Pediatric Trauma- Anarea of concern
CNE- Trauma Care Nursing: Newer modalities perspectives and
Challenges
Venue- Base hospital , Delhi
cantonment Feb 9-10 , 2019
Prof. (Dr.) Smriti Arora
Amity College of Nursing
Amity University, Gurugram, Haryana
smritiamit@msn.com
2.
Introduction
• Injury isthe leading cause of death and disability in children
• accounts for a significant burden on countries with limited resources.
• There are anatomical, physiological, and emotional differences
between adults and children.
• The initial assessment and management of the injured child
follows
• primary survey and resuscitation, followed by
• secondary survey.
3.
Causes of pediatrictrauma
• Road traffic incidents , hit by vehicle
• Fall injuries – at home
• Interpersonal violence
• Submersion injury
• Homicide
• Suicide
• Fires
Primary and secondarysurvey
• Primary survey is quick, initial patient assessment to identify life
threatening injuries and involves active resuscitation.
• Secondary survey identifies other injuries, such as intra-abdominal
injuries and long-bone fractures, which can result in significant
hemorrhage.
• The relief of pain is also an important part of the treatment of an
injured child.
6.
Primary
survey
• starts atthe injury scene and aims to ensure a patent airway, adequate
breathing, circulatory support, and to assess major neurologic
disability.
• address life-threatening injuries that compromise oxygenation and
circulation.
• The priority of this initial phase is evaluation of the child's ABCDE.
• Every trauma patient should arrive boarded and C-spine
immobilized.
• Collar for school-age/adolescents and
• Rolls and tape for infants/toddlers
7.
AIRWAY
• Airway controlis the first priority.
• Unlike in adults, the cause of childhood cardiac arrest is an initial
respiratory arrest. A child's airway is anatomically different from
an adult’s.
• A child has a shorter neck, smaller and anterior larynx, floppy
epiglottis, short trachea, and large tongue.
• classic sign of upper airway partial obstruction- inspiratory
stridor
• complete airway obstruction- Respiratory effort with no air
flow
9.
Airway
• If theairway is obstructed, inspect the mouth for a foreign body and remove it,
but do not perform a blind finger sweep, which may push it further into the
airway.
• Suction to clear blood, secretions, or vomitus.
• oral intubation- , use the jaw-thrust maneuver to improve airway patency.
• All pediatric trauma patients must be assumed to have cervical spine injury until
proven otherwise. Thus, if oral intubation is indicated, in-line cervical spine
immobilization must be performed.
• Size of the ET tube- by the child’s 5th digit or by the formula (age + 16)/4.
• The subglottic trachea is the narrowest portion of the pediatric airway and
provides a "physiologic cuff," so use uncuffed ET tubes in children <8 years
in order to minimize tracheal trauma.
• Use a rapid-sequence intubation technique to facilitate successful
intubation.
11.
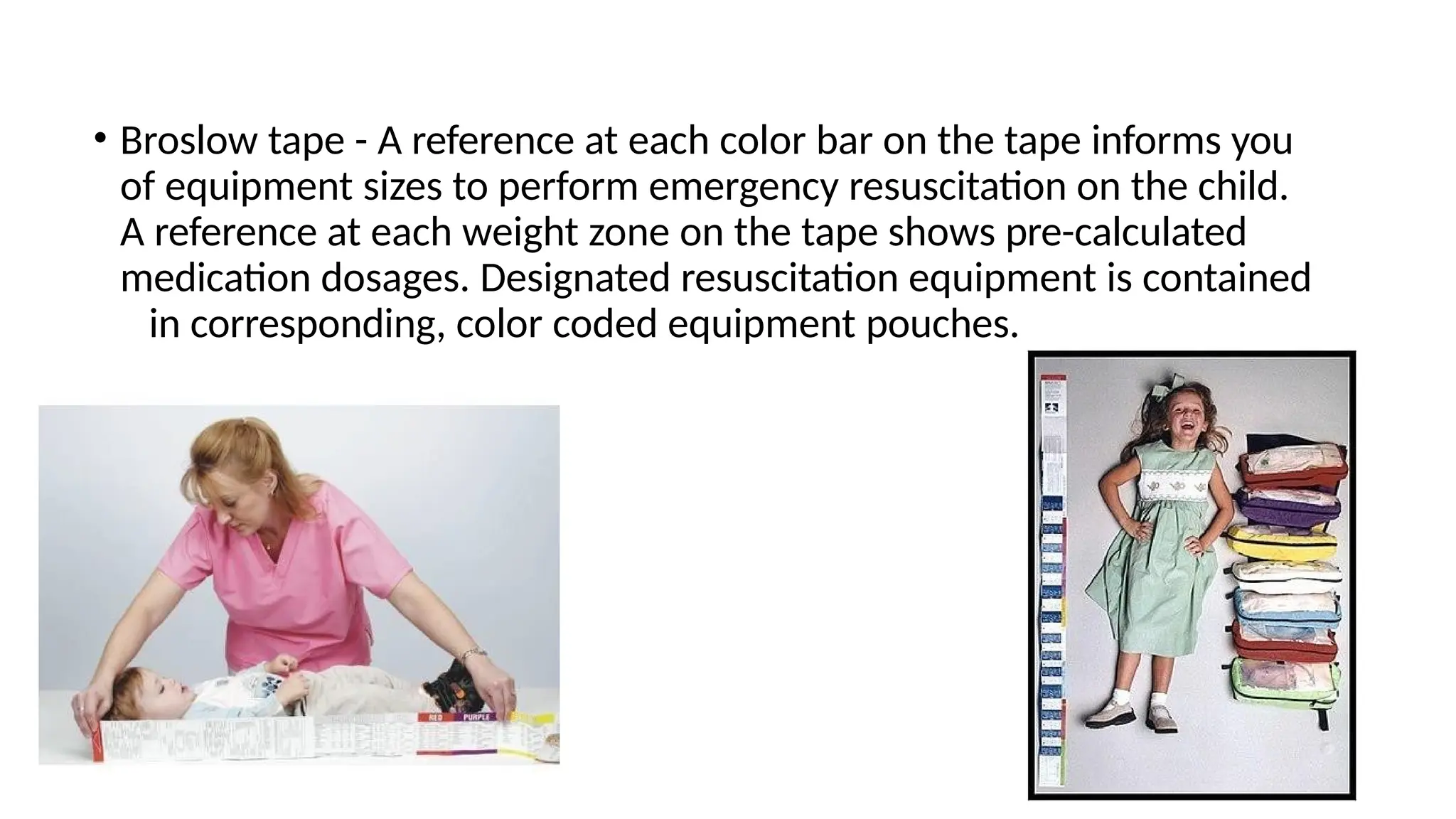
• Broslow tape- A reference at each color bar on the tape informs you
of equipment sizes to perform emergency resuscitation on the child.
A reference at each weight zone on the tape shows pre-calculated
medication dosages. Designated resuscitation equipment is contained
in corresponding, color coded equipment pouches.
13.
BREATHING
• Once apatent airway is established, carefully assess the child's breathing. If
respiration is inadequate, provide ventilatory assistance.
• Infants and small children are primarily diaphragmatic breathers; their ribs
lack the rigidity and configuration present in adults.
• As a result, any compromise of diaphragmatic excursion significantly limits
the child's ability to ventilate.
• Direct injury to the diaphragm, disruption and herniation of intra-
abdominal contents, or gastric distension (aerophagia) can severely
compromise the infant or small child's ability to breathe.
• The mediastinum of a child is very mobile; therefore, mediastinal
structures can shift into the contralateral hemithorax as a result of a simple
pneumothorax, hemothorax, or tension pneumothorax.
15.
Breathing
Anticipate respiratory failureif any of the following signs is present:
• an increased respiratory rate, nasal flaring, retractions, seesaw
breathing, or grunting;
• an inadequate respiratory rate, effort, or chest excursion (e.g.
diminished breath sounds or gasping), especially if mental status is
depressed;
• cyanosis with abnormal breathing despite supplementary oxygen.
• absent or asymmetric breath sounds - pneumothorax
17.
CIRCULATION
• Assess forhypovolemic shock.
• Tachycardia is usually the earliest measurable response to
hypovolemia.
• Other signs- mental status change, respiratory compromise, absence
of peripheral pulses, delayed CRT, skin pallor, and hypothermia are
all possible early signs of shock that must be immediately
recognized.
• Children maintain a near-normal blood pressure even in the face of
25% to 30% of blood volume loss. In these situations, subtle
changes in the HR and extremity perfusion may signal impending
cardiorespiratory failure.
18.
Circulation
• Obvious signsof shock such as
• hypotension
• decrease in urinary output
may not occur
until more than
30% of blood
volume has been
lost
19.
Circulation
ABC
• Make vascularaccess the next priority once adequate ABCs are
established.
• If possible, place 2 percutaneous IV catheters in the upper
extremities.
• If peripheral venous access cannot be obtained after 3
attempts or in
< 90 seconds, establish IO access in children <6 years.
• A saphenous vein cutdown and cannulation of central veins are other
options, but these techniques should be reserved for stable
patients and skilled personnel.
21.
Circulation
• Initial fluidresuscitation- warm isotonic crystalloid solution (RL
or isotonic NS solution) at a bolus of 20
mL/kg.
• The goals of the initial resuscitation should be to achieve
hemodynamic normality and to restore adequate tissue perfusion as
soon as possible.
• Children with evidence of hemorrhagic shock who fail to response to
fluid resuscitation should also receive blood (10 mL/kg) and be
evaluated by a pediatric surgeon for possible operative
intervention.
22.
Disability
ABCD
• Causes ofdecreased level of consciousness in injured children include
traumatic brain injury (TBI), hypoxemia, and poor cerebral
perfusion.
• Assess Neurologic status
• [AVPU] system
• pediatric Glasgow Coma Scale [GCS]- describes level of consciousness in TBI,
categorize head injury
Environment and Exposure
ABCDE
•larger body surface area to body mass ratio predisposes them to larger
heat and insensible fluid loss than adults, resulting in higher fluid and
caloric requirements.
• Avoid accidental hypothermia during the initial phase of resuscitation.
• Hypothermia results in vasoconstriction, low-flow state, acidosis, and
consumptive coagulopathy.
• To prevent hypothermia:
use warm intravenous fluids.
Once the patient is exposed, cover the patient with a warm blanket.
Connective air rewarmers and warmed, humidified ventilation can help maintain
core body temperature if hypothermia is detected (< 35°C/95°F).
Peritoneal lavage with warm saline
Extracorporeal circulatory rewarming- for patients with severe
hypothermia (< 28°C/82°F) in association with ventricular fibrillation or arrest or
with drowning in cold water.
Pain control
• Oncethe primary survey has been completed, address the issue of
pain control.
• Pain relief can be provided with morphine (0.1 mg/kg) or a
combination of fentanyl (1 mcg/kg) and midazolam (0.5-0.1 mg/kg).
• Definitive treatment can be accomplished safely once hypoxia,
tachycardia, hypotension, and hypothermia have been managed.
The secondary survey involves a more detailed systemic evaluation and
initiation of diagnostic studies.
27.
Adjuncts to PrimarySurvey
• Access: IV vs. IO
• Monitor: Cardiorespiratory/Pulse oximetry.
• Bloodwork - CBC, electrolytes, ABG, creatinine, BUN, PT/PTT,
crossmatch, LFT, lipase or amylase, BHCG if female of child-
bearing age
28.
Imaging Prior toSecondary Survey
• Chest X rays: (AP only) , Pelvis (AP only) , C-spine: lateral,
AP
• FAST- Focused assessment with sonography in trauma
29.
Secondary evaluation
• Completehistory taking
• Head to toe physical examination
• Neurological- LOC, Pupils, GCS
• Head, neck , spine
• Chest
• Abdomen
• Orifices, Rectum
• Musculoskeletal
• Reassessment of vital signs
30.
Secondary
survey
1. Head trauma
Management:
• Airway
• Cardiovascular and circulatory status
• Intracranial pressure and cerebral perfusion
• Bleeding, Seizures
• Temperature
• Analgesia, sedation, and neuromuscular blockade
Surgery: Surgical intervention in pediatric patients with head trauma may be required and includes
the following:
• Surgical decompression, Craniotomy and surgical drainage
• Surgical debridement and evacuation, Decompressive craniotomy with duraplasty
32.
2. Chest Injuries
•Children have relatively elastic ribs, that fracture rarely, despite that lungs
contusion is common without ribs fracture.
• Major thoracic injuries may coexist despite normal radiographic findings
like
1) Tension pneumothorax 2) Massive Haemothorax 3) Cardiac Tamponade
• In all cases airway should be secured, O2 is given and hypovolemia is
corrected
with IV – fluid. Diaphragmatic rupture after blunt abdominal trauma can
be
detected by chest x-ray or CT-scan, surgical repair is undertaken once the
pt
become stable
• Tension Pneumothorax: Tension pneumothorax requires prompt
clinical diagnosis
and immediate needle thoracocentesis. Site- 2nd ICS , “midclavicular
line”.
Thoracocentesis is followed by chest tube drainage.
• Massive Haemothorax: it is treated by chest tube drainage via “fifth
35.
3. Abdominal Trauma
►Bluntabdominal trauma is generally more common than
penetrating injury.
►In children more vulnerable organs are liver and spleen because they
are not protected by pliable rib cage.
Fluid resuscitation - 20 ml/kg of RL as bolus, may repeat 1-2 times.
Investigations used In Abdominal Trauma
►The definitive radiological investigation of major abdominal trauma
in haemodynamically stable child is CT – scan with IV – contrast.
►Expert ultrasound scanning is readily available it can demonstrate
free abdominal fluid and solid organ injuries but it is not valuable as CT
►Exp. Laparotomy is indicated for bowel perforation and
penetrating trauma.
36.
4. Burn/Thermal Injury
Management:
• ABCDE
• Consider early intubation if airway involvement
• Tetanus prophylaxis and ANALGESIA
• Fluid resuscitation mainstay of treatment
• Parkland Resuscitation Formula: using Ringer’s Lactate, Give 4ml/kg/%TBSA
• First half of resuscitation fluids (AS WELL AS MAINTENANCE FLUIDS) over
first 8 hours and Second half over following 16 hours
• Urine output goal: 1-2 ml/kg/hour
37.
Prevention of pediatrictrauma
• Supervision of children during play
• Commitment by healthcare workers to the pediatric trauma
population.
• Public education regarding automobile safety, firearm safety, and
burn prevention
• Pediatric life-support courses for providers of care
• Legislation regarding establishment and enforcement of seat belt
laws, increased enforcement of drunk driving statutes, firearm
registration, establishment of trauma registry.
38.
Preventing falls
• Evaluatingmental status, Call light within reach
• Environment clear of hazards and unused equipment
• Orientation to the room
• Bed in low position with brakes on
• Side rails raised as necessary based on the child’s age and cognition
• Nonskid footwear and appropriate-size clothing
• Child and family education
• Checks of the child at least every hour
• Accompaniment of the child during ambulation
• Assessment of the need for 1:1 supervision
Summary
• Experiences withaccidents, injuries, physical abuse, or
hospitalization can leave a lasting impact on
children's minds. Thus psychosocial support .
• ABCDE
• Age appropriate assessment, equipment, and
dosing




















![Disability
ABCD
• Causes of decreased level of consciousness in injured children include
traumatic brain injury (TBI), hypoxemia, and poor cerebral
perfusion.
• Assess Neurologic status
• [AVPU] system
• pediatric Glasgow Coma Scale [GCS]- describes level of consciousness in TBI,
categorize head injury](https://image.slidesharecdn.com/pediatrictrauma-190211082818-250921211727-f0b1105a/75/pediatrictrauma-in-children-190211082818-pptx-22-2048.jpg)


































































