally not needed.
#82 Lecture Outline
2. Bronchopulmonary dysplasia
a. Spectrum of lung conditions found in full-term and preterm infants who required long periods of high-concentration oxygen and ventilator support
i. Ranges from mild reactive airways to debilitating chronic lung disease
b. Some infants are left with severely damaged lungs, occasionally requiring long-term ventilator support.
c. Children may use home ventilators, have tracheostomies, or have fragile lungs and many pulmonary complications.
d. High risk for recurrent pulmonary infections including pneumonias, bronchiolitis, and tracheitis.
e. Many patients will be on home oxygen.
i. Important to ask caregivers about baseline oxygen requirements, tracheostomy secretions, and ventilator settings.
ii. Note any acute changes that have occurred with illness.
#83 Lecture Outline
f. Remember the ABCs
g. Consider bag-mask ventilation and positive airway pressure.
h. CPAP or BiPAP may be beneficial.
i. May require intubation for severe distress or respiratory failure.
i. May need a smaller tube than you would typically pick based on age
j. Children with desaturations require oxygen therapy.
k. If bronchospasm is present, bronchodilators such as albuterol may be tried.
i. Improvement may not be seen because the mechanism could be related to the underlying lung disease.
l. Ipratropium may be beneficial and should be considered.
m. Oral and IM steroids can be considered acutely.
#84 Lecture Outline
F. General assessment and management of respiratory emergencies
1. Infants and young children with severe tachypnea and retractions, in association with hypoxia, bradycardia, or altered mental status, are in respiratory failure and need immediate intervention to prevent respiratory arrest.
2. A respiratory rate too slow for age in a child with a history of respiratory distress should also raise concerns for respiratory fatigue and failure.
3. Airway management
a. Check for obstruction.
b. Position airway using head tilt–chin lift or jaw-thrust maneuver.
c. In a child younger than 2 years, place a thin layer of padding under the shoulders or upper torso to align the airway.
d. Airway adjunct may be helpful if patient is unresponsive and cannot maintain a patent airway.
e. Nasal or oral airway will help to maintain an open airway, improve bag-mask ventilation, and may avert the need for an advanced airway.
#85 Lecture Outline
4. Oropharyngeal airway
a. Keeps the tongue from blocking the airway
b. Makes suctioning easier
c. Use with patients who are unresponsive and cannot maintain their own airway.
d. Do not use with patients who are conscious or have a gag reflex.
e. Do not use with children who have ingested a caustic or petroleum-based product.
f. To properly insert an oropharyngeal airway, refer to Skill Drill 43-1.
g. Avoid injuring the hard palate as you insert the airway.
i. Can cause bleeding that may aggravate airway problems and cause vomiting.
h. If the oropharyngeal airway is too small, the tongue may be pushed back into the pharynx, obstructing the airway.
i. If it is too large, it may obstruct the larynx.
#86 Lecture Outline
5. Nasopharyngeal airway
a. Usually well tolerated.
b. Used for conscious patients and patients with altered levels of consciousness.
c. Typically used in association with respiratory failure.
d. Also a good choice for maintaining an airway in patients who are experiencing a seizure or who are in a postictal state.
e. Rarely used for children younger than 1 year because of the small diameter of their nares.
f. To properly insert a nasopharyngeal airway, refer to Skill Drill 43-2.
#87 Lecture Outline
g. Several problems are possible:
i. Diameter that is too small may become obstructed by mucus, blood, vomitus, or soft tissues of the pharynx.
ii. If airway is too long, it may stimulate the vagus nerve and slow the pulse rate; it may also enter the esophagus, causing gastric distention.
iii. Inserting the airway in responsive patients may cause spasm of the larynx and result in vomiting.
h. Do not use with facial trauma because the airway may tear soft tissues and cause bleeding into the airway.
i. Do not use with moderate to severe head trauma because it could increase intracranial pressure (ICP).
#88 Lecture Outline
6. Oxygenation
a. All patients with respiratory emergencies should receive supplemental oxygen.
b. Two most common delivery methods with pediatric patients:
i. Blow-by technique
ii. Nonrebreathing mask
#89 Lecture Outline
c. Blow-by technique:
i. Best used when only a small amount of supplemental oxygen is needed or when the patient cannot tolerate wearing the mask needed for higher oxygen delivery.
ii. Oxygen tubing, a mask, a cup, or a similar device can be used for delivery.
iii. Child or caregiver can hold the device near the patient’s face.
iv. Do not use a Styrofoam cup because it may blow fluorocarbons into the child’s airway.
v. Goal is to increase oxygen concentration immediately around the mouth and nose.
#90 Lecture Outline
d. For children in significant respiratory distress or respiratory failure or for older children, a nonrebreathing mask is the preferred delivery method.
i. Use high flow rates (10 to 15 L/min) to achieve the maximum oxygen concentration.
ii. Can deliver up to 95% oxygen
#91 Lecture Outline
7. Bag-mask ventilation
a. Use if respiratory effort is not improved with airway positioning or an airway adjunct.
i. Definitive airway management for many patients
iii. May avert the need for ET intubation
b. May need to try a variety of mask sizes
c. Avoid excessive tidal volumes and rate to minimize gastric distention, vomiting, and aspiration.
d. Deliver breaths at a rate of 12 to 20 breaths/min for infants and children
i. One breath every 3 to 5 seconds
ii. Squeeze bag only until you see chest rise.
e Do not overdistend the chest.
#92 Lecture Outline
f. Follow these steps with an infant or child:
i. Ensure that you have the appropriate equipment in the right size.
(a) Mask should extend from the bridge of the nose to the cleft of the chin, avoiding compression of the eyes.
(b) Mask is transparent.
(c) Mask volume should be small to decrease dead space and avoid rebreathing; however, the bag should contain at least 450 mL of air.
(d) Use an infant bag rather than a neonatal bag for children older than 1 year.
(e) Older children and adolescents may need an adult-size bag.
(f) Make sure that there is no pop-off valve on the bag; if there is one, make sure that you can hold it shut as necessary to achieve adequate chest rise.
ii. Maintain a good seal with the mask on the face.
(a) Consider airway adjuncts in tandem with bag-mask ventilation.
iii. Ventilate at the appropriate rate and volume using a slow, gentle squeeze until the chest visibly rises.
(a) One second per breath
(b) Do not hyperventilate.
#93 Lecture Outline
g. Errors in technique can result in gastric distention and decreased preload
i. Too much volume with each breath
ii. Squeezing the bag too forcefully
iii. Ventilating at too fast a rate
h. An inadequate mask-to-face seal or improper head position can lead to inadequately delivered tidal volume and hypoxia.
i. To properly perform one-person bag-mask ventilation for an infant or child, refer to Skill Drill 43-3.
j. Two-person bag-mask ventilation
i. Usually more effective at maintaining a tight seal, delivering adequate tidal volume
#94 Lecture Outline
8. Supraglottic airways
a. Used to provide:
i. Positive pressure ventilation to apneic patients
ii. Maintain a patent airway in unresponsive patients who are breathing spontaneously but who require advanced airway management.
#95 Lecture Outline
9. Endotracheal intubation
a. Consider only if adequate oxygenation and ventilation cannot be achieved with good bag-mask technique or if transport times are long.
#96 Lecture Outline
b. Advantages: Definitive airway and decreased risk of aspiration
c. Significant failure and complication rates in the prehospital setting.
d. Potential complications include:
i. Damage to teeth and oral structures
ii. Aspiration of gastric contents
iii. Bradycardia due to a vagal response
iv. Bradycardia due to hypoxemia from prolonged attempts
v. Increased ICP
vi. Incorrect placement
#97 Lecture Outline
e. Indications:
i. Cardiopulmonary arrest
ii. Respiratory failure or arrest
iii. Traumatic brain injury
iv. Unresponsiveness
v. Inability to maintain a patent airway
vi. Need for prolonged ventilation
vii. Need for ET administration of resuscitative medications (if no IV or IO access available)
f. Remember the differences between adult and pediatric airways.
#98 Lecture Outline
g. Equipment for endotracheal intubation
i. Pediatric-specific equipment is mandatory:
(a) Range of laryngoscope blades, sizes 0 to 3
(b) ET tubes, sizes 2.5 (for field deliveries of premature infants) to 6.0
ii. Tube size selection is based on the child’s age.
iii. Any size of laryngoscope handle can be used.
iv. Straight blades make it easy to lift the floppy epiglottis to provide a direct view of the vocal cords.
#99 Lecture Outline
v. Appropriately sized blade extends from the patient’s mouth to the tragus of the ear.
vi. Length-based resuscitation tape measure or following these general guidelines:
(a) Premature newborn: Size 0 straight blade
(b) Full-term newborn to 1 year: Size 1 straight blade
(c) 2 years to adolescent: Size 2 straight blade
(d) Adolescent or older: Size 3 straight or curved blade
vii. Length-based resuscitation tapes are more accurate than age-based formula estimates for determining the correct ET tube size in patients up to about 77 pounds (35 kg).
#100 Lecture Outline
viii. Uncuffed ET tube:
(a) Use a 3.5-mm tube for infants up to 1 year of age.
(b) Use a 4-mm tube for children between 1 and 2 years of age.
(c) For children older than 2 years, use this formula:
(1) 4 + (Age in years ÷ 4) = Uncuffed tube size (in mm)
#101 Lecture Outline
ix. Cuffed ET tube:
(a) Use a 3-mm tube for infants and a 3.5-mm tube for children between 1 and 2 years of age.
(b) For children older than 2 years, use this formula:
(1) 3.5 + (Age in years ÷ 4) = Cuffed tube size (in mm)
x. Always have a tube that is one size smaller and one that is one size larger than expected available for situations in which there is variability in upper airway diameter.
xi. For patients who are younger than 8 to 10 years, you may choose to use uncuffed ET tubes, although a noninflated cuffed tube is acceptable.
(a) Cuff at the cricoid ring may be unnecessary to obtain a seal in young children.
(b) Possibility of ischemia and damage to the mucosa of the trachea at this location when cuffs are inflated at high pressures
#102 Lecture Outline
xii. The appropriate depth for insertion is 2 to 3 cm beyond the vocal cords.
(a) Record this depth as the mark at the corner of the child’s mouth.
xiii. Uncuffed tubes often have a black glottic marker at the tube’s distal end to use as a guide.
(a) When you see this line go through the vocal cord, stop.
xiv. Cuffed tubes: When the cuff is just below the vocal cords, stop.
xv. Insert tube to a depth that is equal to three times the inside diameter of the tube.
xvi. Pediatric stylets will fit into tubes sized 3 to 6 mm; adult stylets are used for tubes 6 mm or larger.
(a) Use of a stylet is based on personal preference.
(b) If you use a stylet stop at least 1 cm from the end of the tube.
(c) A stylet that protrudes beyond the end of the tube can damage the oral mucosa and vocal cords.
xvii. With stylet in place, bend ET tube into a gentle upward curve.
(a) In some cases, bending the tube into the shape of a hockey stick is beneficial.
#103 Lecture Outline
h. Preparing for and performing endotracheal intubation
i. Preoxygenate (do not hyperventilate) with a bag-mask device and 100% supplemental oxygen for at least 2 to 3 minutes before you attempt intubation.
ii. Ensure proper head position.
(a) Neutral position with suspected spinal trauma
(b) Sniffing position without trauma
iii. Insert an airway adjunct if needed.
iv. Apply a cardiac monitor if one is available.
v. Use a pulse oximeter before, during, and after the intubation attempt.
#104 Lecture Outline
vi. Have suction handy.
vii. To properly perform pediatric endotracheal intubation, refer to Skill Drill 43-4.
viii. If an intubated child deteriorates, use the DOPE mnemonic to identify the potential problem and institute an appropriate intervention.
(a) Displacement
(b) Obstruction
(c) Pneumothorax
(d) Equipment failure
#105 Lecture Outline
l. Complications of endotracheal intubation:
i. Unrecognized esophageal intubation
ii. Induction of emesis and possible aspiration
iii. Hypoxia resulting from prolonged intubation attempts
(a) Limit pediatric intubation attempts to 20 seconds.
iv. Damage to teeth, soft tissues, and intraoral structures
#106 Lecture Outline
10. Orogastric and nasogastric tube insertion
a. During positive pressure ventilation, it is common to inflate the stomach and lungs with air and liquid.
b. Gastric distention slows downward movement of the diaphragm and decreases tidal volume.
i. Makes ventilation more difficult
ii. Necessitates higher inspiratory pressures
iii. Increases risk of patient vomiting and aspirating stomach contents into the lungs
c. Invasive gastric decompression: Placement of a NG tube or OG tube to decompress the stomach by removing the contents with suction, making assisting ventilation easier
i. Contraindicated in unresponsive children with a poor or absent gag reflex and an unsecured airway
#107 Lecture Outline
d. Preparation of equipment
i. You will need the following:
(a) Appropriately sized NG or OG tube
(b) 30- to 60-mL syringe with a funnel-tipped adapter for manual removal of stomach contents through the tube
(c) Mechanical suction
(d) Adhesive tape
(e) Water-soluble lubricant
#108 Lecture Outline
ii. To prepare patient and equipment, take the following steps:
(a) Select proper tube size. Use a pediatric length-based resuscitation tape measure to determine the proper size, or use a tube size twice the uncuffed ET tube size that the child would need. For example, a child who needs a 5-mm uncuffed ET tube requires a 10-F OG or NG tube.
(b) Measure the tube on the patient. Tube length should be the same as the distance from the lips or tip of the nose (depending on whether the OG or NG route is used) to the earlobe plus the distance from the earlobe to the xiphoid process.
(c) Mark this length on the tube with a piece of tape. When the tip of the tube is in the stomach, the tape should be at the lips or nostril.
#109 Lecture Outline
(d) Place patient in a supine position.
(e) Assess the gag reflex. If patient is unresponsive and has a poor or absent gag reflex, perform ET intubation before gastric tube placement.
(f) In a trauma patient, maintain in-line stabilization of the cervical spine if a neck injury is possible. Choose the OG route of insertion if the patient has a severe head or midfacial injury.
(g) Lubricate the end of the tube.
#110 Lecture Outline
e. OG tube insertion
i. Steps:
(a) Insert the tube over the tongue, using a tongue blade if necessary to facilitate insertion.
(b) Advance the tube into the hypopharynx, then insert it rapidly into the stomach.
(c) If the child begins coughing or choking or has a change in voice, immediately remove the tube; it may be in the trachea.
#111 Lecture Outline
f. NG tube insertion
i. Steps:
(a) Insert the tube gently through the naris, directing the tube straight back along the nasal floor. Do not angle the tube superiorly. If the tube does not pass easily, try the opposite naris or a smaller tube. Never force the tube.
(b) Advance the tube into the stomach.
(c) If unsuccessful, use the OG approach.
#112 Lecture Outline
g. Assessing placement of OG and NG tubes
i. Steps:
(a) Aspirate stomach contents. Use a syringe with an appropriate adapter to quickly instill 10 to 20 mL of air through the tube while auscultating over the left upper quadrant. If you hear a rush of air (or gurgling) over the stomach, the placement is correct.
(b) If correct placement cannot be confirmed, remove the tube.
(c) Secure the tube to the bridge of the nose or to the cheek, using adhesive tape.
(d) Aspirate air from the stomach, using a 30- to 60-mL catheter-tipped syringe, or connect the tube to mechanical suction at a low, continuous suction of 20 to 40 mm Hg or to the intermittent setting.
#113 Lecture Outline
h. Complications:
i. Placement of tube into the trachea, resulting in hypoxia
ii. Vomiting and aspiration of stomach contents
iii. Airway bleeding or obstruction
iv. Passage of tube into the cranium
#114 Lecture Outline
G. Cardiopulmonary arrest
1. Most are the result of respiratory failure and shock.
2. About 25% result from sudden dysrhythmias that require:
a. Delivery of high-quality CPR
b. Recognition of a shockable rhythm
c. Prompt defibrillation
#115 Lecture Outline
VII. Pathophysiology, Assessment, and Management of Shock
A. Shock is inadequate delivery of oxygen and nutrients to tissues to meet metabolic demand.
1. You may encounter three types in both children and adults: hypovolemic, distributive, and cardiogenic.
2. Determine the cause of shock and quickly determine whether the child is in a compensated or decompensated state.
#116 Lecture Outline
a. Compensated shock
i. Critical abnormalities of perfusion, but the body is able to maintain adequate perfusion to vital organs by shunting blood from the periphery, increasing the pulse rate, and increasing the vascular tone.
ii. Normal appearance, tachycardia, and signs of decreased peripheral perfusion, such as cool extremities with prolonged capillary refill
iii. Intervention is needed to prevent child from decompensating.
#117 Lecture Outline
b. Decompensated shock
i. State of inadequate perfusion; mechanisms to improve perfusion are no longer sufficient to maintain a normal blood pressure.
ii. Includes hypotension
(a) Relative to the age of the child
iii. Child will be profoundly tachycardic and show signs of poor peripheral perfusion.
iv. May have an altered appearance.
v. Hypotension is a late and ominous sign.
vi. Initial management: Position of comfort, supplemental oxygen
vii. After primary survey, make a transport decision based on the severity of the problem.
viii. Start resuscitation on scene for any child who shows signs of decompensated shock.
ix. Rapid transport.
#118 Lecture Outline
B. Hypovolemic shock
1. Most common cause of shock in infants and young children, with loss of volume occurring due to illness or trauma.
a. Because of their small blood volume (70 mL/kg body weight), a combination of excessive fluid losses and poor intake can result in shock relatively quickly.
b. The same vulnerability exists with hemorrhage from trauma.
2. Patient will have a normal mental status or may appear slightly anxious.
3. Early indicators of shock:
a. Tachycardia
b. Pale or mottled skin
c. Narrowing of the pulse pressure
d. Cool extremities
4. Signs of shock progression:
a. Patient becomes restless and less alert
b. Increased respiratory rate
c. Delayed capillary refill
d. Cool skin
e. Hypotension
5. Signs of dehydration:
a. Sunken eyes
b. Dry mucous membranes
c. Poor skin turgor
#119 Lecture Outline
6. Allow the child to remain in a position of comfort, administer supplemental oxygen, and keep the child warm.
7. Apply direct pressure to stop any external bleeding.
8. Volume replacement is the mainstay of treatment for hypovolemic shock.
#120 Lecture Outline
9. With compensated shock, you can attempt to establish IV or IO access en route.
10. Gather all equipment before beginning this step:
a. Catheters—preferably an over-the-needle catheter—are available in pediatric sizes of 20, 22, and 24 gauge.
i. A butterfly needle is a temporary alternative if an over-the-needle catheter is unavailable.
11. IV access sites in children.
a. Most common: Dorsum of the hand and antecubital fossa
b. Veins in the foot may also be used.
c. Scalp veins, external jugular veins less common
#121 Lecture Outline
12. Establish IV access.
13. Once IV access is established, fluid resuscitation should begin with isotonic fluids only, such as normal saline or lactated Ringer solution.
a. Begin with 20 mL/kg, then reassess the patient’s status.
b. Warm IV fluids (when possible) can counteract the effects of systemic hypothermia from environmental exposure, blood loss, or open wounds.
c. Multiple fluid boluses may be necessary during transport.
14. Address volume resuscitation separately from hypoglycemia.
a. With shock due to medical illness, perform a bedside glucose check.
b. Treat with dextrose-containing fluid only for a documented low blood glucose level.
c. Hypoglycemia is unlikely in shock due to acute injury.
15. If a child is in decompensated shock, begin initial fluid resuscitation on scene.
a. Evaluate sites for IV access.
b. If this is unsuccessful, begin IO infusion.
c. An IO infusion is contraindicated if a secure IV line is available or if a fracture (or possible fracture) exists in the same bone in which you plan to insert the IO needle.
d. Anything that can be administered through an IV line can be administered through an IO line.
#122 Lecture Outline
e. IO needles are usually double needles, consisting of a solid-bore needle inside a sharpened hollow needle.
i. Double needle is pushed into the bone (usually the proximal tibia) with a screwing, twisting action away from the joint to avoid disruption of the growth plate.
ii. Once the needle pops through the bone, the solid needle is removed, leaving the hollow steel needle in place.
iii. Standard IV tubing is attached to this catheter.
f. IO lines require full and careful immobilization because they rest at a 90° angle to the bone and are easily dislodged.
i. Stabilize the IO needle in the same manner that you would any impaled object.
g. Complications associated with IO infusion:
i. Compartment syndrome
ii. Failed infusion
iii. Growth plate injury
iv. Osteomyelitis
v. Skin infection
vi. Bony fracture
h. To properly establish a pediatric IO infusion, refer to Skill Drill 43-5.
i. Administer 20 mL/kg boluses of isotonic fluid via IO infusion to treat hypovolemia, reassessing after each bolus and repeating as needed.
i. As much as 60 mL/kg may be needed during transport to improve blood pressure, pulse rate, mental status, and peripheral perfusion.
j. Rapidly transport the patient.
#123 Lecture Outline
C. Distributive shock
1. Decreased vascular tone develops.
a. Results in vasodilation and third spacing of fluids due to increased vascular permeability
i. Leakage of plasma out of blood vessels, into surrounding tissues
ii. Results in a drop in effective blood volume and functional hypovolemia
2. May be due to:
a. Sepsis
b. Anaphylaxis
c. Adrenal insufficiency
d. Spinal cord injury
3. Sepsis accounts for most pediatric cases.
4. Early in distributive shock, child may have warm, flushed skin and bounding pulses.
a. Result of peripheral vasodilation
5. Signs, symptoms of late distributive shock are similar to those with hypovolemic shock
6. Fever is a key finding in septic shock.
7. Urticarial rash and wheezing may be noted in anaphylaxis.
8. Neurologic deficits are apparent in shock due to spinal cord injury.
9. First-line treatment is volume resuscitation.
a. Child is in a state of relative hypovolemia.
10. In a child with apparent sepsis who remains persistently hypotensive despite 60 mL/kg of isotonic fluid, vasopressor support may be considered.
11. If anaphylaxis is present, provide IM epinephrine.
12. The decision about timing of IV access and transport for patients in distributive shock considers the same factors as for patients in hypovolemic shock.
13. Adrenal insufficiency can lead to distributive shock.
14. Patients may have:
a. A preexisting condition (eg, Addison disease)
b. Adrenal suppression from chronic steroid use (eg, to treat autoimmune disease or a malignancy)
15. These patients will benefit from fluids but will need stress-dose steroids to maintain circulation.
a. Medical direction may order that 2 mg/kg IV (maximum of 125 mg ) be given for this purpose.
#124 Lecture Outline
D. Cardiogenic shock
1. Result of pump failure
a. Normal intravascular volume
b. Poor myocardial function
2. Uncommon in the pediatric population
3. May be present in children with the following:
a. Underlying congenital heart disease
b. Myocarditis
c. Cardiomyopathy
d. Rhythm disturbances
4. Important to recognize cardiogenic shock
a. Treatment is different from that for hypovolemic or distributive shock.
#125 Lecture Outline
5. Signs and symptoms:
a. Listless or lethargic appearance
b. Increased work of breathing
i. Due to heart failure (HF) and pulmonary edema
c. Impaired circulation
d. Pale, mottled, cyanotic, or clammy skin
e. Abnormal pulse rate or rhythm or findings of a murmur or gallop
f. Enlarged liver
g. Sweating with feeding
h. History of congenital heart disease
#126 Lecture Outline
6. Initial management includes:
a. Position of comfort
b. Supplemental oxygen
c. Transport
7. Transport destination is critical.
a. Facility needs to be capable of pediatric critical care.
8. Supplemental oxygen
a. May not increase oxygenation saturation in children with particular types of congenital heart disease
b. Parents will often alert you to this fact.
9. Consider establishing IV access en route.
10. Treat dysrhythmias if they are present and contributing to shock.
#127 Lecture Outline
11. Err on the side of fluid resuscitation unless you are sure of diagnosis.
a. History of congenital heart disease
b. Afebrile
c. No history of volume loss
12. If you suspect cardiac dysfunction:
a. Administer a single isotonic fluid bolus slowly.
b. Monitor patient carefully to assess its effect.
13. The following will confirm suspicion of cardiogenic shock:
a. Increased work of breathing
b. Drop in oxygen saturation
c. Worsening perfusion after a fluid bolus
14. Inotropic agents may be needed to improve cardiac contractility and improve perfusion.
a. Rarely administered in the field
#128 Lecture Outline
VIII. Pathophysiology, Assessment, and Management of Cardiovascular Emergencies
A. Cardiovascular emergencies are relatively rare in children and are often related to respiratory insufficiency or respiratory arrest, hypovolemia, or infection.
1. Through the primary survey, you can quickly identify a cardiovascular emergency, understand the likely cause, and institute potentially life-saving treatment.
#129 Lecture Outline
B. Dysrhythmias
1. Rhythm disturbances can be classified based on whether the pulse rate is:
a. Too slow (bradydysrhythmias)
b. Too fast (tachydysrhythmias)
c. Absent (pulseless)
2. The signs and symptoms are often nonspecific.
3. If rhythm disturbance is suspected, quickly move through the primary survey, supporting the ABCs as necessary.
4. An ECG will help identify the underlying rhythm and determine management.
5. Address reversible causes of dysrhythmias such as hypoxemia.
6. The decision to stay on scene to obtain additional history and perform a secondary assessment will be dictated by overall physiologic status.
#130 Lecture Outline
7. Bradydysrhythmias
b. Most often occurs secondary to hypoxia in children.
c. First-line treatment: Airway management, supplemental oxygen, assisted ventilation as needed
d. Less common causes of bradycardia include hypothermia, congenital or acquired heart block, and toxic ingestion of beta-blockers, calcium-channel blockers, or digoxin.
e. Elevated ICP can also cause bradycardia and should be considered in children with the following:
i. Ventricular shunts
ii. History of head injury
iii. Suspected child abuse without a consistent injury history
#131 Lecture Outline
f. Attempt to identify and treat the underlying cause of the bradycardia.
g. Cardiovascular compromise can occur.
h. Signs and symptoms:
i. Acute changes in mental status
ii. Dizziness
iii. Fatigue
iv. Hypotension
v. Light-headedness
vi. Respiratory distress or failure
vii. Shock
viii. Syncope
i. Initiate electronic cardiac monitoring as part of the primary survey.
j. With a sinus bradycardia, the heart rate is slower than the lower range of normal for the patient’s age.
k. Healthy, athletic adolescents may have sinus bradycardia as an incidental finding.
#132 Lecture Outline
l. Atrioventricular (AV) heart blocks can be congenital or acquired in varying degrees.
i. First-degree block is an asymptomatic, often incidental finding seen on ECG.
(a) No intervention is needed.
(b) Treatment only with signs of cardiovascular compromise.
ii. Second-degree AV block may involve a progressive prolongation of the PR interval with a subsequent drop of the QRS complex (type I) or a random drop of the QRS complex (type II).
(a) May progress to third-degree AV blocks in which the atrial and ventricular rates are totally uncoordinated.
(b) Can lead to poor perfusion and cardiovascular compromise.
(c) If the patient is asymptomatic, no further treatment is indicated in the field.
m. If the child’s heart rate is slower than 60 beats/min with signs of poor perfusion despite oxygenation and ventilation, begin chest compressions and ventilations.
#133 This figure shows the algorithm for managing pediatric bradycardia with a pulse and poor perfusion.
#134 Lecture Outline
8. Tachydysrhythmias
a. Tachycardia is present if the heart rate is faster than the upper limit of normal for the patient’s age.
b. Subdivided into two types based on the width of the QRS complex.
i. Narrow complex tachycardia: QRS complex is 0.09 second or less
ii. Wide complex tachycardia: QRS complex is greater than 0.09 second
c. Interpret the significance of a tachycardia in conjunction with your physical examination findings and the patient’s history.
d. Sinus tachycardia is common in children and may be caused by:
i. Fever
ii. Pain
iii. Anxiety
iv. Increased activity
v. Exercise
e. It may also occur as a compensatory response to hypovolemia, hypoxia, or heart failure or may be medication induced.
#135 Lecture Outline
f. Treatment is directed at the underlying cause.
i. If a child appears well but has a fever and the monitor shows a sinus tachycardia, treatment with antipyretics is all that is necessary.
ii. With a history of copious vomiting or diarrhea, fluid resuscitation is the appropriate treatment.
#136 Lecture Outline
g. Narrow complex tachycardia
i. SVT is the most frequent tachydysrhythmia requiring treatment.
ii. ECG will reveal a regular ventricular rhythm with narrow QRS complexes that begins and ends abruptly.
iii. The heart rate is often 220 beats/min or faster in an infant or 180 beats/min or faster in a child and remains constant.
(a) It does not vary with stimulation or activity.
iv. Generally, P waves cannot be discerned because of the rapid rate.
v. In a child who does not have congenital heart disease, the history obtained often does not explain the rapid heart rate.
(a) May have a history of poor feeding or “not acting right”
(b) Present with fussiness and pallor
vi. An older child may complain of dizziness, palpitations, and chest pain or pressure.
vii. Signs of shock may be present depending on the duration and rate of the tachycardia.
#137 Lecture Outline
viii. Treatment of SVT depends on the patient’s perfusion and overall stability.
ix. If the child is in stable condition, consider attempting vagal maneuvers while obtaining IV access.
(a) Record the patient’s cardiac rhythm before, during, and after a vagal maneuver.
(b) Have an older child hold his or her breath, blow into a straw with the end crimped over, or bear down as if having a bowel movement.
(c) With a younger child, place an exam glove filled with ice firmly over the midface, being careful not to obstruct the nose and mouth.
(d) Attempt these techniques only once.
x. If hemodynamically stable and the SVT persists despite the use of a vagal maneuver, consider administering adenosine.
(a) Administration will be followed by a brief run of bradycardia, VT, VF, or asystole, which will convert spontaneously to sinus rhythm.
(b) Persistence of any of these rhythms is rare.
xi. If hemodynamically unstable, synchronized cardioversion is recommended.
xii. The dose of the initial synchronized cardioversion attempt is 0.5 to 1 joule per kilogram of body weight (J/kg).
(a) If the first shock is unsuccessful, increase the energy level to 2 J/kg.
(b) Because cardioversion is a painful procedure, sedation should be provided to an awake patient before the procedure when possible (follow your protocol).
xiii. Alternative approach to treating the child in SVT with poor perfusion is to give IV adenosine if vascular access is readily available.
xiv. Do not delay synchronized cardioversion if vascular access is not already established.
#138 Lecture Outline
h. Wide complex tachycardia
i. Wide QRS complex tachycardia with a palpable pulse is likely VT.
(a) Rare but potentially life-threatening rhythm in children
(b) May reflect underlying cardiac pathology
ii. SVT may sometimes manifest as a wide complex rhythm.
(a) Distinguishing between the two can be challenging.
iii. Consider giving adenosine IV to help differentiate SVT from VT if:
(a) The child is in hemodynamically stable condition.
(b) IV access is available.
(c) The patient’s ventricular rhythm is regular and monomorphic.
iv. If the rhythm persists:
(a) Amiodarone: Medication of choice
(b) Procainamide is an acceptable alternative.
(c) Do not give amiodarone and procainamide; both prolong the QT interval.
v. If hemodynamically unstable, perform synchronized cardioversion using the same energy level as that used for SVT.
vi. If pulseless, begin CPR and follow the pulseless arrest treatment guidelines.
#139 Lecture Outline
i. Pulseless arrest
i. Survival rate from pediatric arrest in the prehospital setting is poor; few survivors have good neurologic outcomes.
ii. Most out-of-hospital pediatric cardiac arrests are not witnessed; it is estimated that only about 30% of children who experience an out-of-hospital cardiac arrest receive bystander CPR.
iii. The most important consideration is to provide high-quality CPR.
iv. Attach a monitor or defibrillator to determine the underlying cardiac rhythm.
#140 Lecture Outline
(a) Pulseless VT or VF: Defibrillation is indicated.
(1) Additional interventions: establish vascular access, administer epinephrine, and consider the administration of an antidysrhythmic, such as amiodarone.
#141 Lecture Outline
(b) Asystole or PEA: Defibrillation is not indicated.
(1) Additional treatment: establish vascular access and administer epinephrine.
(c) After administering medication, perform five cycles of CPR before rechecking rhythm.
(d) If asystole or PEA persists, continue with CPR and epinephrine.
#142 This figure shows the pediatric cardiac arrest algorithm.
#143 Lecture Outline
C. Heart failure
1. Heart can no longer meet the body’s metabolic demands at normal physiologic venous pressures.
a. Infants typically present with tachypnea, retractions, grunting, and difficulty with feeding.
b. Children often have profuse sweating, increased work of breathing during feedings.
c. Older children may have tachycardia, tachypnea, crackles on exam, or an enlarged liver.
d. Treatment focuses on correcting hypoxia, reducing preload, reducing afterload, and improving myocardial contractility.
#144 Lecture Outline
e. Treatment may include:
i. Oxygen
ii. Diuretics
iii. Inotropic medications (may be ordered by medical direction)
f. Use IV fluids judiciously because these patients are prone to worsening symptoms from fluid overload.
#145 Lecture Outline
2. Myocarditis
a. Inflammation of the heart muscle
i. Results in myocardial dysfunction
ii. Can lead to heart failure
b. Most children present with acute disease, resulting from viral infection.
#146 Lecture Outline
c. Because of the high risk of dysrhythmias and hemodynamic compromise, transport with cardiac monitors and pulse oximetry.
d. Obtain vascular access, but use IV fluids judiciously because these patients are prone to fluid overload from inefficient heart function.
e. Patients will often need inotropic support.
f. Apply oxygen during transport.
#147 Lecture Outline
3. Cardiomyopathy
a. The three main types of cardiomyopathy are dilated, hypertrophic, and restrictive.
b. Dilated cardiomyopathy is characterized by progressive dilation of the ventricles with poor contraction of the myocardial muscle fibers, resulting in low cardiac output and symptoms of heart failure.
i. Most common type of cardiomyopathy in children.
ii. It is estimated that at least 30% to 50% of cases are inherited.
iii. Other possible causes include:
(a) Infection
(b) Nutritional deficiency
(c) Exposure to toxins
iv. Common symptoms include:
(a) Fatigue
(b) Weakness
(c) Signs of heart failure
(d) Atrial and ventricular dysrhythmias
v. Because of ineffective ventricular contraction, blood pools within the heart chambers, predisposing the patient to systemic and pulmonary emboli.
#148 Lecture Outline
c. In hypertrophic cardiomyopathy, heart muscle is unusually thick; heart has to pump harder to get blood to leave.
i. Inherited disorder.
ii. Symptoms usually appear in the school-age years or during adolescence and may include chest pain, dysrhythmias, dyspnea with exertion, syncope, and sudden death.
iii. When hypertrophic cardiomyopathy occurs during infancy, signs and symptoms are those of heart failure.
iv. Crucial to thoroughly investigate reports of unexplained syncope in all patients, especially in the younger population and athletes.
#149 Lecture Outline
d. With restrictive cardiomyopathy, ventricular filling is impaired because the walls of the ventricles are stiff due to endocardial disease, myocardial disease, or both.
i. Signs and symptoms are similar to those of heart failure.
ii. Tachydysrhythmias are common.
iii. Transport the patient with cardiac monitoring and frequent reassessment of vital signs.
iv. Obtain vascular access.
v. Be prepared to treat heart failure and dysrhythmias according to local protocol or instructions from medical direction.
#150 Lecture Outline
D. General assessment and management of cardiovascular emergencies
1. Begin with PAT, primary survey, and secondary assessment.
a. An abnormal appearance may indicate inadequate brain perfusion and the need for rapid intervention.
b. Tachypnea, without retractions or abnormal airway sounds, is common in an infant or child with a primary cardiac problem.
i. Mechanism for blowing off carbon dioxide to compensate for metabolic acidosis related to poor perfusion
c. When cardiac compromise progresses to heart failure, pulmonary edema leads to increased work of breathing and a fast respiratory rate.
i. Pallor, cyanosis, or mottling may offer clues.
#151 Lecture Outline
d. Based on primary survey, determine the likely underlying cause, patient’s priority, and need for treatment or transport.
e. If patient is stable, continue assessment on site.
f. Repeat PAT, ABCs after each intervention; monitor trends.
#152 Lecture Outline
IX. Pathophysiology, Assessment, and Management of Neurologic Emergencies
A. Neurologic emergencies can be benign (eg, febrile seizure) or life threatening (eg, ventricular shunt failure).
1. Obtain a thorough past medical history, including previous seizures, shunts, cerebral palsy, or any recent trauma or ingestions.
2. Infants and children are difficult to assess neurologically; often uncooperative with your exam due to a lack of understanding or fear.
a. Assess general appearance.
b. Seek parent’s impression of subtle changes in demeanor and activity level.
#153 Lecture Outline
B. Altered mental status
1. Conditions that can result in abnormal mental status:
a. Metabolic problems
b. Infectious diseases
c. Intracranial structural abnormalities
d. Trauma
e. Hypoxia
f. Poisonings
2. A child with altered mental status displays changes in personality, behavior, or responsiveness inappropriate for age.
3. Child may appear:
a. Agitated
b. Combative
c. Sleepy
d. Withdrawn
e. Slow to respond
f. Completely unresponsive
#154 Lecture Outline
4. Use mnemonic AEIOUTIPS to remember common causes of altered level of consciousness.
5. Run through PAT and ABCDEs quickly.
6. Pay special attention to possible disability and dextrose issues.
a. Use AVPU scale to identify level of disability.
7. Check glucose level.
a. Hypoglycemia:
i. Serum glucose concentration of less than 40 mg/dL in a newborn
ii. Less than 60 mg/dL in all other infants and children
8. History taking and secondary assessment, at the scene or en route, may provide clues about the underlying cause.
#155 Lecture Outline
9. Management is the same regardless of cause.
a. Support ABCs.
b. Provide assisted ventilation or airway support as needed.
c. If child is hypoglycemic, give glucose at a targeted dose of 0.5 to 1 g/kg.
i. Goal: Maintain normal glucose level. Hyperglycemia is associated with worse neurologic outcomes in patients with cerebral ischemia.
d. If signs or symptoms suggest an opiate toxidrome, consider giving naloxone.
#156 Lecture Outline
e. Transport all patients expeditiously.
f. Assess for increased ICP; intervene as appropriate.
g. When you are intubating a pediatric patient with an altered mental status, etomidate is a common induction agent if septic shock is not suspected.
i. Dose: 0.3 mg/kg
ii. Good if patient is hypotensive; less effect on blood pressure than other choices.
iii. Other options: Midazolam 0.1 mg/kg and ketamine 2 mg/kg
iv. Ketamine is a bronchodilator; good for patients with respiratory problems.
(a) Can cause increased bronchorrhea
(b) May cause a transient drop in the blood pressure.
h. Muscle relaxants such as succinylcholine 1 to 2 mg/kg or rocuronium 1 mg/kg can be used in the pediatric population.
i. If increased ICP is suggested, adding lidocaine prior to intubation may blunt the increase in ICP associated with intubation.
i. Signs of increased ICP include Cushing triad:
(a) Bradycardia
(b) Irregular respirations
(c) Widening pulse pressure
ii. If you suspect increased ICP, elevate the head 30° if cervical spine injury is not suspected.
iii. Hyperventilation can lower ICP temporarily, but this practice must be used judiciously.
#157 Lecture Outline
C. Seizures
1. Result from abnormal electrical discharges in the brain.
a. Generalized seizures manifest as abnormal motor activity and an altered level of consciousness.
b. Some children are predisposed to seizures because of underlying brain abnormalities.
c. Others experience seizures as a result of trauma, metabolic disturbances, ingestion, or infection.
d. Febrile seizures are unique to young children and are typically benign.
#158 Lecture Outline
e. Physical manifestation of a seizure will depend on the area of the brain firing the electrical discharges and the age of the child.
i. Infants have immature brains; seizures may be subtle.
f. Repetitive movements such as lip smacking, chewing, and “bicycling” suggest seizure activity.
g. Apnea and cyanosis can also be signs of underlying seizure activity.
h. Prognosis is closely linked to the underlying cause.
i. A febrile seizure will not cause brain damage.
ii. A child who has a seizure as a complication of a head injury or meningitis may have long-term neurologic abnormalities.
#159 Lecture Outline
2. Types of seizures
a. Classification system is the same for children and adults.
i. Generalized seizures involve the entire brain.
ii. Partial seizures involve only one part of the brain.
b. The most common types of seizures are generalized tonic-clonic seizures (grand mal), which involve jerking of both arms and legs.
c. Absence seizures (petit mal) are generalized seizures that involve a brief loss of attention without abnormal body movements.
d. Partial seizures can be further subclassified.
i. Simple partial seizures: Focal motor jerking without loss of consciousness
ii. Complex partial seizures: Focal motor jerking with loss of consciousness
#160 Lecture Outline
3. Febrile seizures
a. Febrile seizures occur in about 2% to 5% of all children.
b. Child must be between age 3 months and 6 years, have a fever, and have no identifiable precipitating cause (such as head injury, ingestion, or meningitis).
c. Strongest predictor is a history of this diagnosis in a first-degree relative.
d. The child’s temperature usually increases rapidly to 101.8°F (38.8°C), and the seizure occurs during the temperature rise rather than after a prolonged elevation.
#161 Lecture Outline
e. Simple febrile seizures are brief, generalized tonic-clonic seizures (lasting less than 15 minutes) that occur in a child without underlying neurologic abnormalities.
f. Complex febrile seizures are longer (lasting more than 15 minutes), focal, or occur in a child with baseline developmental or neurologic abnormality.
i. May also be associated with serious illness.
g. Postictal phase after a febrile seizure tends to be brief, so the child will often be waking up or back to baseline by the time you arrive at the scene.
h. Depending on agency policy, a well-appearing child with a history consistent with a simple febrile seizure may be transported by EMS or by parents but always needs urgent physician evaluation.
i. Prognosis with simple febrile seizures is excellent.
i. Rare: febrile seizures that last more than 30 minutes may cause scar tissue in the temporal lobe of the brain.
ii. In some of these patients, chronic epilepsy develops, which often can be effectively treated.
#162 Lecture Outline
4. Assessment of seizures
a. Give special attention to compromised oxygenation and ventilation and signs of ongoing seizure activity.
b. Seizures place a child at risk for respiratory distress or failure because of airway obstruction, aspiration, or depressed respiratory drive.
c. Any child who is having a seizure when you arrive has likely been having seizure activity for at least 8 to 10 minutes.
i. Consider child in status epilepticus.
ii. Initiate treatment to stop the seizure.
d. Status epilepticus: Any seizure lasting more than 4 to 5 minutes or consecutive seizures without a return to consciousness between seizures
e. Refer to your local protocols for guidelines related to how long a seizure can continue before you should intervene.
#163 Lecture Outline
f. As part of history taking, ask about:
i. Prior seizures
ii. Anticonvulsant medications
iii. Recent illness, injury, or suspected ingestion
iv. Duration of seizure activity
v. Character of the seizure
#164 Lecture Outline
5. Management of seizures
a. Treatment on scene is limited to supportive care if seizure has stopped by your arrival.
b. Provide 100% supplemental oxygen to the patient, and start bag-mask ventilation as indicated for hypoventilation.
#165 Lecture Outline
c. For a child with ongoing seizure, open airway using head tilt–chin lift or jaw-thrust maneuver.
d. If airway is not maintainable with positioning, consider a nasopharyngeal airway.
e. Suction for secretions or vomitus.
i. Consider lateral decubitus position in case of ongoing vomiting.
f. Do not attempt to intubate during an active seizure.
i. Associated with serious complications
ii. Rarely successful
g. More appropriate care should include:
i. BLS airway management
ii. Stopping seizure
iii. Considering the need for ALS airway support
h. Consider NG tube if patient requires assisted ventilation.
i. Assess for IV sites.
j. Measure serum glucose; treat documented hypoglycemia.
k. Consider options for anticonvulsant administration.
l. Insertion of an IV line can be difficult.
i. Alternative routes for medication delivery may be needed.
m. Goal of medical therapy: Stop seizure, minimize anticonvulsant side effects.
n. First-line anticonvulsant treatment is a benzodiazepine:
i. Lorazepam, diazepam, or midazolam
ii. All can cause respiratory depression.
iii. Monitor oxygenation and ventilation carefully.
o. Lorazepam
i. Excellent choice for seizure management
ii. Rapid onset, lower risk of respiratory depression, relatively long half-life
p. Diazepam
i. Relatively short half-life; seizures may occur with longer transport times.
q. Midazolam
i. May be administered by IV, IM, and intranasal routes.
ii. Excellent anticonvulsant effects, but shortest duration of action of the three benzodiazepines mentioned.
iii. Be prepared to repeat dosing for recurrent seizures.
r. Any child with a history suggestive of seizures requires physician evaluation.
s. On-scene treatment is appropriate for a child in status epilepticus, but perform a detailed assessment during transport.
t. Monitor cardiorespiratory status in any postictal child; reassess frequently for recurrent seizure activity.
#166 Lecture Outline
D. Meningitis
1. Inflammation or infection of the meninges, the covering of the brain and spinal cord; most often caused by a viral or bacterial infection
2. Viral meningitis
a. More common in the summer
b. Usually caused by an enterovirus
c. Presents with associated gastrointestinal symptoms such as vomiting and diarrhea
3. Children may look and feel quite ill; viral meningitis is rarely life threatening.
4. Bacterial meningitis is potentially fatal.
a. Children can progress rapidly from mildly ill-appearing to coma and even death.
5. In the early stages, it is difficult to tell the type of infection.
a. Always proceed as if it may be bacterial meningitis.
6. Symptoms vary depending on age and the agent causing infection.
a. In general, the younger the child, the more vague the symptoms.
#167 Lecture Outline
b. A newborn with early bacterial meningitis: Only symptom may be fever.
c. Young infants will often have a fever and perhaps localizing signs such as lethargy, irritability, poor feeding, bulging fontanelle.
d. Young children rarely show typical “meningeal signs” such as nuchal rigidity until they are older.
e. Verbal children often report headaches and neck pain.
f. Altered level of consciousness and seizures are ominous symptoms at any age.
g. Projectile vomiting and photosensitivity are common findings.
h. Other signs may include Kernig sign (patient cannot extend the leg at the knee when the thigh is flexed because of hamstring stiffness) and Brudzinski sign (passive flexion of the leg on one side causes a similar movement in the opposite leg).
7. Neonates most often contract meningitis-causing bacteria during the birthing process.
a. Normal bacteria in vaginal tract can produce serious infections.
b. Escherichia coli, group B Streptococcus, Listeria monocytogenes
c. Neonatal meningitis is usually not seen beyond 3 months of age.
8. Older infants and young children are at risk for contracting viral meningitis from enteroviruses.
a. Widespread during summer and fall
9. Bacterial meningitis in this age group most often involves Streptococcus pneumoniae (pneumococcus) and Neisseria meningitidis (meningococcus).
a. Pneumococcus infection is becoming less frequent due to vaccination.
Meningitis from H. influenzae is rare because a vaccine against this pathogen was introduced in the 1990s.
11. N. meningitidis may also cause sepsis.
a. Meningococcal meningitis with sepsis is typically characterized by a rash in addition to the other meningitis symptoms.
i. Petechial (small, pinpoint red spots)
ii. Purpuric (larger purple or black spots)
#168 Lecture Outline
12. Infection control is important.
a. Meningococcus, in particular, is quite contagious.
b. Be vigilant about using standard and respiratory precautions.
c. Wear gown, gloves, and mask if meningitis is a possibility.
d. Place mask on patient.
13. Children with meningococcal sepsis and meningitis quickly become extremely sick.
14. Look for the following:
a. Fever
b. Altered mental status
c. Bulging fontanelle
d. Photophobia
e. Nuchal rigidity
f. Irritability
g. Petechiae
h. Purpura
i. Signs of shock
#169 Lecture Outline
15. Perform a glucose check.
16. Provide lifesaving interventions as needed and transport quickly.
a. Reassess frequently en route—rapid deterioration is a hallmark.
17. Patient may need oxygen, airway management, ventilation support.
18. Medical control may order IV fluids or medications for seizures or signs of shock.
#170 Lecture Outline
E. Hydrocephalus
1. Condition resulting from impaired circulation and absorption of CSF, leading to increased size of the ventricles and increased ICP.
2. CSF production rate normally matches the absorption rate, so the net volume of fluid within the brain remains constant.
3. Occurs in two main forms.
a. Normal-pressure hydrocephalus: A rare condition that occurs in older adults
i. Mechanism is unclear.
b. The other type results in increased pressure within the cranial vault.
4. The most common cause of increased ICP hydrocephalus is the slowed movement of CSF.
5. Most common reason for slowed movement:
a. Congenital malformations in the CSF aqueducts
b. Tumors
c. Trauma
d. Intracranial hemorrhage
e. Meningitis
6. Even though movement of CSF decreases, production does not; therefore, total CSF volume increases.
7. Most commonly seen:
a. Congenital brain malformations
b. As a complication of prematurity
c. Following surgery for a brain tumor
8. Signs and symptoms can develop gradually, over months, or suddenly, over days.
9. Signs and symptoms will vary depending on the cause and the age of the patient.
10. Symptoms in infants:
a. Increased head circumference due to their soft skulls
b. Lethargy
c. Irritability
d. Vomiting
e. Sun-setting eyes (a downward deviation of the eyes)
f. Tense or bulging fontanels
g. Seizures
11. Symptoms in older children and adults:
a. Headache
b. Nausea
c. Projectile vomiting
d. Blurry or double vision
e. Ataxia
f. Poor coordination
g. Memory and personality impairments
12. Cerebral shunt often used to decrease ICP.
a. Ventriculoperitoneal (VP), or less commonly, ventriculoatrial (VA) shunts are surgically inserted into the ventricles of the brain by neurosurgeons.
b. VP shunts drain excess fluid from the ventricular system of the brain into the peritoneal cavity through a tube that exits the skull at a valve.
c. VA shunts are similar, except tubing terminates in the right atrium of the heart.
d. Tubing can often be felt in the lateral portion of the neck.
e. In thin or young children, coils of tubing may also be palpable in the abdomen.
f. Draining extra CSF prevents brain herniation.
#171 Lecture Outline
13. Complications include infections, blockages, overdrainage.
14. Excessive drainage can cause the brain to collapse because of its own weight, which causes tearing and intracranial hemorrhage; insufficient drainage causes increased ICP.
15. Signs of malfunction:
a. Vomiting
b. Headache
c. Altered level of consciousness
d. Visual changes
e. With infection: Fever, redness, or tenderness over shunt
16. In patients with VP shunts, peritonitis can also accompany VP shunt infections.
#172 Lecture Outline
17. Manage increased ICP and transport immediately to a facility with pediatric neurosurgical capabilities.
18. As children grow, the length of the tube tends to shorten and must be replaced.
19. Management involves standard care.
20. Be prepared for seizures and increased ICP.
21. The patient is typically a child with multiple medical problems.
22. Do not manipulate the VP shunt; the ED physician will access the shunt if needed.
23. In patients without shunts, an emergency ventriculostomy can be done to relieve pressure within the skull.
#173 Lecture Outline
F. Traumatic brain injury (TBI)
1. Head trauma is common in childhood.
2. Small number of children who appear to be at low risk may have an intracranial injury.
a. A number of states have laws requiring medical evaluation prior to allowing children who have been concussed in a sporting event back into play.
b. Goals: Identify TBI; prevent deterioration, secondary injury.
3. Evaluate any child with head injury for signs of potential abuse.
#174 Lecture Outline
4. Epidural hematoma
a. Hemorrhage into the space between the dura and skull.
b. Uncommon in pediatric patients, but they may occur after a low-velocity fall.
c. Child abuse accounts for a significant number of cases in infants and children, whereas motor vehicle crashes account for most epidural hematomas in adolescents.
d. The low incidence in childhood may be because the middle meningeal artery is not embedded in the bone surface of the skull until about 2 years of age.
i. A fracture of the temporal bone is less likely to lacerate the artery.
e. Prompt diagnosis is critical.
f. Often presents with loss of consciousness or altered mental status.
g. Also report a severe headache accompanied by persistent vomiting or ataxia.
h. Infants may be difficult to console and have a cephalohematoma on exam.
i. Older patients may have a lucid interval with minimal symptoms after head trauma, followed several hours later by rapid clinical deterioration.
5. Subdural hematoma
a. Hemorrhage into the potential space between the dura and the arachnoid membranes.
b. Common in infants, with a peak incidence between birth and 4 months of age.
c. Occurs as a result of:
i. Birth trauma
ii. Falls
iii. Assaults
iv. Violent shaking
d. Any infant or toddler with a subdural hematoma should be suspected of having been abused until proven otherwise.
e. Suspect cervical spine injury and take cervical spine precautions.
#175 Lecture Outline
f. Hypoxia must be prevented to avoid secondary injury to brain tissue.
g. Expect vomiting, and suction as needed.
h. Administer supplemental oxygen if indicated.
i. Be prepared to assist inadequate breathing.
j. Vascular access is often indicated in patients with epidural hematomas but is less often needed for patients with subdural bleeding.
k. Consult medical direction to determine the appropriate rate at which fluids should be infused.
l. If hypotension is present, look for signs of internal bleeding.
m. Treat seizures if present.
n. Perform frequent neurologic.
i. Repeated assessments are crucial to detect signs of increasing ICP.
#176 Lecture Outline
X. Pathophysiology, Assessment, and Management of Gastrointestinal Emergencies
A. Common in the pediatric population.
1. The gut embryonically develops external to the body, then regresses into abdominal cavity.
2. Features of maldevelopment are responsible for certain pediatric gastrointestinal diseases such as Meckel diverticulum or malrotation with volvulus.
3. Organs like the liver mature over the first few months of life.
B. Biliary atresia
1. Can present in the newborn period.
a. Biliary tract is malformed such that bilirubin cannot be excreted.
b. Leads to liver disease and failure
2. Some rare genetic disorders can also present as liver failure.
a. Children may have esophageal varices, which can bleed profusely.
b. Transport children with massive GI bleeds to the nearest ED, obtain IV access, and administer fluid boluses.
#177 Lecture Outline
C. Viral gastroenteritis
1. Infection caused by a variety of viruses, or the ingestion of certain foods, such as milk or ice cream (lactose intolerance), or unknown substances.
2. In most cases, patient will have abdominal discomfort with nausea, vomiting, and diarrhea.
3. Many also have fever
4. Vomiting and diarrhea can quickly cause dehydration in children.
5. If you suspect dehydration, place an IV line and administer 20 mL/kg of an isotonic fluid.
#178 Lecture Outline
D. Appendicitis
1. Common in pediatric patients
a. If untreated can lead to peritonitis or shock.
2. Typically present with fever and pain on palpation of right lower abdominal quadrant.
a. Often describe the pain as having started in the periumbilical region and migrating to the right lower quadrant over time, usually hours.
b. Some patients have fever or vomiting.
c. Rebound tenderness may be present, but is not a finding specific to appendicitis.
3. Constipation can also cause severe abdominal pain.
a. Pain often follows a meal and is intermittent.
b. Patients have diffuse abdominal pain, but no guarding or rebound tenderness.
c. Severity can often mimic appendicitis.
4. Never assume that you can distinguish between appendicitis and constipation.
5. Transport immediately to the ED.
#179 Lecture Outline
E. Ingestion of foreign bodies
1. Common cause of GI complaints in pediatric patients
2. If a foreign body gets lodged in the esophagus, patients will often present with gagging, vomiting, and difficulty swallowing.
3. Worsening pain raises concern for perforation of a viscus.
4. Difficulty breathing or choking raises the possibility of a foreign body airway obstruction.
5. Keep child in a calm, comfortable position, often on parent’s lap, and transport immediately to the ED.
#180 Lecture Outline
F. Gastrointestinal bleeding
1. GI bleeds are rare in the pediatric population.
2. Causes are often different compared to adults.
3. An important difference: Because of the rapid transport times in the pediatric GI tract, ingested, upper, and lower bleeding may all present with hematochezia or bright red rectal bleeding.
4. In adults, upper bleeding may present as melena or dark black, tarlike stools because of the digestion of the blood in the GI tract.
5. In newborns, blood ingested during birth can present as rectal bleeding.
a. Seen in the first few days of life and is harmless.
b. Infants may have blood in their stool if there is maternal bleeding from the nipples during breastfeeding.
i. Maternal mastitis, an infection of the breast, is a common cause.
6. Children: ingested blood from epistaxis, after surgery such as tonsillectomy, or after multiple episodes of forceful vomiting.
a. Gastroenteritis and repetitive vomiting can cause small tears of the esophagus called Mallory-Weiss tears.
b. Can present as blood streaking of the emesis or blood in the stool.
i. Usually small, harmless, self-limited
7. Constipation can cause small anal fissures that present as rectal bleeding.
a. Blood from fissures presents as blood streaking on the surface of the stool.
b. Painful but self-limiting
8. Abusive trauma should always be on the differential diagnosis of rectal bleeding in the pediatric population.
#181 Lecture Outline
G. Intussusception
1. Most commonly occurs in children between ages 6 months and 6 years
2. Bowel telescopes into itself, commonly the small intestine into the large intestine at the cecum.
3. Presents with intermittent severe abdominal pain, lethargy and bloody stools (or currant jelly–like stools)
4. Surgical emergency; transport immediately.
#182 Lecture Outline
H. Meckel diverticulum
1. One of the most common congenital malformations of the small intestines
2. Presents with painless rectal bleeding or hematochezia.
3. Presents with the “rule of 2s”:
a. 2% of the population
b. Has a 2:1 male-to-female ratio
c. Located within 2 feet of the ileocecal valve
d. Commonly 2 cm in diameter and 2 inches in length
e. Contains 2 types of ectopic tissue (pancreatic and gastric)
f. Symptomatic by age 2 year
4. Can cause concern because of the large volume of blood loss
5. If you suspect Meckel diverticulum, transport the patient to the ED for further evaluation.
#183 Lecture Outline
I. Pyloric stenosis and malrotation with volvulus
1. Pyloric stenosis occurs when the pylorus becomes hypertrophied.
a. Infants present with projectile vomiting occurring after feedings.
b. Poor weight gain or weight loss, dehydration, and electrolyte abnormalities can be seen due to the amount of vomiting.
c. Surgery is curative.
#184 Lecture Outline
2. Malrotation with volvulus: Twisting of the bowel around its mesenteric attachment to the abdominal wall
a. Patients present with bilious emesis (dark green), pain, and a distended, rigid abdomen.
b. May have blood in the vomitus or stool
c. Surgical emergency; transport immediately to ED with pediatric capabilities.
#185 Lecture Outline
J. General assessment and management of gastrointestinal emergencies
1. Consider age, gender, whether child was born premature.
2. Ask about current medication use and history of similar past complaints.
#186 Lecture Outline
a. Severe abdominal pain is a common complaint with a large differential diagnosis list; however, recurrent abdominal pain that can mimic the pain of appendicitis can be seen with constipation or gastroenteritis.
b. Patients on polyethylene glycol may have pain from constipation, whereas patients on H2-blockers such as ranitidine may have gastritis or ulcer disease.
3. Look for pallor or jaundice; scleral jaundice may also be present.
a. May be signs of hepatic disease or blood breakdown or loss
4. Tachycardia is seen before hypotension.
a. Treat with an IV fluid bolus of 20 mL/kg.
5. Assess and reassess location, severity of abdominal pain at regular intervals for changes.
6. Premature infants and those with symptoms in the first weeks of life require further evaluation at a center with pediatric capabilities.
7. Give special consideration to patients with gastrostomy tubes (G-tubes); they may require continuous feeds to maintain hydration.
a. G-tubes can become dislodged by the child playing or pulling them, or when the balloon that secures the tube deflates.
b. Many parents have been trained in replacing G-tubes.
c. If a replacement tube is not available, insertion of a sterile urinary catheter or other similar catheter into the stoma is important.
d. Stomas can become narrow quickly and completely close after tube is removed.
e. Reinsertion of the original tube into the stoma can also help prevent this.
f. When replacing a G-tube or inserting another catheter, consider the age of the tract the G-tube follows.
i. Mature tracts (over 6 months old) can safely be replaced.
ii. Do not replace immature G-tube tract tubes in the field: Risk of tract perforation and insertion of the G-tube into the abdominal cavity rather than the stomach is high.
#187 Lecture Outline
g. Replacing G-tube:
i. Water-soluble lubricate tube end being inserted.
ii. Apply gentle pressure to allow the tube to slide into the stoma.
iii. If significant resistance, pain, or bleeding, abort the attempt.
iv. Tape replacement into place.
v. Transport for definitive replacement.
#188 Lecture Outline
h. Ask questions to determine how dehydrated the patient may be:
i. How many wet diapers has the child had today?
ii. Is your child tolerating liquids, and is he or she able to keep them down?
iii. How many times has your child had diarrhea and for how long?
iv. When he or she cries, are there tears present?
8. When transporting, give nothing to eat or drink until a thorough assessment can be completed.
9. Vascular access is often indicated with signs of clinical dehydration.
10. Keep patient comfortable on cardiorespiratory monitors with frequent assessment for change in hemodynamic status.
#189 Lecture Outline
XI. Pathophysiology, Assessment, and Management of Endocrine Emergencies
A. Children and young adults are much more commonly diagnosed with type 1 diabetes and are susceptible to DKA.
1. Hypoglycemia can be particularly damaging to the developing brain.
2. Children are at varying stages of cognitive development, so maintenance of blood glucose levels within the normal range can be challenging.
3. A low socioeconomic status is associated with:
a. An increased incidence of DKA
b. Poor blood glucose control
c. Lengthier hospital admissions
4. It is essential that the family be involved and supportive to increase compliance.
B. Hyperglycemia
1. Can be the presenting problem with new-onset diabetes mellitus or a complication with a known history of diabetes
2. Can result in severe dehydration and DKA if not recognized or promptly treated
3. During assessment, you will typically find:
a. Dose of insulin was missed.
b. Greater proportion of food was eaten compared with the dose of insulin.
c. Insulin pump malfunctioned.
4. Signs and symptoms depend on blood glucose level.
#190 Lecture Outline
5. During assessment, ask about the following:
a. Insulin administration
b. Functioning of insulin pump, including when the site of insertion was last changed
c. Changes in urine output
d. Changes in mental status
e. Patterns on recent glucose checks
f. Presence of urine ketones (if checked)
g. Any other symptoms, including headache, visual changes, seizures, abnormal speech, or the presence of vomiting and abdominal pain
#191 Lecture Outline
6. Management begins with 100% oxygen or assisted ventilation if needed.
7. Monitor vital signs closely.
8. Obtain IV access, and administer isotonic fluids.
9. A 10-mL/kg bolus may be administered with shock.
a. Repeat as needed to maintain adequate perfusion.
b. Up to 40 mL/kg total infusion, to maintain adequate perfusion.
10. Risk of cerebral edema with rapid IV fluid administration exists.
a. Run IV fluids slowly during transport if needed.
#192 Lecture Outline
11. If patients report worsening of a headache or mental status deteriorates during fluid administration:
a. Discontinue fluids.
b. Assess, and treat for increased ICP.
12. Closely monitor ABCs.
13. Electrolyte imbalances (particularly of potassium) may lead to ECG abnormalities and dysrhythmias.
14. Patient in DKA desperately needs insulin; however, this is not a drug that is administered in the prehospital setting.
15. If an insulin pump is working, do not discontinue its use.
16. Immediate transport to the closest appropriate facility is crucial.
#193 Lecture Outline
C. Hypoglycemia
1. May occur in patients with diabetes, often because of treatment with insulin or oral hypoglycemic agents.
2. Common in metabolically stressed children because a child is unable to store large quantities of glucose and mobilize what they can store
3. Can lead to irreversible brain damage if prolonged
4. In children, alcohol intoxication increases susceptibility to hypoglycemia and altered mental status.
5. The blood sugar level may become too low if the patient with diabetes:
a. Has taken too much insulin
b. Not eaten enough food
c. Overexercised and burned off sugar faster than normal
d. Experienced significant physical or emotional stress
#194 Lecture Outline
6. Early signs include:
a. Headache
b. Hunger
c. Nausea
d. Weakness
e. Irritability
f. Agitation
7. Later signs include:
a. Cool, pale, clammy skin
b. Tachycardia
c. Tachypnea
d. Abdominal pain
e. Dizziness
f. Sweating
g. Pallor
h. Confusion
i. Tremors
j. Seizures
k. Coma
#195 Lecture Outline
8. Maintain ABCs and establish vascular access.
a. Give normal saline at a to-keep-open rate.
i. If signs of shock are observed or if the child is dehydrated, give a fluid bolus of normal saline at 20 mL/kg as instructed by medical direction.
ii. Reassess the child’s response.
b. Determine the child’s blood glucose level.
i. If glucose level is low, treat with dextrose.
ii. Dextrose concentration and dosage are age dependent.
c. If IV access cannot be established, medical direction may order glucagon IM or intranasal (IN).
i. If given, place the child on his or her side after administration (unless contraindicated) because glucagon may cause nausea.
d. Give oral glucose gel only if the patient can swallow, has a gag reflex, and is alert or can be roused to alertness.
e. Repeat a blood glucose reading 10 to 15 minutes following the administration of glucose.
f. Reassess frequently thereafter until the level stabilizes.
#196 Lecture Outline
D. Congenital adrenal hyperplasia (CAH)
1. Autosomal-recessive disorder of an enzyme responsible for the metabolism of cortisol (steroidogenesis) and aldosterone in the adrenal glands
2. The most common form is due to 21-hydroxylase deficiency.
3. Males born appear normal, although some may exhibit signs of puberty as a toddler, including increased musculature, penis growth, pubic hair, and a lowering of the voice.
4. Females may be masculinized.
a. Enlarged clitoris may resemble a penis.
#197 Lecture Outline
5. Patients sometimes undergo:
a. Early pubertal development, pubic hair growth
b. Early growth acceleration
c. Development of facial hair
d. Short stature
e. Severe acne
6. Surgery can correct genital deformities early in life.
7. Dexamethasone may be prescribed to a pregnant woman prior to the infant’s delivery if the condition is diagnosed early in the first trimester of pregnancy.
8. When children with CAH become sick, their bodies may not be able to compensate because of the lack of cortisol.
a. Can lead to salt wasting from decreased aldosterone
9. Infants who present with salt-wasting crisis because of loss of urinary sodium may present with metabolic acidosis and hyperkalemia.
#198 Lecture Outline
10. Infants with this condition may have vomiting, poor weight gain, dehydration, and may progress to shock in the first few weeks of life.
11. Hypoglycemia may also be present.
12. If this condition is suspected, hydrocortisone and IV boluses of normal saline (and glucose if hypoglycemic) are needed.
13. Stress-dose steroids should be considered with suspected CAH.
a. Contact medical control before administration.
14. For children on chronic steroid replacement, ask parents if they have a stress-dose steroid regimen.
a. Parents usually know the appropriate dose if their child becomes ill.
b. If not, it is reasonable to give an extra dose of the child’s home steroid dose, which is often tripled (or given three times a day rather than once) during acute illnesses.
c. Consult with medical control.
15. For children who appear in shock, IV hydrocortisone or methylprednisone may be considered in consultation with medical control.
#199 Lecture Outline
E. Panhypopituitarism
1. The pituitary gland produces eight hormones.
2. Examples include:
a. Growth hormone
b. Adrenocorticotropic hormone (ACTH)
c. Follicle-stimulating hormone (FSH)
d. Thyroid-stimulating hormone (TSH)
e. Antidiuretic hormone (ADH)
3. Hypopituitarism
a. Pituitary gland does not produce normal amounts of some or all of its hormones.
b. Can be congenital
c. Secondary to tumors, infection or strokes, or develops after trauma or radiation therapy
d. Patients require hormone replacement therapy.
4. Because several pituitary hormones affect production of secretions of the adrenal glands, patients with panhypopituitarism can be at risk for adrenal crisis.
5. Panhypopituitarism: Inadequate production or absence of pituitary hormones, including:
a. ACTH
b. Cortisol
c. Thyroxine (T4)
d. Luteinizing hormone (LH)
e. FSH
f. Estrogen
g. Testosterone
h. Growth hormone
i. ADH
#200 Lecture Outline
6. Patients can present with symptoms similar to CAH, including:
a. Hypoglycemia
b. Dehydration
c. Poor weight gain or weight loss
d. Vomiting
e. Muscle cramping
f. Weakness
g. Dizziness
h. Hypotension
i. Tanning of the skin with gradual onset
7. Patients require IV fluid boluses with normal saline, glucose replacement, and replacement of steroids with IV hydrocortisone.
#201 Lecture Outline
8. Management by a pediatric endocrinologist is important.
9. Often these conditions are a result of the hypothalamus, rather than the pituitary gland.
10. These hormones control growth and sexual maturation.
a. Once hormone therapy is initiated, children can generally live a normal life.
11. Hormone replacement therapy needs to be continually monitored.
#202 Lecture Outline
F. Inborn errors of metabolism (IEM)
1. Group of congenital conditions that cause either accumulation of toxins or disorders of energy metabolism in the neonate
2. Characterized by failure to thrive and vague signs such as poor feeding
3. May be a family history of the disorder.
#203 Lecture Outline
4. Usually identified in infancy, IEMs are grouped into two categories (with selected examples presented here):
a. Disorders that result in toxic accumulations
i. Maple syrup urine disease: A genetic disorder that causes a buildup of the amino acids leucine, isoleucine, and valine
ii. Phenylketonuria: The body’s inability to break down the amino acid phenylalanine
b. Disorders of energy production or use
i. Hereditary fructose intolerance: A lack of aldolase B, the enzyme responsible for breaking down fructose
ii. Galactosemia: The inability to break down the simple sugar galactose
#204 Lecture Outline
5. Symptoms can vary significantly and include:
a. Poor weight gain, failure to thrive
b. Loss of milestones in development
c. Recurring vomiting and diarrhea
d. Skin problems
e. Dental deformities
f. Deafness
g. Blindness
h. Various cancers
6. A neonate with sepsis or who is critically ill should be assessed for an IEM.
#205 Lecture Outline
7. Dietary restrictions and replacements can control many of these disorders.
8. Some patients become hypoglycemic, particularly when sick or vomiting.
9. They may also be hypermetabolic when ill, so boluses of glucose and the use of 10% dextrose (D10) fluids may be necessary.
#206 Lecture Outline
XII. Pathophysiology, Assessment, and Management of Hematologic, Oncologic, and Immunologic Emergencies
A. Hematologic, oncologic, and immunologic diseases are common in pediatrics, ranging from cancers to bleeding disorders to immune deficiencies.
1. Immunosuppression may be due to:
a. Cancer
b. Congenital diseases of the immune system
c. Chronic steroid use
d. Chemotherapy
e. Immunosuppressive medications after transplantation
f. Infections like human immunodeficiency virus (HIV)
2. May present with severe illness and shock.
3. Tachycardia associated with a fever or hypothermia should indicate possible sepsis.
4. When patients are ill, the oxygen-carrying capacity of hemoglobin is altered, resulting in decreased oxygen-carrying capacity.
5. Oxygen supplementation is important if you suspect sepsis.
#207 Lecture Outline
6. Special considerations besides sepsis include:
a. Acute chest syndrome associated with sickle cell crisis
b. Stroke with sickle cell crisis
c. Tumor lysis syndrome in chemotherapy patients
d. Increased overall risk of infection
7. May also have increased or decreased tendencies to clot.
#208 Lecture Outline
8. Patients with congenital or acquired immunodeficiencies are at high risk for recurrent infections and invasive disease.
a. Bacterial, viral, and fungal organisms can quickly lead to severe morbidity, mortality.
b. Quickly assess patients for signs of sepsis and decompensation.
c. Examination should include:
i. Thorough lung, circulatory, and neurologic examination
ii. Evaluation of the extremities for swollen joints that could be a sign of infection, hemarthrosis (bleeding into the joint), or a pain crisis
d. Delay in capillary refill and diminished peripheral pulses can indicate early sepsis.
#209 Lecture Outline
9. Because some patients with hematologic, oncologic, and immunologic problems have indwelling catheters such as peripherally inserted central catheter lines, Broviacs, and Port-A-Caths, evaluation of the catheter site for erythema, swelling, and tenderness is imperative.
a. There can be signs of central line infections that warrant early initiation of antibiotics after blood cultures are obtained.
#210 Lecture Outline
B. Sickle cell disease
1. Genetically inherited autosomal-recessive disorder of red blood cells
2. Causes the red blood cells to be misshapen, resulting in poor oxygen-carrying capability and potentially lodging of the red blood cells in blood vessels or the spleen.
a. Leads to vascular occlusion and subsequently to ischemia and painful crises
3. Sickle cell vasoocclusive episodes can be precipitated by hypoxia, infection, fever, dehydration, cold environment, and acidosis.
#211 Lecture Outline
4. An infant experiencing a vasoocclusive crisis may present with fussiness, irritability, crying, poor feeding, and other nonspecific findings.
5. Older children may report pain in specific locations, including joints, back, and chest.
#212 Lecture Outline
6. Opioids manage the pain due to vasoocclusive episodes.
a. These medications are sometimes inadequate in controlling severe painful episodes.
7. Ask about any medication taken since the onset of the present pain.
#213 Lecture Outline
8. Treatment includes oxygen, IV fluids, and opioids.
#214 Lecture Outline
C. Bleeding disorders
1. Abnormality in clotting of the blood
2. Development of a thrombosis can occur in either arterial or venous blood vessels.
3. Symptoms depend on the following:
a. Location of clot
b. Size of clot
c. Whether clot becomes dislodged and travels to another part of the body
4. Most bleeding is the result of trauma, but with a bleeding disorder, bleeding may be more severe or spontaneous.
#215 Lecture Outline
5. Consider how to best control the bleeding, if possible.
6. Direct pressure, packing, and the judicious use of tourniquets may be necessary.
7. Fluid replacement with boluses of isotonic fluids is necessary until patient is at a hospital.
8. Bleeding may be drug induced, inherited, or acquired.
9. Drugs such as aspirin and the nonsteroidal anti-inflammatory drugs (eg, ibuprofen) can cause a decrease in platelet adhesion, making patients more prone to bleeding.
10. Medications such as aspirin, warfarin (Coumadin), and heparin interfere with the clotting cascade and decrease the tendency to form a clot.
11. Over-the-counter medications (ginkgo biloba, ginger, vitamin E, ginseng, and garlic) and some antibiotics can also increase bleeding tendencies.
12. Ethanol use or diseases that affect the liver can lead to bleeding by decreasing the liver’s capacity to synthesize the factors needed in the clotting cascade.
#216 Lecture Outline
13. Thrombocytopenia
a. Abnormally low number of platelets in the blood
b. Causes include infections, cancers such as leukemia, rheumatologic diseases such as lupus, and splenic sequestration
c. Some inherited conditions may also cause low platelet counts.
d. Many medications (including valproic acid used to treat seizures) and chemotherapy drugs can reduce the platelet count.
e. Besides spontaneous bleeding or prolonged bleeding with injury, patients with low levels of platelets may exhibit petechiae or purpura.
f. Large bruises may develop from minimal injuries or with no history of injury.
g. Physical abuse should always be considered in children with unexplained bruising until proven otherwise.
#217 Lecture Outline
h. Treatment includes treating the underlying cause if present and transfusing platelets if bleeding cannot be controlled with local measures.
i. Consultation with a hematologist is required, so do not delay transport.
#218 Lecture Outline
14. Hemophilia
a. Genetic disorder usually inherited from the mother
b. Significant decrease in one of the clotting factors, or proteins in the blood that work with platelets to help blood to clot
c. More difficult for bleeding to stop
d. A child with severe factor deficiencies can experience hemorrhage after minor trauma.
e. Spontaneous bleeding into the joints (particularly the knees, elbows, and ankles) and IM hemorrhages are common.
f. Intracranial hemorrhage is one of the major causes of death.
#219 Lecture Outline
g. Patient and patient’s family learn to treat patient:
i. Family of the child who is 2 to 3 years of age is taught how to perform venipuncture and administer clotting factors.
ii. The child learns how to self-administer clotting factors between the ages of 8 and 12 years.
h. Recognize signs of internal bleeding.
#220 Lecture Outline
i. Be alert for signs of cerebral bleeding:
i. Headache
ii. Slurred speech
iii. Altered mental status
j. Be alert for signs of GI bleeding, such as black, tarry stools.
k. Provide supportive care:
i. Supplemental oxygen
ii. IV fluids
#221 Lecture Outline
15. Von Willebrand disease
a. Bleeding disorder in which the patient is missing the von Willebrand factor (a protein essential for platelet adhesion)
i. Prevents the blood from clotting well
ii. Most people with the disease are undiagnosed.
#222 Lecture Outline
b. Several types ranging from mild (nosebleeds) to severe with uncontrolled bleeding tendencies
c. Treatment involves bleeding control and transport to hospital with hematology services.
#223 Lecture Outline
D. Leukemia/lymphoma
1. In children, two forms of leukemia are generally recognized:
a. Acute lymphoblastic leukemia
b. Acute myelogenous leukemia
2. At its onset, the child with leukemia often displays few symptoms.
3. The condition may be diagnosed when a child has had a minor infection, such as a cold, but continues to be febrile, listless, and pale with little appetite.
4. Parents seek medical attention upon noticing:
a. Weight loss
b. Bruising without cause
c. Complaints of bone and joint pain
5. At other times the diagnosis of leukemia is made following an unrelated event, such as a routine physical exam before playing sports.
#224 Lecture Outline
6. Treatment of leukemia involves the use of IV chemotherapy and may involve radiation therapy.
7. Patients are susceptible to:
a. Bacteremia
b. Sepsis
c. Shock
8. Fluid therapy should be aggressive in patients who are:
a. Tachycardic (first sign of sepsis)
b. Hypotensive (late sign of sepsis)
9. Patients with lymphoma generally require treatment involving chemotherapy or radiation therapy.
11. These patients may be in constant pain and require supportive care and pain management en route to an appropriate receiving facility.
#225 Lecture Outline
XIII. Pathophysiology, Assessment, and Management of Toxicologic Emergencies
A. Toxic exposures account for a significant number of pediatric emergencies.
1. Can take the form of ingestion, inhalation, injection, or application of a substance
2. Toddler or preschool-age child
a. Most likely to have an unintentional exposure
b. Ingestion tends to involve small quantities of a single cleaning product, cosmetic product, or plant, or a few pills.
3. Adolescents
a. Recreational drug use or suicide attempts
b. Often involve multiple agents
4. Greater morbidity and mortality in adolescents, though in small children, toxic effects of some medications are such that “one pill can kill.”
#226 Lecture Outline
B. Assessment of toxicologic emergencies
1. Evaluation follows standard assessment sequence.
a. Identify agents to which the child was exposed, the quantity, and the route and time of exposure.
b. Note vital signs, pupillary changes, skin temperature and moisture, and any unusual odors.
2. Attend to ABCDEs as indicated.
a. Ingestion of some common substances can lead to hypoglycemia:
i. Ethanol and other alcohols, insulin, oral hypoglycemic agents, and beta-blockers
b. Treat documented hypoglycemia.
3. If child is in stable condition obtain additional history on scene using SAMPLE and perform secondary assessment.
#227 Lecture Outline
4. Look for toxidromes by assessing mental status, pupillary changes, skin CTC, GI activity (bowel sounds, emesis, or diarrhea), and abnormal odors.
5. Reassess frequently.
6. Children with potentially life-threatening toxic exposures may be asymptomatic on your arrival.
a. Dose in accidental toddler ingestion may be high.
7. Collect any pill containers or bottles, and transport them with the patient to the hospital.
#228 Lecture Outline
C. Management of toxicologic emergencies
1. Begins with supportive care and ABCDEs
2. Other options include:
a. Reducing absorption by decontamination
b. Enhancing elimination
c. Providing an antidote
3. Pay special attention to risks of environmental exposures for the EMS crew, who may also require decontamination measures.
#229 Lecture Outline
4. If you are not sure about toxicity, call national Poison Center hotline.
a. Available 24 hours a day
b. 1-800-222-1222.
#230 Lecture Outline
5. Decontamination
a. With skin exposure, remove all clothing and wash skin thoroughly.
b. With ocular exposure, immediately wash out the eyes.
c. For ingested toxins, options to reduce gastric absorption include dilution, gastric lavage, and activated charcoal.
i. Depending on substance, it may be useful to dilute the substance with a glass of milk or water.
ii. Decide in conjunction with poison center or medical control physician or nurse, depending on your protocols.
d. If the child has any airway or breathing concerns, do not allow the child to drink.
e. Syrup of ipecac is no longer recommended by American Academy of Pediatrics.
i. Does not remove significant amounts of ingested toxins and can cause prolonged emesis
f. Most common method for GI decontamination in the ED setting is activated charcoal.
i. Absorbs many ingested toxins in the gut, making less toxin available for systemic absorption if administered within the first hour after exposure
ii. Some common toxins do not bind to charcoal—for example, heavy metals, alcohols, hydrocarbons, acids, and alkalis.
iii. Messy to administer and rarely readily accepted by pediatric patients
iv. Risk of severe chemical pneumonia if aspirated
v. May be best given in the hospital setting
vi. If given in the field, typical dose is 1 g/kg.
#231 Lecture Outline
g. For substances that are renally excreted, diuresis may be beneficial.
i. IV fluids can increase diuresis, as can mannitol.
ii. Some substances have enhanced excretion in an alkali environment, such as salicylates and methyl alcohol (antifreeze or wood alcohol).
iii. Using sodium bicarbonate to alkalinize urinary pH can be beneficial.
h. Dialysis
i. Required for some overdoses and those that do not improve with other therapies.
ii. Can help with:
(a) Salicylates
(b) Lithium
(c) Methyl alcohol
(d) Ethylene glycol
(e) Barbiturates
#232 Lecture Outline
i. If substance is inhaled, assess patient’s respiratory status.
i. Bronchodilators may be needed for bronchial irritation and bronchospasm.
ii. Monitoring of oxygen saturations and intubation may be necessary, particularly with inhalational injuries associated with house fires.
iii. With soot in the upper airway, stridor, or swelling of the upper airway, early intubation is indicated.
j. Carbon monoxide inhalation injuries may be difficult to diagnose because oxygen saturation level will be near 100%.
i. Place patients on a nonrebreathing mask until blood carboxyhemoglobin levels can be checked at the hospital.
#233 Lecture Outline
6. Enhanced elimination
a. Cathartics such as sorbitol or magnesium citrate are sometimes combined with activated charcoal.
b. Work by speeding up elimination
c. Not recommended for young children.
i. Known to cause significant diarrhea with serious—sometimes life-threatening—electrolyte abnormalities
#234 Lecture Outline
7. Antidotes
a. Can be lifesaving but are available for only a few poisons
b. Work by reversing or blocking the effects of the ingested toxin
c. Dose depends on child’s weight
#235 Lecture Outline
XIV. Pathophysiology, Assessment, and Management of Psychiatric and Behavioral Emergencies
A. You will encounter children with behavioral and psychiatric problems including out-of-control behavior or suicide attempts.
1. EMS calls for behavioral emergencies are increasing.
a. Of children between 13 and 18 years old, 21.4% either currently or in their life have had a seriously debilitating mental disorder.
#236 Lecture Outline
2. Many of these problems begin as simple complaints not easily recognized by health care providers.
a. When not treated properly, such problems usually persist into adulthood.
3. Medical professionals have given increased attention to mood disorders, anxiety, and other behavioral problems in this population:
a. Suicide is the second leading cause of death in adolescents and the second leading cause of death in children between ages 10 and 14 years.
4. Children also are more likely to have coexisting problems (eg, attention-deficit/hyperactivity disorder, conduct disorder, and oppositional defiant disorder) along with the more traditional mental health disorders.
#237 Lecture Outline
B. Safety
1. Safety is your first priority.
2. Approach the child calmly, and explain you are there to help.
3. Address patient directly when obtaining history; explain what you are doing and why.
4. Some children are flight risks.
a. Determine how best to deploy your squad so the child does not leave the scene.
5. Answer questions honestly.
#238 Lecture Outline
6. A small percentage of children cannot be safely talked down for transport and must be mechanically restrained for everyone’s protection.
a. May be a task for EMS or law enforcement.
b. Carefully document the reason; keep restraints in place until arrival at the ED.
c. Avoid using chemical restraints.
#239 Lecture Outline
C. Assessment and management of psychiatric and behavioral emergencies
1. Mental health problems in children are difficult to diagnose.
2. Causes are:
a. Organic
b. Genetic
c. Environmental
3. Cultural and ethnic factors also blur the line between normal and abnormal coping mechanisms.
#240 Lecture Outline
4. Abnormal findings in the developmental and mental status examinations often are related to:
a. Adjustment disorders
b. Stress
5. Assessment of any child must include suicide risk.
#241 Lecture Outline
6. PAT gives a general impression of mental status and cardiovascular stability.
7. Child who has attempted suicide by ingestion may have life-threatening medical complications that take precedence over psychiatric concerns.
8. In the absence of acute medical issues, the bulk of your assessment will be based on observation and history.
9. In cases involving an agitated child, hands-on assessment may be limited.
10. Treat medical problems or injuries with standard protocols.
#242 Lecture Outline
XV. Pathophysiology, Assessment, and Management of Fever Emergencies
A. Fever is a common pediatric complaint but often not a true medical emergency.
1. A symptom of an underlying infectious or inflammatory process, fever can have multiple causes.
2. Most fevers are caused by viral infections.
a. Often mild and self-limiting
b. Sometimes a symptom of a more serious bacterial infection
3. General impression and primary survey will help you determine severity.
a. Young children with a fever can look quite ill.
#243 Lecture Outline
b. Record temperature, although height of fever does not reflect severity of illness.
c. With young infants, rectal temperature is most accurate.
d. Look for signs of respiratory distress, shock, seizures, stiff neck, petechial or purpuric rash, or a bulging fontanelle in an infant.
i. May tip you off to the presence of pneumonia, sepsis, or meningitis.
ii. All can be life threatening and require prompt transport.
4. Infants younger than 2 months should always be considered at risk for serious infection.
a. Fever may be the only sign of a potentially life-threatening illness.
b. Regardless of how well child looks, assess and transport quickly.
i. All children younger than 28 days with a fever, and most children younger than 2 months of age will require admission to the ED.
#244 Lecture Outline
5. History taking and secondary assessment will help you to determine the underlying cause of the fever and the severity of illness.
a. Perform on scene if child is stable, en route if seriously ill.
b. Ask about vomiting, diarrhea, poor feeding, headache, neck pain or stiffness, and rash.
c. History of infectious exposure may provide clues to cause of current illness.
d. May also identify a child at high risk for serious bacterial illness.
i. Sickle cell disease, HIV infection, and childhood cancers may all lead to an immunocompromised state.
#245 Lecture Outline
6. Child with a fever may require little intervention.
a. Support ABCs.
b. Provide temperature control.
c. Consider acetaminophen or ibuprofen; avoid aspirin in children.
i. Linked with Reye syndrome, a rare illness that can result in cerebral edema and liver failure
d. Limit other cooling measures to undressing.
7. Transport to an appropriate medical facility.
#246 Lecture Outline
XVI. Child Abuse and Neglect
A. Child abuse is any improper or excessive action that injures or otherwise harms a child or infant; it includes physical, sexual, and emotional abuse as well as neglect.
1. In the United States, a report of child abuse is made every 10 seconds.
2. In 2014, state agencies identified an estimated 1,580 children who died as a result of abuse and neglect—between 4 and 5 children per day.
a. More than 70% of the children who died as a result of child abuse or neglect were 2 years of age or younger.
b. More than 80% were not yet old enough for kindergarten.
c. Around 80% of child maltreatment fatalities involve at least one parent as perpetrator.
3. Definitions of abuse
a. Physical abuse: Inflicting injury to a child.
b. Sexual abuse: An adult engaging in sexual activity with a child, ranging from inappropriate touching to intercourse.
c. Emotional abuse and child neglect: Often difficult to identify, may go unreported.
d. Neglect: Refusal or failure on the part of the caregiver to provide life necessities.
e. Emotional abuse: Lack of emotional support by the caregiver.
#247 Lecture Outline
4. Abandonment
a. Occurs when a parent or guardian physically leaves a child without regard to the child’s health, safety, or welfare
b. Abandoned children (called foundlings):
i. May be found in a home where the parents or caregivers have left them without appropriate supervision
ii. May be dropped off in a location to be found by someone else.
c. Parents have relinquished consent authority, and EMS providers should render care without written or verbal consent.
d. Safe-haven laws allow parents to leave a child without fear of legal implications; children become wards of the state.
e. Children may be left unharmed by caregivers at the following locations:
i. Police stations
ii. Fire houses
iii. Hospitals
iv. Specialized infant boxes
f. All 50 states have passed safe-haven laws, but details vary from state to state.
5. Keep the possibility of abuse in mind with injured children.
a. Information you gather from scene size-up and interviews may prove invaluable.
b. Act on any suspicions of abuse.
#248 Lecture Outline
B. Risk factors for abuse
1. Risk factors:
a. Younger children
b. Children who require extra attention (eg, handicaps, chronic illnesses, other developmental problems)
c. Occurs in all socioeconomic levels, but more prevalent in lower socioeconomic status
d. Divorce, financial problems, and illness
e. Drug and alcohol abuse
f. Domestic violence in the home
#249 Lecture Outline
C. Suspecting abuse or neglect
1. When you are called to the home of an injured child and suspect abuse, trust your instincts.
2. Look for “red flags” (summarized in the mnemonic CHILD ABUSE):
a. History inconsistent with the type of injury—eg, a child who fell from a tree with bruises only on the buttocks
b. Account of the injury that is inconsistent with developmental abilities—eg, a 2-month-old infant rolling off a bed
c. An old injury that went unreported
d. Inappropriate actions or language from the caregiver
D. Assessment and management of abuse and neglect
1. To recognize abuse, you first have to suspect it.
#250 Lecture Outline
2. Carefully document what you see.
a. Remain impartial
b. Record what you see and hear in a detailed incident report.
i. Include notes about child’s environment, condition of home, and interactions among caregivers, child, and EMS crew.
ii. Record concerning comments verbatim, who made them, and when.
c. In all states, prehospital personnel are legal obligated to report suspicion of abuse to child protective services (CPS) and law enforcement
i. Failure to report may be a crime; review state law.
d. Reporting is done in conjunction with emergency physicians, social workers, and child protection teams at the ED.
#251 Lecture Outline
e. Involve police early to secure the crime scene and collect evidence.
f. In cases where death occurs, the medical examiner will investigate the cause of death.
i. Notify of any death if child is not being transported to the ED.
3. Approach ED staff with concerns, not the caregiver.
4. Be aware of local regulations.
5. Scene can be emotional; focus on trauma assessment and management and on the child’s safety.
a. Base general impression on PAT; may range from normal to grossly abnormal.
b. Shaken baby syndrome: May find abnormal appearance, no external signs of injury
#252 Lecture Outline
6. Few caregivers will admit to having hurt the child; be alert for a history that is inconsistent with the clinical picture.
a. Lookfor bruises, especially in different stages of healing or in concerning locations.
b. Active toddlers often have bruises on their shins but rarely on backs or buttocks.
c. Bruises in identifiable patterns are rarely incurred accidentally.
d. Use CHILD ABUSE mnemonic when you obtain additional history.
#253 Lecture Outline
7. Mimics of abuse
a. Can be difficult to distinguish some normal skin findings from inflicted injuries.
i. Mongolian spots
(a) Birthmarks generally found on the lower back and buttocks of children of Asian or African American descent
(b) May be mistaken for bruises because of their unique bluish coloring
#254 Lecture Outline
ii. Other medical conditions can mimic bruises.
(a) Purpura of meningitis, Henoch-Schönlein purpura
(b) Petechiae of idiopathic thrombocytopenic purpura and leukemia
iii. Exposure to sun can cause reactions with certain medications or fruits (limes, mangos).
(a) Causes phytophotodermatitis, reddish-purple skin discolorations
#255 Lecture Outline
iv. Certain cultural customs also produce skin markings that can mimic child abuse.
(a) Coining and cupping: Traditional Asian practices, often used to treat fever
(b) Markings can be impressive but practice is not harmful.
#256 Lecture Outline
XVII. Sudden Infant Death Syndrome (SIDS)
A. Sudden unexpected infant death (SUID) is the death of an infant younger than 1 year that occurs suddenly and unexpectedly, the cause of which is not immediately obvious before investigation.
#257 Lecture Outline
1. Most SUIDs are reported as one of three types:
a. SIDS
i. Formerly known as crib death
ii. The sudden death of an infant younger than 1 year that cannot be explained after a thorough investigation is conducted, including:
(a) A complete autopsy
(b) Examination of the death scene
(c) A review of the clinical history
iii. About 1,600 infants died of SIDS in 2015.
iv. Leading cause of death among infants 1 to 12 months old.
b. Unknown cause
i. The sudden death of an infant younger than 1 year may remain undetermined because one or more parts of the investigation was not completed.
c. Accidental suffocation and strangulation in bed
i. The sudden death of an infant younger than 1 year can happen because of suffocation by:
(a) Soft bedding
(b) Overlay
(c) Wedging or entrapment
(d) Strangulation
2. Devastating to families and EMS crew who responds to the call
#258 Lecture Outline
B. Assessment and management of SIDS
1. Typical scenario for a SIDS call:
a. Healthy infant put down for a nap, later found dead in bed.
b. On arrival of EMS, baby will be lifeless and, depending on discovery time, may have rigor mortis and dependent lividity.
c. Frothy or blood-tinged fluid in the mouth or nose or on the bedding is typical.
2. Be alert for clues to other potential causes of death, such as trauma, suffocation, or maltreatment.
3. Decision to start resuscitative efforts, or to stop CPR that was started by first responders or family members, can be difficult.
a. Guided by local protocols on declaring death in the field, patient assessment, and needs of the family.
b. Although victim cannot be resuscitated, failure to initiate care may not be acceptable to the shocked family.
c. Hospital-based social services for the family may be an important resource.
d. In cases that meet the criteria for declaring death at the scene and nontransport, notify the coroner, medical examiner, or law enforcement personnel, as dictated by local protocol, so that appropriate scene investigation can be undertaken.
e. Mobilize support for the survivors:
i. Chaplain or minister, SIDS team, social worker, other family members
4. Thorough scene size-up and history are important.
a. History of recent illnesses, chronic conditions, medications, or trauma may decrease the likelihood of SIDS as the cause of death.
b. Presence of pillows, stuffed toys, window blind cords, or sheepskin in the baby’s crib may make suffocation a possibility.
#259 Lecture Outline
XVIII. Brief Resolved Unexplained Event
A. An episode during which an infant becomes pale or cyanotic; chokes, gags, or has an apneic spell; or loses muscle tone.
1. Formerly known as an apparent life-threatening event (ALTE)
2. Causes may include benign and serious diagnoses.
a. Benign: Brief episode of laryngospasm during feedings or gastroesophageal reflux
b. Serious: Sepsis, congenital heart disease, and seizures
3. Once thought of as existing along a spectrum with SIDS, but recent evidence demonstrates they are not related.
4. Common to find a distraught caregiver and a well-appearing baby
#260 Lecture Outline
5. Provide life support with signs of cardiorespiratory compromise or altered mental status.
6. Transport all infants with a history of BRUE.
7. Challenging age group to assess; overtriage is safest path.
a. BRUEs may be associated with serious underlying illness.
b. Failure to transport may have grave consequences for the child.
#261 Lecture Outline
XIX. Pathophysiology, Assessment, and Management of Pediatric Trauma Emergencies
A. Age-related anatomy and physiology make injury patterns and responses to trauma different from those seen in adults.
1. Developmental stage will affect response to injury.
2. For a young child, being strapped to a backboard may be as traumatic as the injury leading to the EMS call!
#262 Lecture Outline
B. Pathophysiology of traumatic injuries
1. Blunt trauma is the MOI in most pediatric injury cases.
a. Less muscle and fat mass leads to less protection against the forces transmitted.
#263 Lecture Outline
2. Falls are common; injuries will reflect child’s anatomy child and height of fall.
a. Eg, 6-year-old playing on the monkey bars is most likely to sustain an upper extremity fracture when falling onto an outstretched arm.
i. Internal or head injuries would be uncommon with this mechanism.
b. An infant, with a big head and no protective reflexes, who falls out of a shopping cart will commonly have a skull fracture, and could have intracranial hemorrhage.
c. Falls from a standing position usually result in isolated long bone injuries.
d. High-energy falls may result in multisystem trauma.
e. Injuries from bicycle handlebars typically produce compression injuries to intra-abdominal organs.
i. Duodenal hematomas, pancreatic injuries, upper extremity injuries are common.
ii. Consider head injury if patient went over the handlebars, especially if not wearing a helmet.
#264 Lecture Outline
3. Motor vehicle crashes can result in a variety of injury patterns depending on use of restraints, position in car.
a. For unrestrained passengers, assume multisystem trauma.
b. Restrained passengers may sustain chest and abdominal injuries associated with seat belt use.
c. Suspect spinal fractures with chest or abdominal bruising in a seat belt pattern.
d. Air bags can cause head and neck injuries in young children.
e. Multisystem trauma is likely with vehicle-pedestrian collisions.
i. Chest, abdominal, and lower extremity injuries occur on impact.
ii. Head and neck injuries may result from the fall when the child is thrown.
#265 Lecture Outline
C. Assessment and management of traumatic injuries
1. Begin with a thorough scene size-up:
a. Address safety concerns.
b. Determine MOI or NOI.
c. Note number of patients.
d. Follow standard precautions.
e. Determine whether additional resources are needed.
2. Use PAT to form a general impression.
a. If findings are grossly abnormal, quickly move to ABCs.
b. Immediately think of head injury with abnormal appearance.
i. With isolated closed head injury, breathing and circulation may be normal.
c. Abnormal appearance may reflect inadequate oxygenation of the brain owing to shock or respiratory failure.
d. Abnormalities in work of breathing will tip you off to chest or airway injury and abnormal circulation to a hemorrhage problem.
e. If multisystem injuries are present, all three sides of the PAT may be abnormal.
3. Initiate life support interventions as you identify problems.
a. Assess the airway for obstruction with teeth, blood, vomit, or edema.
i. Suction as needed.
b. For cervical spinal injury, open airway with jaw-thrust maneuver.
c. If child cannot maintain the airway, consider an NG or oropharyngeal airway.
d. If you attempt ET intubation, maintain cervical spinal precautions.
e. Emergency surgical airways in a child have several complications and a high failure rate.
i. Tracheotomy should be reserved for surgeons in a controlled setting.
ii. Remote chances of needing to perform a needle cricothyrotomy in a child
(a) In younger children, identification of the cricothyroid membrane is difficult.
4. Breathing assessment includes evaluation for symmetric chest rise and equal breath sounds.
a. 100% supplemental oxygen
b. Bag-mask ventilation as needed
c. NG or OG tube for stomach decompression
#266 Lecture Outline
5. Pneumothorax: Not common in pediatric blunt chest injury, but may be present with penetrating trauma of the chest or upper abdomen
a. Jugular venous distention and tracheal deviation less likely in a child
b. If MOI suggests a possible tension pneumothorax and child is in significant respiratory distress, perform needle decompression.
c. Signs and symptoms of tension pneumothorax:
i. Tachycardia
ii. Difficult ventilation despite an open airway
iii. Absent or decreased breath sounds on affected side
iv. Jugular vein distention (may not be present with associated hemorrhage)
v. Hyperresonance to percussion on affected side
vi. Tracheal deviation away from affected side (late sign, not always present)
vii. Pulsus paradoxus
#267 Lecture Outline
d. Tracheal deviation, hyperresonance, pulsus paradoxus, and decreased breath sounds can be difficult to assess in a young child.
i. Tracheal deviation is a late finding, and tension pneumothorax can be present without it.
ii. Use a large-bore IV catheter, preferably 14 to 16 gauge.
iii. Locate the second or third intercostal space in the midclavicular line on the affected side.
iv. Insert the needle at a 90° angle, just superior to the third rib.
#268 Lecture Outline
6. Any trauma patient should be considered to be at risk for developing shock
a. Assess circulation by checking pulse rate and quality, capillary refill, skin temperature, and blood pressure.
b. In pediatric patients, the only sign of compensated shock might be an elevated pulse rate.
i. Children have a remarkable capacity for peripheral vasoconstriction.
ii. Can maintain blood pressure despite significant blood loss
c. If MOI is concerning and child is tachycardic, assume compensated shock and initiate volume resuscitation with 20 mL/kg of isotonic fluid.
d. Ideally, insert two peripheral IV lines, but an IO line may be best in a child with hemorrhagic shock.
e. Control external bleeding.
7. Once ABCs are stabilized, continue assessment of disability with AVPU.
a. Assessment of appearance in the PAT will already have identified an altered level of consciousness.
b. Check pupils and motor function.
#269 Lecture Outline
8. Place a cervical collar and immobilize on a long backboard as indicated.
9. If increased ICP is a concern, keep the head midline to facilitate jugular venous return to the heart.
a. If child is not in shock, elevate the backboard or head of the stretcher to 30°.
b. Perform shock resuscitation with IV fluids.
c. If child has acute signs of herniation such as a “blown” pupil or Cushing triad, consider mild hyperventilation guided to an end-tidal carbon dioxide level of 30 to 35 mm Hg and administer mannitol.
10. Perform a rapid exam to identify all injuries.
a. Log roll the child to examine back and buttocks.
11. Cover the child with blankets.
a. Cover the head, especially in infants and young children.
b. Avoid drafts from heating or air conditioning units.
c. Consider warm IV fluids, warm oxygen, and warm patient transport environment.
d. Remove wet clothing.
12. Treat any fractures as you would in an adult.
#270 Lecture Outline
D. Transport considerations
1. Some traumas are load-and-go because of severe injuries and unstable condition.
a. Trauma involving an ominous MOI regardless of how the child looks on scene
b. Unstable or compromised airway
c. Shock
d. Difficulty breathing
e. Severe neurologic disability
2. For these situations, perform lifesaving procedures on scene or en route, and quickly transfer to an appropriate trauma center according to local protocols.
#271 Lecture Outline
3. All trauma victims with suspected spinal injury require appropriate spinal stabilization.
a. Do not place a collar that is too big on a small child—use towel rolls and tape to immobilize the head.
i. Apply tape across temples and forehead.
ii. Avoid chin or throat; may impair ventilation.
b. Use a pediatric immobilizer with a recess for the child’s large occiput.
c. Place a towel or small blanket under the shoulders and back to prevent neck flexion in infants and toddlers.
4. To properly immobilize a child, refer to Skill Drill 43-6; follow the steps in Skill Drill 43-7 to immobilize an infant.
5. Nearest appropriate facility depends on local protocols, capabilities of local EDs.
#272 Lecture Outline
E. History taking and secondary assessment
1. If patient is stable obtain additional history and perform a more thorough physical exam.
a. Full-body, back-to-front detailed physical exam en route for all trauma patients with significant MOI.
b. For infants, this includes checking anterior fontanelle for bulging.
c. Look for bruises, abrasions, other subtle signs of injury that may have been missed.
#273 Lecture Outline
F. Fluid management
1. Airway management and ventilatory support take priority over management of circulation.
a. Tachycardia is usually the first sign of circulatory compromise in a child.
i. Can also be caused by agitation, being scared, or being restrained
b. Hypotension is a late finding in pediatric trauma.
c. Recognizie circulatory compromise and treat it early!
#274 Lecture Outline
d. Consider the following when establishing vascular access in the injured child:
i. Large-bore IV catheters should be inserted into a large peripheral vein whenever possible.
ii. In infants and young children, 20- or 22-gauge IV needles may be considered “large bore.”
iii. Definitive care can only be provided at the ED, so never delay transport to start an IV line; perform en route.
iv. To maintain perfusion, administer an initial bolus of 20 mL/kg using an isotonic crystalloid solution.
(a) Frequently reassess vital signs, and provide additional IV fluid boluses of 20 mL/kg if no improvement is noted.
(b) Up to 60 mL/kg can be given for resuscitation of a pediatric patient.
(c) If patient is over 50 kg, use adult resuscitation fluid volumes.
(d) If condition does not improve following two boluses of an isotonic crystalloid, blood loss is likely severe and the patient may need surgical intervention. Provide rapid transport with continuous monitoring en route.
e. If the child is hypotensive and IV access cannot be obtained within 90 seconds, consider inserting an IO needle.
#275 Lecture Outline
G. Pain management
1. Pain is often undertreated in young children; do not overlook signs.
2. Consider pain assessment as important as vital signs.
a. Use one of many tools to elicit the child’s self-report of pain level.
b. Tachycardia and inconsolability may be the only way a child has to express pain.
c. Findings may be similar to those of early shock or fear.
3. Use a calm, reassuring voice, distraction techniques, and medications when appropriate.
a. Commonly used pain medications include morphine and fentanyl.
b. Intubated patients should receive pain medication and sedation if they are hemodynamically stable.
i. May need to be redosed depending on transport time.
ii. Can be used in conjunction with narcotics for patients in stable condition.
c. Side effects of narcotics and benzodiazepines include respiratory depression, hypoxemia, bradycardia, and hypotension.
d. Weigh benefits and risks of administering.
i. Children who are in shock and hemodynamically unstable are not good candidates for narcotics or sedatives.
ii. May worsen their condition
e. Carefully monitor vital signs.
#276 Lecture Outline
XX. Pathophysiology, Assessment, and Management of Burns
A. The initial assessment and management of pediatric burn victims is similar to that of adults, with a few key differences.
1. Higher skin surface–body mass ratio makes them more susceptible to heat and fluid loss.
2. Worrisome patterns of injury or suspicious circumstances should raise concerns of abuse.
#277 Lecture Outline
B. Assessment and management of burns
1. Scene safety is an important element.
a. Check for ongoing dangers such as fire, chemicals, or other hazardous materials.
2. From-the-doorway assessment may identify signs of smoke inhalation.
a. Eg, abnormal airway sounds, respiratory distress, soot around the nose
b. Quickly move patient and crew to a well-ventilated area.
3. Estimation of percentage of BSA burned may affect decisions on fluids, transport.
a. Adolescents: use rule of nines that you use for adults.
b. Younger children: modify rule to account for disproportionately larger head size.
c. Infants: Head and trunk each account for 18% of BSA; arms 9%; legs 13.5% each.
d. Size of child’s palm (not including fingers) represents about 1% total BSA.
#278 Lecture Outline
4. Burns suggestive of abuse include those in which the mechanism or pattern observed does not match history or child’s developmental capabilities.
a. Eg, a child who cannot stand is unlikely to pull a hot cup of coffee off a table.
b. Splash burns—as from tipping over a pot of boiling water—should have an irregular configuration because the hot liquid runs down the child’s body.
c. Be suspicious if a burn has clear demarcation lines or is on the buttocks.
5. Remove burning clothing, and support ABCs.
a. With signs of smoke inhalation, consider early intubation.
b. Give all burn victims 100% supplemental oxygen.
c. Smoke inhalation may cause bronchospasm resulting in wheezing and mild respiratory distress.
i. Consider a bronchodilator such as albuterol or epinephrine IM.
d. If possible, insert an IV line and initiate fluid resuscitation in transport for patients with more than 5% of burned BSA.
i. Start with 20 mL/kg of isotonic fluid.
ii. Reassess the need for additional boluses; large burns can lead to huge fluid shifts.
#279 Lecture Outline
6. Clean burned areas minimally to avoid hypothermia; cover with clean, dry cloth.
7. Avoid lotions or ointments; they can trap heat and bacteria.
8. Cover burn and patient as needed.
9. Analgesia is a crucial part of early management.
10. Transport to an appropriate medical facility once the patient’s condition is stabilized.
a. Larger burns, full-thickness burns, and burns involving the face and neck are best treated at a regional burn center.
#280 Lecture Outline
XXI. Children with Special Health Care Needs
A. Children with special health care needs include those with physical, developmental, and learning disabilities.
1. Broad range of causes, including premature birth, traumatic brain injury, congenital anatomic anomalies, and acquired illnesses
2. Advances in technology and drugs have enabled an increasing number of children with disabilities to receive care in the community.
B. Technology-assisted children
#281 Lecture Outline
B. Technology-assisted children
1. Tracheostomy tubes and artificial ventilators
a. Tracheostomy: Surgical procedure, involving creation of a stoma through which a tracheostomy tube can be placed for long-term ventilatory needs.
b. Reasons:
i. Long-term ventilator support for chronic lung disease
ii. Inability to protect the airway due to neurologic impairment
iii. Congenital airway anomaly leading to airway obstruction
#282 Lecture Outline
c. Caregivers are a source of valuable information and will generally have a spare tube.
d. Child may breathe spontaneously with room air if the function of the tube is simply to bypass mechanical upper airway obstruction.
e. With severe lung disease or problems with respiratory drive, child may depend on a home ventilator and supplemental oxygen.
f. Most common problem is obstruction of the tube with secretions.
g. Tube displacement is another potential problem.
h. With respiratory distress, assess tube position and suction tube.
i. If child is using a home ventilator, disconnect the circuit and provide bag-mask ventilation.
j. If child does not improve or is cyanotic or in severe distress, you may need to remove and replace the tube, preferably using a tube of the same diameter and length.
k. Confirm tube position as you would with an ET tube.
l. A small ET tube can be inserted through the tracheostomy.
m. A standard oral ET intubation can be performed.
n. Make sure the ET tube comes to rest below the level of the tracheostomy, or cover the tracheostomy and ventilate the patient with a bag-mask device.
#283 Lecture Outline
2. Gastrostomy tubes (G-tubes)
a. Surgically placed directly into the stomach through the skin and provide nutrition or medications, bypassing the oropharynx and esophagus
b. Some children depend on a G-tube for all of their nutrition.
c. For others, the tube supplements intake, ensures adequate nutrition.
d. Problems such as obstruction, dislodgment, or leakage of a G-tube are not uncommon but rarely represent an emergency.
e. Most calls can be managed by supportive care and transport.
f. Urgent physician evaluation is needed if a G-tube has been pulled out because the opening on the abdominal wall tends to constrict quickly, making replacement difficult.
#284 Lecture Outline
3. Central venous catheters
a. May be inserted for long-term IV access for medications or nutrition
b. Placed into large central veins, such as the subclavian
c. Completely implanted central lines, with a port or reservoir accessible under the skin, may be left in place for months to years.
i. Eg, common in children who are undergoing long courses of chemotherapy
d. Partially implanted central lines have tubing external to the skin.
e. Complications include infections, obstruction, and dislodged or broken catheters.
f. Infection of the central line: Possible redness, swelling, tenderness, or pus at the site of insertion; may have systemic signs of infection or signs of septic shock
g. Central line obstruction may be a medical emergency, depending on what is infusing through the line.
h. If child does not urgently need the infusion, assess and transport.
i. Dislodged or broken catheters may result in leakage of fluid or blood.
ii. Use sterile technique to clamp off the broken line to minimize risk of infection or air embolus.
i. On rare occasions, a child with a functioning central line will require emergency IV access for field treatment.
i. Look for peripheral access; avoid central line whenever possible due to high risk for infection.
#285 Lecture Outline
4. Ventricular shunts
a. Inserted to drain excessive fluid from the brain, normalizing ICP
i. Neurosurgeon places tube, connects it to a one-way, pressure-sensitive valve that runs from the enlarged ventricle into the abdominal peritoneal space.
ii. When pressure builds up in the ventricle, the one-way valve opens, and CSF drains into the peritoneum, where it is reabsorbed.
b. Obstruction occurs when the shunt tubing becomes blocked.
c. Without adequate fluid drainage, CSF fluid continues to accumulate, resulting in hydrocephalus.
i. Child will show signs of increased ICP; may range from subtle behavior changes to impending brain herniation.
ii. Typical symptoms include headache, fatigue, vomiting, and even coma.
d. Infection can result from bacterial contamination during the surgery to place the shunt or from bacteria in the blood adhering to and infecting the hardware.
i. Encountered most frequently within months of shunt surgery.
ii. Children are generally extremely sick, have a fever, and show signs of shunt obstruction.
#286 Lecture Outline
e. Shunt obstructions and infections are medical emergencies.
i. Transport for neurosurgical evaluation.
ii. Maintain continuous cardiopulmonary monitoring during transport.
f. Shunt obstruction may be recognized by signs and symptoms of increased ICP, including Cushing triad.
#287 Lecture Outline
C. Assessment and management of children with special health care needs
1. Follow standard pediatric assessment sequence.
2. Ask questions of the parent or caregiver to establish baseline neurologic function and physiologic status.
3. Meet every child at his or her developmental level.
a. An otherwise healthy 10-year-old with a perinatal brain injury may have the developmental skills of a toddler.
b. A 6-year-old with severe cardiopulmonary compromise may be ventilator-dependent and have an oxygen saturation level in the 80s but be cognitively intact.
4. Treatment goal is to restore a child to his or her own physiologic baseline.
a. Requires collaboration with caregivers to determine what is normal for the child and management strategies that have been successful in the past.
#288 Lecture Outline
D. Transport of children with special health care needs
1. Most children with special health care needs will have a medical home.
a. Hospital, clinic, or private practice where they receive care
2. Transporting to a facility where the clinical team is familiar with patient will streamline care.
3. If this is not possible, take any available medical records to assist the receiving team.
4. Take any assistive devices, including home ventilators and feeding pumps.
5. Most important, take the parent or caregiver!
a. It can be emotionally difficult for the child to be separated from the caretaker.
#289 Lecture Outline
XXII. An Ounce of Prevention
A. Emergency care for children involves a team approach by health care professionals in the community and in the ED.
1. To be an effective child safety advocate, you must be knowledgeable about local and national prevention programs.
#290 Lecture Outline
B. Emergency Medical Services for Children (EMSC) initiative
1. Federally funded program created more than 25 years ago to reduce child disability and death due to severe illness and injury
2. Works with local communities and hospitals to improve care in and out of the ED
3. Works with existing EMS systems to improve the quality of emergency care:
a. Pediatric-specific protocols and procedures
b. Child-appropriate equipment for ambulances and EDs
4. Supports training in pediatric-specific emergency care
#291 Lecture Outline
C. Prevention of injuries
1. Most injuries are predictable and preventable events.
2. Tracking injury patterns helps target areas for intervention and prevention.
#292 This table shows examples of common injuries and possible prevention strategies.