
Recommended
Recommended
More Related Content
Similar to Educational & Child Psychology; Vol. 36 No. 3 33Evaluating.docx
Similar to Educational & Child Psychology; Vol. 36 No. 3 33Evaluating.docx (20)
More from gidmanmary
More from gidmanmary (20)
Recently uploaded
Recently uploaded (20)
Educational & Child Psychology; Vol. 36 No. 3 33Evaluating.docx
- 1. Educational & Child Psychology; Vol. 36 No. 3 33 Evaluating the impact of an autogenic training relaxation intervention on levels of anxiety amongst adolescents in school Tracey Atkins & Ben Hayes Aim: This study aimed to investigate the impact of a group- based autogenic training (AT) relaxation intervention on levels of anxiety in adolescents in mainstream school settings. Method: A mixed-methods design was used to measure differences in levels of anxiety and explore a range of perceived changes between groups over time. Sixty-six young people aged between 14 and 15 years old from four mainstream schools in the UK were randomly assigned within each school to an intervention or wait-list control group. Quantitative data were analysed using a mixed between-within subjects ANOVA. Qualitative information from 12 volunteer participants was analysed using thematic analysis. Findings: Results showed a main effect of time for both the intervention group and the wait-list group however, no significant main interaction was found. Qualitative results showed perceived improvements in social relationships and connectivity; reflectiveness; self- awareness; physiological symptoms; and a sense of control. Limitations: Measures were reliant on self-reported data. Schools were recruited through self-referral and expression of interest, excluding participants who may not have
- 2. the opportunity to take part. There were no opportunities to collect follow-up data. Conclusions: Results suggest that a structured AT relaxation intervention delivered in a familiar school environment may significantly reduce levels of anxiety amongst adolescents. However, significant improvements for the wait-list group also raises questions around the potential of other supportive variables, such as acknowledgement and validation of feelings, the promise and availability of forthcoming support and the potential impact of raised awareness and interest in pupil wellbeing amongst school staff. Keywords: autogenic training; relaxation; adolescence; mind- body interventions; anxiety. M ENTAL HEALTH difficulties in young people are a serious cause for concern across the world. The World Health Organization (WHO) reports that in half of all cases of mental health conditions, onset has occurred by the age of 14 years old; suicide is the third leading cause of death in 15–19 year olds; and the second leading cause of death in girls (WHO, 2018). It is estimated that one in ten children and young people aged 5–16 years old have a diagnosable mental health disorder in the UK alone; and at least one in 12 children and young people deliberately self-harm (Young Minds, 2018). In 2009, the UK government identi- fied mental health as everyone’s business
- 3. (Department of Health; DoH, 2009) and was specific about prevention and the tran- sition time between adolescence and early adulthood. Suggestions for schools include promoting students’ mental health as part of their curriculum (Department for Educa- tion; DfE, 2016), highlighting the desire of young people themselves to be more involved with the development, delivery and evalu- ation of interventions (National Institute of Health and Clinical Excellence; NICE, 2014); making use of group work to teach specific skills and empower young people; 34 Educational & Child Psychology; Vol. 36 No. 3 Tracey Atkins & Ben Hayes and identifying the expertise and role of educational psychologists (EPs) (Weare & Gray, 2003). The mental health of the nation was viewed by the Prime Minister as one of the ‘greatest social challenges of our time’ (Gov.uk, 2017). A government green paper now aims to transform services by training new mental health workers including educa- tional mental health practitioners to work in schools and in collaboration with NHS professionals (DoH & DfE, 2017) Adolescence and brain development Adolescence is recognised as a period of social and psychological change and neuro- biological development that can either
- 4. enhance vulnerability or provide a window of opportunity for growth and learning (Dahl et al., 2018). Research into cognitive and affective development in adolescence shows that on the one hand cognitive development appears to progress regardless of pubertal changes (Dahl, 2004), but on the other, although development during this period takes place in regions of the brain associated with regulation of behaviour and emotion and the evaluation of risk and reward, these are impeded by increases in arousal, moti- vation and sensation seeking behaviour. Consequently, while there are advances in reasoning and decision-making skills, and the ability to comprehend the consequences of impulsivity, these can be easily over-ridden not only by a natural propensity to experi- ence intense feelings but also a keen desire to seek these intense feelings out, occasion- ally at a serious or fatal cost (Dahl, 2004). Adolescence and Mental Health Adolescents are particularly at risk of expe- riencing emotional distress as their brains mature (Blakemore & Frith, 2011). It is a period of life where many experience their first episode of mental health difficulties (Kessler et al., 2005). Literature suggests an increase in stress hormones compared to adults (Romeo, 2009) and a clear asso- ciation between exposure to chronic stress and significant changes in emotion and cognition, such as anxiety and depression (Romeo, 2017). Sensitivity to the effects of
- 5. stress also inhibits typical brain development and maturation (Sinclair et al., 2014). The impact of exposure to stress is associated with risk-taking and aggression (Byrne & Mazanov, 2002) but despite the cognitive capabilities to do so (Dahl, 2004) adoles- cents are less able to apply effective problem solving strategies to cope (Llorca et al., 2017). Changes in social acceptance, negative rela- tionships, experience of bullying, and fear of peer rejection are all strong predictors of anxiety disorders (Carr, 2002; Horwitz et al., 2011; Morris & Kratochwill, 1991; Roza et al., 2003), and yet adolescents are far less likely than other young people with psychiatric disorders to be in contact with supportive services or receive any treatment (Chavira et al., 2004; Neil & Christensen, 2009). Relaxation interventions in schools Relaxation training in its many forms can be used exclusively as an intervention or in conjunction with other cognitive or psychotherapeutic programmes (Ashton, 2015). Purposeful muscle-relaxation and controlled breathing techniques have been used to treat a range of psychological prob- lems (Kobayashi-Suzuki et al., 2014) and educational stress (Manjushyambika et al., 2017). Progressive muscle relaxation (PMR) has been found to raise self-esteem, particu- larly amongst females with moderate levels of depression (Larson et al., 2014; Reyn- olds & Coats, 1986); reduce aggression, and improve levels of aspiration, vitality, mental health and social functioning (Nickel et
- 6. al., 2005). Interventions such as mindful- ness and autogenic training (AT) have had a positive impact on quality of sleep (Bootzin & Stevens, 2005), attention skills (Jha et al., 2007), emotional regulation (Metz et al., 2013), and self-reported wellbeing (Sanger et al., 2018). More recently, findings for meditation in schools have been linked to improvements in coping skills, social rela- tionships and eating disorders (Wisner et al., 2010). Educational & Child Psychology; Vol. 36 No. 3 35 Evaluating the impact of an autogenic training relaxation intervention Autogenic training (AT) Based on research into sleep and hypnosis, AT was developed as a relaxation technique by Schultz and Luthe in 1959. AT focuses on an observant and passive attitude towards one’s own cognitive, emotional and phys- ical state, and through a series of taught exercises over a period of five to ten weeks, a deep state of relaxation can be achieved. Once learned, AT can be used regularly without the need for any external human or material support. It is considered to be one of a range of mind–body interventions recognised by the American Psychological Association (APA; Kotecki et al., 2014), and consistent with interventions recommended to treat anxiety disorders (Carr, 2002),
- 7. such as ‘self-instructional training focusing on control and competence’ and ‘relaxation skills’ (pp.199). Research into the effects of AT shows reductions in anxiety amongst adults (Ernst & Kanji, 2000; Garvin et al., 2001; Manzoni et al., 2008) and improvements in externalising emotional and behavioural presentation (Goldbeck & Schmidt, 2003) amongst young people. However, there is a distinct gap in the literature for AT from an educational perspective. Previous research has mainly focused on adults in health settings with small sample sizes and what research there is for young people lacks transparency. Given the similarities between AT and other relaxation-based interventions, it is surprising that there is no empirical evidence for the use of AT to address anxiety and wellbeing amongst young people in the UK. The role of the educational psychologist in delivering relaxation interventions There are professional and ethical reasons why EPs should be involved in the devel- opment and delivery of innovative inter- ventions to promote mental health in schools. Although still in its infancy, the evidence base for mind–body relaxation interventions is growing and the concept is now widely recommended to address the psychological wellbeing of young people and their educators (Kotecki et al., 2014;
- 8. Weare, 2015). Interventions vary dramat- ically in content and it is not clear which particular elements of programme design distinctively contribute to its overall effec- tiveness (Khoury et al., 2013). However, EPs are uniquely placed to apply psycho- logical research and theory and deliver evidence-based programmes to support young people experiencing emotional problems in school (Macleod et al., 2015; Perfect & Morris, 2011). In the light of government concerns (DfE, 2016; Weare, 2015) this includes personal health and wellbeing as well as academic achievement (Cameron, 2006; Rydzkowski et al., 2015). Many EPs want to engage in more high quality casework (Boyle & Lauchlan, 2009) and are open to expanding their reper- toire of skills to include more therapeutic approaches (Jimerson & Oakland, 2007). EPs are also increasingly supporting others to provide direct support with supervision, guidance and advice at a whole school level. These skills can help to fill the gaps in outreach services and contribute to work typically offered by other agencies (Truong & Ellam, 2014). It is recommended that EPs work along- side resident pastoral support staff providing direct interventions or supervision, espe- cially where a more targeted and individual approach is necessary (Weare, 2015). In such cases, EPs provide a service that follows strict ethical guidelines and draws on the principles of competence, responsibility and integrity.
- 9. They continuously further their professional development and expertise, apply knowledge of the advantages and limitations of different types of interventions, especially in terms of universal availability and potential harm, and recognise the proper protocols for consent, privacy and information sharing. In addi- tion, their awareness of group dynamics and therapeutic alliance can greatly enhance the outcomes of an intervention whether they train others or take part directly with young people (MacKay, 2007). 36 Educational & Child Psychology; Vol. 36 No. 3 Tracey Atkins & Ben Hayes The present study Given the potential for improving well- being through the delivery of a range of relaxation-based interventions in schools, this study aimed to investigate the impact of a group-based AT relaxation intervention on levels of anxiety amongst adolescents in schools, and to gather the perceptions about the intervention from the young people taking part. Method The study employed a partially mixed, concurrent, equal status mixed methods design (Leech & Onwuegbuzie, 2009). Quan- titative and qualitative data were collected independently of each other using nested
- 10. samples for the qualitative components of the study. Data were then analysed separately before drawing the two strands together for integration at the overall interpretation stage at the end of the study (Creswell & Plano Clark, 2011). Sample sizes Using ‘G*Power’, an average effect size of d = 0.68 (Cohen, 1998) chosen from research reflecting the use of AT with as close a sample population as possible to the present study (Stetter & Kupper, 2002) and a proposed alpha level of 0.05 was used to calculate a sample size of between 56 (one-tailed) and 70 (two-tailed) participants in order for the study to provide a statistical power in excess of 80 per cent. Quantitative and qualitative measures Pre and post quantitative information was gathered using the Spence Children’s Anxiety Scale (SCAS; Spence, 1997). This self-report measure is widely used around the world for both clinical and community purposes. Forty-four items are rated on a four-point Likert scale ranging from 0 = Never to 3 = Always. Example questions include ‘I worry about things’ and ‘I can’t seem to get bad or silly thoughts out of my head’. Table 1: Phases of thematic analysis (Braun & Clarke, 2006) Phase Description of the process 1. Familiarising yourself with your data The data was
- 11. transcribed by the researcher and re-read three times. Initial notes were made at this time. 2. Generating initial codes Interesting features of the data were coded in a systematic fashion across the entire data set again by summarising quotes and extracts for meaning. 3. Searching for themes Codes were then collated and linked together into potential themes. 4. Reviewing themes Themes were then checked for congruence with phases 1 and 2 to generate a ‘thematic map’. 5. Defining and naming themes Data was then revisited again to refine themes and generate clear definitions and titles. At this point, coded transcripts and definitions were viewed and analysed by a peer before being discussed for inter-rater reliability. 6. Producing the report The researcher then selected the most vivid, compelling extract examples to illustrate an overall picture of the results. Educational & Child Psychology; Vol. 36 No. 3 37 Evaluating the impact of an autogenic training relaxation intervention
- 12. Table 2: Semi-structured interview schedule Questions Rationale 1. What has the AT group meant to you? (Don’t be afraid to say negatives as well as positives…) Open question to prompt initial thoughts about their experience of AT. 2. Have you noticed any changes in yourself – or not? Open question for recipient to explore what they perceive to be ‘changes’. 3. What was it like for you? Open question for recipient to think about emotional responses to the intervention. 4. Was it what you expected it to be? Direct question to prompt for differences in initial perceptions of the intervention and for participants to compare what they actually experienced. 5. Is it something you are likely to keep practising or not? Direct question with prompt for responding either way: ‘or not?’ Designed to assess the extent to which the intervention has been incorporated into lifestyles.
- 13. 6. What will you remember the most about learning AT? Open question to prompt further understanding of experiences relating to AT. 7. Is there anything else you would like to say about your experience of AT? Open question to give further opportunity to express thoughts in case previous questions have not included information. Sub-scales include obsessive compulsive disorder, separation anxiety, social phobia, panic agoraphobia, physical injury fears and generalised anxiety. Cronbach’s alpha for the total SCAS score was reported consist- ently between 0.90 and 0.92; and between 0.54 to 0.83 for the six subscales (Muris et al., 2000, 2002; Spence, 1997; Spence et al., 2003). Post-intervention qualitative informa- tion was gathered by three participants from each school (total n = 12). Each participant was interviewed on an individual basis for up to 15 minutes a session. Responses were then analysed using the thematic analysis procedure (Braun & Clarke, 2006) outlined in Table 1. Sampling methods and procedure For the quantitative phase of the study and for practical and geographical reasons, conven- ience sampling (Onwuegbuzie & Collins, 2007) was initially used, whereby schools
- 14. in an area of the South East of England were approached to express interest. Identifying a specific geographical area counteracted some of the issues around matching groups from different schools within a large local authority – although it was recognised that generalisability across a wider population would be limited. Once schools were iden- tified, volunteer sampling was employed to recruit individuals from each school who were then provided with written information about AT from the British Autogenic Society (BAS) and consent forms to complete. After completing the SCAS pre-measure question- naire individuals were randomised to either the intervention or wait-list group. At the post intervention stage, individual semi-structured interviews with three participants from each mainstream setting were held approximately one week after post-intervention quantita- tive data collection. The interview schedule is outlined in Table 2. 38 Educational & Child Psychology; Vol. 36 No. 3 Tracey Atkins & Ben Hayes Table 3: Summary of participant and school characteristics School 1 School 2 School 3 School 4 I W I W I W I W
- 15. N = 11 10 7 6 7 5 10 10 Gender Male 1 5 3 10 10 Female 10 10 7 6 2 2 Mean age 15.0 15.8 15.0 14.8 15.0 15.0 15.3 14.7 Ethnicity White British 11 9 7 6 6 5 10 9 Irish 1 White other 1 Kurdish 1 SEN C&L 2 2 1 1 2 1 SEMH 3 C&I 1 1 Sensory impairment 1 Physical disability 1 Socio-economic status Type of school Community Grammar Grammar Grammar
- 16. Gender Mixed Girls Mixed Boys Ethnic minorities > national average < national average < national average < national average SEN < national average < national average < national average < national average FSM > national average < national average < national average < national
- 17. average I = Intervention group; W = Waitlist group; C&L = Cognition and learning; SEMH = Social emotional and mental health; C&I = Communication and interaction; SEN = Special educational needs; FSM = Free school meals. Educational & Child Psychology; Vol. 36 No. 3 39 Evaluating the impact of an autogenic training relaxation intervention Participants Sixty-six adolescents aged 14 and 15 years old took part in the study. An independent samples t-test was used to assess possible differences in anxiety scores (SCAS) between intervention and wait-list groups at the pre-intervention assessment stage. No signif- icant between-group differences were found however, initial scores for the SCAS prior to the intervention showed that the mean score for males fell within the average range of anxiety level (M = 29.4, SD = 14.94); and the mean score for females within the elevated range of anxiety level (M = 43.41, SD = 17.77). Further details on participant characteristics are outlined in Table 3. Intervention details The AT intervention consisted of six weekly sessions lasting approximately 30 minutes
- 18. each. Each session followed the same struc- ture as outlined in Table 4. Examples of the AT exercises included encouraging a seated position with eyes closed, followed by auto-suggestions of heaviness and warmth to isolated parts of the body. The participants repeated formulas in their minds such as: ‘My arms and legs are heavy and warm’, ‘My neck and shoulders are heavy’, ‘My forehead is cool and clear’. A new exercise formula was taught each week which built on the previous one, to eventually achieve physio- logical and psychological feelings of relax- ation through classical conditioning. This technique is intended to be self-sufficient and transferable across contexts so that no props or additional resources are needed. Each session was delivered by the same qual- ified autogenic therapist (the first author) and a manualised programme of training was delivered to all groups meaning that direct replication was possible (Wolery, 2011). Results Quantitative analysis Scores for the SCAS were analysed using a mixed between-within subjects analysis of variance (ANOVA). Output showed no signif- icant interaction between group and time, Wilk’s l = 0.96, F(1, 64) = 2.87, p = 0.095, partial h2 = 0.04. There was a significant main effect for time, Wilk’s l = 0.64, F(1, 64) = 36, p < 0.0005, partial h2 = 0.36, suggesting that anxiety scores for both groups did change between pre and post-intervention time points
- 19. (see Table 5). The main effect comparing groups was not significant, F(1, 64) = 0.41, p = 0.52, partial h2 = 0.006, suggesting no differ- Table 4: Structure of AT sessions Activity 1 Participants were asked for feedback on how the exercise practice from the previous session had gone, along with the opportunity for further questions and clarification. Keeping a diary was encouraged but was for the participants’ own reflection and reference. 2 The old exercise was practiced once again, feedback was sought, and questions answered. 3 The new exercise for the week was introduced. The researcher provided the rationale along with modelling and psychoeducational information. 4 The new exercise was practiced together. 5 Participants were asked for feedback on their experience. 6 Additional short exercises were introduced and explained but not practiced. 7 The researcher talked through the home practice and information was provided in the form of a hand-out. 8 Home practice was recommended 3 times a day, every day.
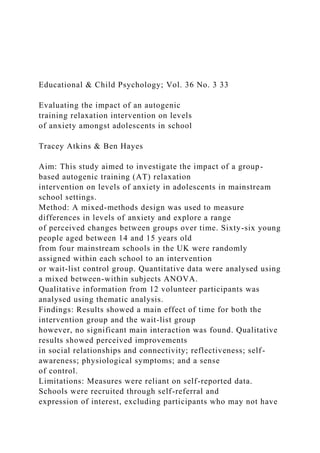
- 20. 40 Educational & Child Psychology; Vol. 36 No. 3 Tracey Atkins & Ben Hayes ence in the effectiveness of the intervention compared to the wait-list control group (see Table 6). Given the differences between male and female anxiety levels before the interven- tion, an additional ANOVA was run with sex as an additional between subjects factor with no interaction found for sex. Qualitative analysis Transcripts of qualitative information were checked for accuracy by the researcher and a peer before thematic analysis and interpretation began. Inter-rater reliability percentage agreement scores were estab- lished at 93 per cent and were calculated by dividing the number of times a code was identified and agreed by both coders by the number of times it was possible for a code to occur (Boyatzis, 1998). The thematic map (Figure 1) highlights five over-arching themes and contributing sub-themes that indicate the perceived changes that took place as a result of the AT intervention. Relationships A number of participants made reference to changes in the way they thought about and related to others. Sub-themes included better friendships, increased feeling of connectivity to others, a desire to share their new knowledge, and the benefits of group
- 21. participation. One participant said she had ‘definitely’ noticed changes in her friend- ships. She felt that her feelings about herself had prompted her to think differently about her friends’ intentions and that her mood had impacted positively on the reciprocity and quality of her friendships. Others commented on the sessions being a bonding experience where everyone had been on a journey learning together; and for someone who had ‘suffered from anxiety for a while’, he noticed an increase in his ability to join in with activities he previously found difficult. Many participants revealed an ability to think of others besides themselves, demon- strating a desire to help them, and not be ‘bothered by the tiny things any more’. One young man with an autism spectrum condition commented that it was easier to learn in a group as it took the focus away from him and gave him more freedom to engage. Emotional awareness and control Participants also reported changes in emotional reactivity and emotional aware- ness. Three participants talked about how they usually reacted aggressively towards pressure. They were more able to take a step back in the face of antagonism in class and social situations, or simply to ignore it.
- 22. Table 5: SCAS anxiety scores for intervention and wait-list groups across pre and post time points Intervention group Wait-list group Time period N M SD N M SD Time 1 35.00 39.22 17.10 31.00 34.58 18.65 Time 2 35.00 30.45 16.91 31.00 29.70 18.64 Table 6: SCAS anxiety scores for intervention compared to wait-list group using mixed between-within ANOVA F value Sig. Effect size Main effect of time F (1,64) = 36 p < 0.0005 hρ² = 0.36 Main effect of group F (1,64) = .41 p = 0.52 hρ² = 0.006 Interaction F (1,64) = 2.87 p = 0.095 hρ² = 0.04 Educational & Child Psychology; Vol. 36 No. 3 41 Evaluating the impact of an autogenic training relaxation intervention Others talked about how the scheduled time in the week was something they looked forward to as a ‘relief’ or ‘break’ from the stress of school inferring that AT exercises were a sort of respite from a frantic world and a ‘break from reality’.
- 23. Physical change Many participants reported an improvement in the somatic symptoms of stress, such as less panic attacks in crowded corridors or attacks that were less intense than before. Less head- aches and increased energy also increase pro-activity and motivation for activities: ‘more up for the (like) lessons…’ There were numerous comments about being able to fall asleep quicker and, once asleep, sleep better feeling more motivated in the morning, along with noticing a reduction in aching muscles, sports injuries and quicker recuper- ation after glandular fever. Increased self-awareness Some participants felt their new knowledge of how the body works had helped them to understand the principles behind the exer- cises and how they could play an important part in maintaining wellbeing. Sub-themes reflected feelings of increased control and self-confidence through recognising the warning signs that they were becoming stressed, what form their state of stress took, increased understanding of what was happening to the body, and experiencing feelings that they could now cope. Participants reported increased self- confidence in a variety of ways, talking about their ability to let go of small things that used to occupy their minds and hold them back. They implied that a certain trust and confi-
- 24. dence in the future had also grown enabling them to get on with life and live in the moment. Some talked of having the confi- dence to express how they were feeling to others more, relieving the burden of worry and without feeling self-conscious. One participant felt that the process of alleviating her anxiety started from the very first time she brought the introductory letter home to her parents. There was a sense of empowerment and an ability to make choices and decisions about which exercise to use and how this could be fitted into their practice. AT was recognised as a self-help skill that was prac- tical, versatile and portable, and a tool for people to take responsibility for themselves. Cognitive change Participants found that they could concen- trate better and this had been helpful in school, even to the point that one partic- ipant had noticed that she was sitting up straighter in lessons. She felt that this small Figure 1: Thematic analysis map 42 Educational & Child Psychology; Vol. 36 No. 3 Tracey Atkins & Ben Hayes Table 7: Overarching themes and examples of dialogue
- 25. Overarching Theme Sub-theme Examples of dialogue Relationships Better friendships I think that my friendships have got better… Yeah, I just been a lot happier and better… Um – I feel my friendships have got, become a lot nicer to me but I think they’ve always been nice to me but before I was just curious so maybe she wasn’t sitting next to me because of that or she’s not doing that but now I’ve just become (pause) and opened up and just been aware of just (pause) my friendships and become a lot less stressed – haven’t broken down in a while. …it’s more to do with for me it’s like socialising I find quite difficult I’ve just been able to… I’ve been more easy-going with other people as well… so – that’s been interesting. Recognising difficulties in others I just see the world in a more positive light now… Yeah I just, I just, like I would always feel judged or like as if everything going around me was about like someone was doing it to me. If someone was like sad, I would think, ‘Oh gosh, I’ve done something to them…’. But now I don’t view it as me I just view it as them. I really like that – and I think everyone around me likes that. Increase in bonding and connectivity …it’s kind of… we have done the whole journey... we’ve all been able to help each other, I think it’s been quite
- 26. good to connect us individually as well and not just develop our own things… Group participation Normally I wouldn’t have wanted to leave my parents at all. Other trips that I have done, I have not wanted to leave my parents so I won’t have eaten anything. I wouldn’t have really done much either but with this I got stuck in and did everything. There was less pressure on me specifically and that made it significantly easier to understand. Desire to share and help others It was fun, it was good, it was like, I thought it would be rubbish but it was actually really really good – I told my mum and my mum done it… Yeah, I’ll show them cos I think some of my friends, they get really stressed and if I just read it out to them they can get calm. ...it’s definitely helped me to relay my feelings to other people… uh, kind of with the being able to express how I’m feeling. I’ve actually started writing a blog. Emotional awareness and control Slower emotional reactions
- 27. If somebody upsets me or anything I can move away from them and use the meditation and stuff to calm myself down before going back to like speak with people… Normally, something violent may have happened. Educational & Child Psychology; Vol. 36 No. 3 43 Evaluating the impact of an autogenic training relaxation intervention Feelings of safety and reassurance Coming in on Mondays was kind of like a safe, a safe kind of like a retreat, so I’m quite visual so I usually think, um, this is a line between being anxious and not being anxious… and then my day consists of, you know, going out of the zone at different lengths and then it’s kind of like a retreat back, it’s like a reassurance, a um yeah it’s kind of like a safe zone for me. Physical change Reduced somatic symptoms of stress …I don’t really dream as vividly any more so it’s kind of like helping me to actually sleep and not, and not like waste all that energy you like imagine you would do… I think I feel more like it sounds really like what can I say, I feel like I can get up like I can do things. …it would have been longer to get better because
- 28. obviously the more you worry the more stressed you get and the ‘iller’ you get so it’s definitely, it’s definitely been helpful for my health especially so… I just get so tired during the day, usually, and it’s quite good to, it kind of like reboots yourself – if that makes sense? Increased self-awareness Psycho-educational understanding …it just helps – it helps, you can feel it in the muscles in the shoulders and your arms it’s kind of – being more relaxed afterwards. …I’m using it even if I’m not stressed cos it’s kind of like in a roof – you don’t get rid of the drainpipes when it’s not raining you know, you keep those as a safeguard so like a sort of a maintenance thing, a maintenance of wellbeing. …I often think I’m like choking on air and then I think, like Oh!… and then I’ll get panicked about that and that I can’t breathe and yeah then it all kind of snowballs… it’s a lot more relaxed. If I’m (in) somewhere that’s like crowded and I do feel claustrophobic and I’m kind – like step back and can free myself and actually take time to breathe. Empowerment I liked that instead of like having to rely on someone else to help us – it was like you telling us how we could help ourselves.
- 29. Well actually, as I’ve got an injury at the moment and like when it’s really hurting I sit there and I think about other parts of the body and then it doesn’t hurt… cos I do sport quite a lot I always get like aches and pains and its quite good to use to relax muscles then… yeah yeah because whenever I come out I feel like I’m floating (laughs). 44 Educational & Child Psychology; Vol. 36 No. 3 Tracey Atkins & Ben Hayes Confidence …and I’m much more calm and relaxed and I feel that this has given me a positive effect in lessons because I can concentrate more rather than think – oh my gosh, I’ve got to remember this and then I’ve got to do this, and then I’ve got to do this… and it just builds up and now I’m just cool about it. Because before, like before I was doing it I didn’t really tell anyone how I was feeling… a lot of the time I feel quite queezy and a lot of butterflies in my stomach all the time and then when I brought home the letter like Oh Yeah! I’m doing a relaxing thing I was able to tell my mum that I was feeling like that… yeah and it’s definitely helped me to be able to relay my feelings to other people. Cognitive change Improved concentration …cos I think all over the place way like a very busy kind of mind map but, um, maybe autogenics helps
- 30. to kind of take a few moments to help my brain just to put things in order so it’s more kind of like a linear process… Increase in positive thinking I just see the world in a better more positive light now… before when I did tests I usually get all worried about and then like on the way home oh I’m all worried… but when I was walking home I thought I’m not nervous about this so, and then um I’m going to do well so I find out today, but I think I’m not thinking all the negative stuff – just the positive stuff. Clarity of thought So it’s just easier to get through um I think it’s, it’s changed the way I kind of think about things quite a lot, cos I used to, like when things happen and you just can’t really do anything about it you just got like, you know you just have to like worry about it but now I just, I’m more like I just let things happen and I can just… well you can only control what you can control I think that’s what I’ve learned. Increased problem solving skills Um I think it’s just because I am able to like really think about it and then I just kind of realise that it is just not that important. Increased self-monitoring Well, I know that this autogenics is supposed to relax
- 31. you and everything yeah, you done those sheets to take home and try to practice – I can’t find a time cos I’ve got loads of work to do at home, it’s really stressful … Yeah, I managed a bit but too stressful at time… I just concentrated a bit more that’s all… I realise how good my work is so… I’ve concentrated more before I done autogenics but… Educational & Child Psychology; Vol. 36 No. 3 45 Evaluating the impact of an autogenic training relaxation intervention change was also helping her to engage more in class. Participants reported more clarity, noticing that less stress meant that work seemed to be easier to do. Many started to notice that they were thinking differently and seeing life more positively and from other perspectives, with some specifically commenting on how they were now more able to discern what they could reasonably take responsibility for and what they could not, putting everyday situa- tions into perspective. Two participants were able to re-evaluate situations in terms of how significant they were in the grand scheme of things. For instance, one felt more relaxed about exams, firstly because he was secure in the
- 32. knowledge that he could relax himself, but also because he had done his revision and reasoned that if this was so, there was no need to get stressed. On the other hand, one male participant reported that he continued to feel stressed throughout the programme and that this had prevented him from finding the time to practice the exercises at home. Some examples of participant responses can be found in Table 7. Discussion Although there was a main effect of time for both groups, no significant main interaction effect was found between time and group, indicating that the AT intervention was no more effective in reducing overall anxiety levels in adolescents compared to the wait-list group. While the results are promising, there is no way to rule out that there may have been other factors that supported partici- pants with their anxiety in both groups, aside from the intervention. Interestingly, similar results were found in studies by Garvin et al. (2001) and Goldbeck and Schmidt (2003) for AT; and for other school-based early intervention programmes for anxiety (Neil & Christensen, 2009). One explanation may be that both the wait-list group and the intervention group experienced a Hawthorne effect (Barker et
- 33. al., 2012), whereby the research itself height- ened expectancy to produce beneficial changes. Reactivity of measurement effects (Barker et al., 2012) have been known to produce psychological benefits. The qualitative results suggest that this part of the research was just as impor- tant as the intervention itself in providing an opportunity to share and talk about feel- ings. They also revealed that the information and consent letter provided one participant with the opportunity to talk about her anxiety to her family and to discover that she was not alone. Psychological coherence can be understood as the experience of emotional comfort when views of the self are matched or validated (Wright et al., 2014). The bene- fits of identifying with a group and feelings of belonging and commonality are also docu- mented by Sani et al. (2015). This may have been the case for the wait-list groups since there was no way of knowing whether their opportunities to express their feelings or mix within a supportive group had increased. Equally, participation in the research may have raised awareness amongst school staff. Schools who had opted into the study indicated that they recognised pupil anxiety which could have made them more predis- posed to provide a nurturing environment, especially to those who they knew were waiting for their intervention. Previous research find- ings show that increased teacher interest in the emotional wellbeing of students is highly
- 34. valued and improves subjective wellbeing (Suldo et al., 2009) as well as the importance of increased school identification as a predictor of better mental health outcomes (Miller et al., 2018) and the benefits of talking to an attuned adult who can offer unconditional positive regard (Reichardt, 2016). Qualitative analysis from the study indi- cates perceived changes in some participants in a range of physiological and psychological areas. Participants perceived an increased ability to take a step back from situations with less emotional reaction to provocation, better connectivity and analytic thought into other people’s social behaviour and 46 Educational & Child Psychology; Vol. 36 No. 3 Tracey Atkins & Ben Hayes needs, and improvements in self-monitoring and planning behaviours. Participants also reported not only a reduction in somatic symptoms but also a faster recovery rate from illness, better sleep, and an increase in moti- vation to look after one’s health overall. Such reports reflect current attention towards a wider perspective on what it means to be mentally healthy with the importance of sleep and practical relaxation techniques specifi- cally highlighted in the government’s advice for mental health and behaviour in schools (DfE, 2016, pp.13). Results also comply with
- 35. the findings of Llorca et al. (2017), who recommend that besides the acquisition of coping skills, all adolescent anxiety inter- ventions or preventative programmes should include specific teaching in the development of emotional self-regulation and the recogni- tion and acceptance of feelings. This study adds to the evidence avail- able about AT and addresses a gap in the research field for the adolescent population in UK mainstream schools. Despite no main interaction effect, the perceived impact of the intervention seen in the qualitative data is promising. Furthermore, the study provides illuminating information from the wait-list groups, who also showed significant reductions in anxiety levels, and may have opened a door for further research and investigation to take place. Limitations Several factors were found to account for potential limitations of the study. It must be recognised that representation of the population was compromised as some of the data from one of the schools were not normally distributed at the outset. Demo- graphic details also showed a lack of cultural diversity, and although ethical reasons dictated sampling strategy, convenience and volunteer bias meant that it would be impos- sible to be able to infer generalisability of the sample (Cohen et al., 2013). The type of participants who volunteer may not be representative of the target population for
- 36. a number of reasons. They may be more likely to engage with adult initiated activity, be more motivated to take part in projects such as research studies or their own motives may clash with those of the researcher (Borg & Gall, 1989). Similarly, those who did not come forward for involvement may have done so to avoid criticism and stigmatisation, but equally be in need of support (Cohen et al, 2013, Kaushik et al., 2016). There was also a lack of information on other supporting strategies and interventions that may have been provided at the same time as the intervention group. In schools where a commitment to developing the social and emotional wellbeing of young people is woven into the curriculum, it is likely that these strat- egies will also have a positive effect on devel- opment (Fabiano et al., 2014). Future studies or replications would benefit from including detailed information on concurrent types of support for wellbeing in each school, espe- cially where school settings differ. Although randomisation was intended to minimise as many confounding variables as possible, and maximise equivalency, the possibility that information and strategies were leaked between members of the inter- vention group to members of the wait-list group within each educational setting prior to post-intervention data collection cannot be ruled out. Similarly, the absence of qualitative information sought from the wait-list group
- 37. makes it difficult to attribute effects to AT. Another limitation of the study was that only one self-report questionnaire was used to measure overall anxiety levels, which poses a question over the validity of the data (Barker, et. al., 2012). Future research could include the use of other measures from other sources (such as parents and teachers). Qualitative results suggesting perceived improvements in social skills, relationships, and ability to cope, also highlight the poten- tial usefulness of additional measures in the future such as the Strengths and Difficulties Questionnaire, Beck Youth Inventories, and Resiliency Scales, as well as non-standardised rating scales to measure personal and specific anxiety provoking situations. Educational & Child Psychology; Vol. 36 No. 3 47 Evaluating the impact of an autogenic training relaxation intervention Implications for practice The current study contributes to a better understanding of researcher effects, aware- ness raising and the impact that interven- tions such as AT in schools might have. This study specifically explored an EP- facilitated, group-based relaxation interven- tion within a school setting. School-based interventions have the advantage of bringing
- 38. mental health support directly to the young people at school, avoiding common barriers such as costs and transport to attend alter- native settings (Swan et al., 2014). They provide greater consistency, reliability, and adherence to programme protocols (Langley et. al., 2010) and may provide the oppor- tunity to alleviate anxiety levels in the very places where learning is taking place. Since there may be no evidence for any significant difference between delivering interventions to groups or individuals (Flannery-Schroeder et al, 2005), it is suggested that group-based interventions could increase the reach for mental health and wellbeing in schools (Weare & Gray, 2003). The study was only able to provide the interviewed sub-sample (n = 12) with the opportunity to talk about their expe- riences. Many of the comments indicated that the debriefing process was an impor- tant element of intervention delivery and an opportunity to gather pupil voice and pupil collaboration. Future delivery of the inter- vention could include discussions with all group members to set goals and suggest ways forward, not only to meet their individual needs but to implement change at a systemic level. Forman et al. (2009) suggest fitting programmes seamlessly into school settings by considering the curriculum, teaching styles, school ethos and resources available, and nurturing strong and ongoing relation- ships. Involving pupils in decision-making around how their mental health will be
- 39. promoted is vital at secondary school level where teachers find it more difficult to iden- tify internalised symptoms (Auger, 2004). The findings that many participants found the psychoeducation aspect of the intervention helpful is also something for EPs to consider. Participants felt this had a positive effect on their ability to recognise the early warning signs of stress and feel in control of their anxiety. It would, there- fore, be useful for EPs to raise awareness of the key changes that take place in adolescent brain development amongst all adolescents to promote adaptive behaviours that reduce risk and increase positive outcomes for youth (Dahl, 2004). The qualitative results indicate other aspects of the intervention that might be supportive. Valuable elements were felt by participants to be working in a group, acknowledging anxiety, and sharing and expressing feelings within a supportive environment. Self-compassion has been found to be a protective factor in rela- tion to mental health issues (Marshall et al., 2015), and the acknowledgement and acceptance of symptoms to be facilitators of increased perceived control (Arch & Craske, 2008). Young people experiencing problems with anxiety and depression may be reluctant to request help due to concern about burdening others or the stigma they may face (Kaushik et. al., 2016). Further
- 40. research could investigate the impact of researcher effects in relation to anxiety in particular, considering what might facilitate change in young people whether they are part of an intervention or not. EPs could also consider working with schools with this wider set of factors in mind. Possible mech- anisms could include developing supportive environments where there are safe areas to talk, opportunities to bond and connect with like-minded others, and increasing positive supportive relationships between peers and peers, peers and members of staff, and members of staff themselves. Authors Dr Tracey Atkins, Educational Psychologist, East Sussex; [email protected] Dr Ben Hayes, Senior Educational Psycholo- gist, Kent & Associate Professor, University College London 48 Educational & Child Psychology; Vol. 36 No. 3 Tracey Atkins & Ben Hayes References Arch, J.J. & Craske, M.G. (2008). Acceptance and commitment therapy and cognitive behavioral therapy for anxiety disorders: Different treat- ments, similar mechanisms? Clinical Psychology: Science and Practice, 15(4), 263–279.
- 41. Ashton, R. (2015). Relaxation as an intervention to improve emotional and behavioural outcomes for children. Open Journal of Educational Psychology, 1, 1–17. Auger, R.W. (2004). The accuracy of teacher reports in the identification of middle school students with depressive symptomatology. Psychology in the Schools, 41(3), 379–389. Barker, C., Pistrang, N. & Elliott, R. (2012). Research methods in clinical psychology: An introduction for students and practitioners. Ohio: John Wiley & Sons. Blakemore, S.J. & Frith, U. (2011). The learning brain: Lessons for education. Oxford: Blackwell Publishing. Bootzin, R.R. & Stevens, S.J. (2005). Adolescents, substance abuse, and the treatment of insomnia and daytime sleepiness. Clinical Psychology Review, 25(5), 629–644. Borg, W.B. & Gall, M.D. (1989). Educational research: An introduction (5th edn). New York: Longman. Boyatzis, R.E. (1998). Transforming qualitative infor- mation: Thematic analysis and code development. London: Sage. Boyle, C. & Lauchlan, F. (2009). Applied psychology and the case for individual casework: Some reflections on the role of the educational psychologist. Educational Psychology in Practice, 25(1), 71–84.
- 42. Braun, V. & Clarke, V. (2006) Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. Byrne, D.G. & Mazanov, J. (2002). Sources of stress in Australian adolescents: Factor structure and stability over time. Stress and Health: Journal of the International Society for the Investigation of Stress, 18(4), 185–192. Cameron, R.J. (2006). Educational psychology: The distinctive contribution. Educational Psychology in Practice, 22(4), 289–304. Carr, A. (2002). What works with children and adoles- cents?: A critical review of psychological interventions with children, adolescents and their families. Hove: Routledge. Chavira, D.A., Stein, M.B., Bailey, K. & Stein, M.T. (2004). Child anxiety in primary care: preva- lent but untreated. Depression and Anxiety, 20(4), 155–164. Cohen, J. (1988). Statistical power analysis for the behav- ioural sciences (2nd edn). New Jersey: Lawrence Erlbaum. Cohen, L., Manion, L. & Morrison, K. (2013). Research methods in education. Oxon: Routledge. Creswell, J.W. & Plano Clark, V.L.P. (2011). Designing and conducting mixed methods research. California: Sage.
- 43. Dahl, R.E. (2004). Adolescent brain development: A period of vulnerabilities and opportunities. Keynote address. Annals of the New York Academy of Sciences, 1021, 1–22. Dahl, R.E., Allen, N.B., Wilbrecht, L. & Suleiman, A.B. (2018). Importance of investing in adoles- cence from a developmental science perspective. Nature, 554(7693), 441. Department for Education (2016). Mental health and behav- iour in schools. Retrieved 4 November 2018 from www. gov.uk/government/uploads/system/uploads/ attachment_data/file/508847/Mental_Health _and_Behaviour_-_advice_for_Schools_160316.pdf Department for Education, Department of Health and Social Care, The Charity Commission, Prime Minister’s Office, 10 Downing Street & The Rt Hon Theresa May MP (2017). The shared society. Prime Minister’s speech at the Charity Commission annual meeting, 9 January 2017. Retrieved 5 November 2018 from www.gov.uk/government/speeches/ t h e - s h a r e d - s o c i e t y - p r i m e - m i n i s t e r s - s p e e c h - a t - t h e - c h a r i t y - c o m m i s s i o n - a n n u a l - meeting Department for Education (2016). Mental health and behaviour in schools: Departmental advice for school staff. Retrieved 8 November 2018 from www.gov.uk/government/uploads/system/ uploads/attachment_data/file/508847 Department of Health (2009). New Horizons: Towards a shared vision for mental health – consultation.
- 44. Retrieved 8 November 2018 from http://webar- chive.nationalarchives.gov.uk/20130107105354/ h t t p : / / w w w. d h . g o v. u k / p r o d _ c o n s u m _ d h / groups/dh_digitalassets/documents/digital- asset/dh_103175.pdf Department of Health & Department for Educa- tion (2017). Transforming children and young people’s mental health provision: A green paper. Retrieved 5 November 2018 from https:// assets.publishing.service.gov.uk/government/ uploads/system/uploads/attachment_data/ file/664855/Transforming_children_and_ young_people_s_mental_health_provision.pdf Ernst, E. & Kanji,N.(2000). AT for stress and anxiety: A systematic review. Complementary Therapies in Medicine, 8(2), 106–110. Fabiano,G.A., Chafouleas, S.M., Weist, M.D.,Sum- i,W.C. & Humphrey, N.(2014). Methodology considerations in school mental health research. School Mental Health, 6(2), 68–83. Flannery-Schroeder, E., Choudhury, M.S. & Kendall, P.C. (2005). Group and individual cognitive-behavioral treatments for youth with anxiety disorders: 1-year follow-up. Cognitive Therapy and Research, 29(2), 253–259. Educational & Child Psychology; Vol. 36 No. 3 49 Forman, S.G., Olin, S.S., Hoagwood, K.E., Crowe, M. & Saka, N. (2009). Evidence-based interventions
- 45. in schools: Developers’ views of implementation barriers and facilitators. School Mental Health, 1(1), 26. Garvin, A.W., Trine, M.R. & Morgan, W.P. (2001). Affective and metabolic responses to hypno- sis,autogenic relaxation and quiet rest in the supine and seated positions. International Journal of Clinical and Experimental Hypnosis, 49(1), 5–18. Goldbeck,L. & Schmid,K.(2003). Effectiveness of autogenic relaxation training on children and adolescents with behavioral and emotional prob- lems. Journal of the American Academy of Child & Adolescent Psychiatry, 42(9), 1046–1054. Horwitz, A.G., Hill, R.M. & King, C.A. (2011). Specific coping behaviors in relation to adoles- cent depression and suicidal ideation. Journal of Adolescence, 34(5), 1077–1085. Jha, A.P., Krompinger, J. & Baime, M.J. (2007).Mind- fulness training modifies subsystems of attention. Cognitive, Affective, & Behavioral Neuroscience, 7(2), 109–119. Jimerson, S.R. & Oakland, T.D. (2007). School psychology internationally: A retrospective view and influential conditions. In S.R. Jimerson, T.D. Oakland & P.T. Farrell (Eds.) The Handbook of International School Psychology (pp.453–462). Cali- fornia: Sage. Kaushik, A., Kostaki, E. & Kyriakopoulos, M. (2016). The stigma of mental illness in children and adolescents: A systematic review. Psychiatry
- 46. Research, 243, 469–494. Kessler, R.C., Berglund, P., Demler, O., Jin, R., Meri- kangas, K.R. & Walters, E.E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602. Khoury, B., Lecomte, T., Fortin, G. et al. (2013). Mindfulness-based therapy: A comprehensive meta-analysis. Clinical Psychology Review, 33(6), 763–771. Kobayashi-Suzuki, E. ,Tachibana, Y. ,Okuyama, M. & Igarashi, T. (2014). Breathing focused mind-body approach for treatment of posttraumatic stress disorder among children and adolescents: a systematic review. Journal of Psychology Psycho- therapy, 4(3), 2161–0487. Kotecki, J., Khubchandani, J., Simmons, R. & Sharma, M. (2014). Mind–body interventions applications and potential opportunities for health education practice. Health Promotion Practice,16(2),157–161. Langley, A.K., Nadeem, E., Kataoka, S.H., Stein, B.D. & Jaycox, L.H. (2010). Evidence-based mental health programs in schools: Barriers and facilita- tors of successful implementation. School Mental Health, 2(3), 105–113. Larson, H.A., Kim, S.Y., McKinney, R. et al. (2014). This is just a test: Overcoming high-stakes test anxiety through relaxation and gum chewing when preparing for the ACT. Eastern Education
- 47. Journal, 42. Leech, N.L. & Onwuegbuzie, A.J. (2009). A typology of mixed methods research designs. Quality & Quantity, 43(2), 265–275. Llorca, A., Malonda, E. & Samper, P. (2017). Anxiety in adolescence. Can we prevent it? Medicina Oral, Patologia Oral y Cirugia Bucal, 22(1), e70. MacKay, T.A.W.N. (2007). Educational psychology: The fall and rise of therapy. Educational and Child Psychology, 24(1), 7. Macleod, S., Sharp, C., Bernardinelli, D., Skipp, A. & Higgins,S. (2015). Supporting the attainment of disadvantaged pupils: Articulating success and good practice: Research report November 2015 (No. DFE-RR411,pp.DFE-RR411). London: Depart- ment for Education. Manjushambika, R., Prasanna, B., Vijayaraghavan, R. & Sushama,B.(2017). Effectiveness of Jacob- son’s progressive muscle relaxation (JPMR) on educational stress among school going adoles- cents. International Journal of Nursing Education, 9(4), 110–115. Manzoni, G.M., Pagnini, F., Castelnuovo, G. & Moli- nari, E. (2008). Relaxation training for anxiety: A ten-years systematic review with meta-analysis. Bio Med Central Psychiatry, 8(41), 1–12. Marshall, S.L., Parker, P.D., Ciarrochi, J. et al. (2015). Self-compassion protects against the negative effects of low self-esteem: A longitudinal study
- 48. in a large adolescent sample. Personality and Indi- vidual Differences, 74, 116–121. Metz, S.M., Frank, J.L., Reibel, D., Cantrell, T., Sanders, R. & Broderick, P.C. (2013).The effec- tiveness of the learning to BREATHE program on adolescent emotion regulation. Research in Human Development, 10(3),252–272. Miller, K., Wakefield, J. & Sani, F. (2018). Identifi- cation with the school predicts better mental health amongst high school students over time. Educational and Child Psychology, 35(2), 21–29. Morris, R.J. & Kratochwill, T.R. (1991). Fears and phobias. The Practice of Child Therapy, 76–114. Muris, P., Merckelbach, H., Ollendick, T. et al. (2002). Three traditional and three new child- hood anxiety questionnaires: Their reliability and validity in a normal adolescent sample. Behaviour Research and Therapy, 40(7), 753–772. Muris, P., Schmidt, H. & Merckelbach, H. (2000). Correlations among two self-report question- naires for measuring DSM-defined anxiety disorder symptoms in children: The Screen for Child Anxiety Related Emotional Disorders and the Spence Children’s Anxiety Scale. Personality and Individual Differences, 28(2), 333–346. Evaluating the impact of an autogenic training relaxation intervention
- 49. 50 Educational & Child Psychology; Vol. 36 No. 3 Tracey Atkins & Ben Hayes Neil, A.L. & Christensen, H. (2009). Efficacy and effectiveness of school-based prevention and early intervention programs for anxiety. Clinical Psychology Review, 29(3), 208–215. National Institute for Health and Clinical Excellence (2014). Social and emotional wellbeing for children and young people over- view. Retrieved 8 November 2018 from http://pathways.nice.org.uk/pathways/social-an d-emotional-wellbeing-for-children-and-young- people Nickel, C., Lahmann, C., Tritt,K. et al. (2005). Short communication: Stressed aggressive adolescents benefit from progressive muscle relaxation: A random,prospective, controlled trial. Stress and Health: Journal of the International Society for the Investigation of Stress, 21, 169–175. Onwuegbuzie, A.J. & Collins, K.M. (2007). A typology of mixed methods sampling designs in social science research. The Qualitative Report, 12(2), 281–316. Perfect, M.M. & Morris, R.J. (2011). Delivering school? Based mental health services by school psychologists: Education, training, and ethical issues. Psychology in the Schools, 48(10), 1049–1063. Reichardt, J. (2016). Exploring school experiences of young people who have self-harmed: How can
- 50. schools help. Educational and Child Psychology, 33(4),28–29. Reynolds, W.M. & Coats, K.I. (1986). A comparison of cognitive-behavioral therapy and relaxa- tion training for the treatment of depression in adolescents. Journal of Consulting and Clinical Psychology, 54(5), 653. Romeo, R.D. (2009). Adolescence: A central event in shaping stress reactivity. Developmental psychobi- ology, 52(3), 244–253. Romeo, R. (2017). The impact of stress on the structure of the adolescent brain: implications for adolescent mental health. Brain Research, 1654, 185–191. Roza, S.J., Hofstra, M.B., van der Ende, J. & Verhulst, F.C. (2003). Stable prediction of mood and anxiety disorders based on behavioral and emotional problems in childhood: A 14-year follow-up during childhood, adolescence, and young adulthood. American Journal of Psychiatry, 160(12), 2116–2121. Rydzkowski, W., Canale, N. & Reynolds, L.(2016). A review of interventions for adolescents with insomnia and the role of the educational and child psychologist: when sleep does not come easily. Educational Psychology in Practice, 32(1), 24–37. Sanger, K.L., Thierry, G. & Dorjee ,D. (2018). Effects of school? Based mindfulness training on emotion processing and well? Being in adoles- cents: Evidence from event?related potentials.
- 51. Developmental Science, e12646. Sani, F., Madhok, V., Norbury, M., Dugard,P. & Wakefield, J.R. (2015). Greater number of group identifications is associated with healthier behaviour: Evidence from a Scottish community sample. British Journal of Health Psychology, 20(3), 466–481. Schultz, J.H. & Luthe,W.(1959). Autogenic training: A psychophysiologic approach to psychotherapy.New York: Grune & Stratton. Sinclair, D., Purves-Tyson, T.D., Allen, K.M. & Weickert, C.S. (2014). Impacts of stress and sex hormones on dopamine neurotransmission in the adolescent brain. Psychopharmacology, 231(8), 1581–1599. Spence, S.H. (1997). The Spence Children’s Anxiety Scale (SCAS). In I. Sclare (Ed.) Child Psychology Portfolio. Windsor: NFER-Nelson. Spence, S.H., Barrett, P.M. & Turner,C.M. (2003). Psychometric properties of the Spence Children’s Anxeity Scale with young adolescents. Journal of Anxiety Disorders, 17, 605–625. Stetter, F. & Kupper, S. (2002). AT: A meta-analysis of clinical outcome studies. Applied Psychophysiology and Biofeedback, 27(1). Suldo, S.M., Friedrich, A.A., White, T., Farmer, J., Minch, D. & Michalowski, J. (2009). Teacher support and adolescents’ subjective wellbeing:
- 52. A mixed-methods investigation. School Psychology Review, 38(1), 67. Swan, A.J., Cummings, C.M., Caporino, N.E. & Kendall, P.C. (2014). Evidence-based inter- vention approaches for students with anxiety and related disorders. In H.M. Walker & F.M. Gresham (Eds.) Handbook of evidence-based prac- tices for emotional and behavioural disorders: Applica- tions in schools. New York: Guildford. Truong, Y. & Ellam, H. (2014). Educational psychology workforce survey 2013. https://dera.ioe.ac.uk/ 19840 Weare,K. (2015). What works in promoting social and emotional wellbeing and responding to mental health problems in schools? Retrieved 6 November 2018 from www.mentalhealth.org.nz/assets/ ResourceFinder/What-works-in-promoting-social- and-emotional-wellbeing-in-schools-2015.pdf Weare, K. & Gray, G. (2003). What works in devel- oping children’s emotional and social competence and wellbeing? London: Department for Education and Skills. Retrieved 6 November 2018 from http://learning.gov.wales/docs/learningwales/ publications/121129emotionalandsocialcompe- tenceen.pdf Wisner, B.L., Jones, B. & Gwin, D. (2010). School-based meditation practices for adolescents: A resource for strengthening self-regulation,emotional coping,and self-esteem. Children & Schools, 32(3), 150–159.
- 53. Educational & Child Psychology; Vol. 36 No. 3 51 The psychology within models of reading comprehension Wolery, M. (2011). Intervention research: The importance of fidelity measurement. Topics in Early Childhood Special Education, 31(3), 155–157. World Health Organization (2018). Adolescent mental health. Retrieved 1 November 2018 from www.who.int/mental_health/maternal-child/ adolescent/en Wright, K.B., King, S. & Rosenberg, J. (2014). Func- tions of social support and self-verification in association with loneliness,depression, and stress. Journal of Health Communication, 19(1), 82–99. Young Minds (2018). Mental health statis- tics.Retrieved 1 November 2018 from www.youngminds.org.uk/about-us/media-centre/ mental-health-stats Copyright of Educational & Child Psychology is the property of British Psychological Society and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.
- 54. Executive Summary Guidelines with Scoring Rubric Purpose The purposes of this assignment are to: a) identify and articulate the results of a Magnet report received from the American Nurses Credentialing Center (ANCC) for Saint Louis Medical Center (SLMC). You, the nurse director, will present your findings to the SLMC board of directors, in an executive summary format (CO 2, 3), b) articulate and include the key components of an executive summary in your report (CO 5), and c) provide empirical, scholarly evidence to support your assignment (CO 4). NOTE: As the nurse executive of SLMC, you may choose one item from any of the following Magnet Model Components to discuss and present to the SLMC board of directors, in your executive summary. There is no written report of a Magnet Survey; you have the flexibility to choose what you would like to discuss in this assignment. For example, you may state in your report that your Magnet model component is structural empowerment and you wish to implement a new nurse model since the results of your Magnet report were not acceptable in this area. Magnet Model Components: Transformational Leadership Structural Empowerment Exemplary Professional Practice New Knowledge, Innovations & Improvements Empirical Outcomes Due Date: Sunday 11:59 p.m. MT at the end of Week 7 Total Points Possible: 225Requirements: 1. This paper will be graded on quality of paper information, use of citations, use of Standard English grammar, sentence structure, and organization based on the required components. 2. Create this assignment using Microsoft (MS) Word, which is
- 55. the required format for all Chamberlain documents. You can tell that the document is saved as a MS Word document because it will end in “.docx”. 3. Submit to the appropriate assignment area by 11:59 p.m. MT on Sunday of the week due. Any questions about this paper may be discussed in the weekly Q & A Discussion topic. 4. The length of the paper is to be no greater than three (3) pages, excluding title page and reference page. 5. APA format using the sixth edition manual is required in this assignment, including a title page and reference page. Use APA level 1 headings for the organizational structure of this assignment. Remember that the introduction does not carry a heading that labels it as a level heading in APA format. The first part of your paper is assumed to be the introduction. See the APA manual sixth edition for details. Use the suggested format and headings to organize your assignment: a. Include introduction (do not label as a heading in APA format) b. Issue and Magnet Model Component Identified c. Key Components of Executive Summary d. Supporting Evidence e. ConclusionPreparing the paper Note: Please use the resources in your Roussel textbook, Chapter 15, to assist with how to write an executive summary format to articulate the results of your Magnet report from ANCC. 1. Clearly introduce your executive summary in the introduction paragraph. Include a sentence that states the purpose of your assignment. 2. Clearly identify and articulate the issue and component from the Magnet model to be communicated to the board of directors at SLMC by you, the nurse executive. Discuss how your choice may affect your healthcare environment and transform healthcare. 3. Key components of an executive summary format, related to the results of the Magnet report, should be included and clearly
- 56. articulated. (Examples are in your textbook or you may search for them on the web). Include in your executive summary how this assignment relates to the Person-centred Framework by McCormack and McCance (2017). 4. Include of a minimum of three sources of scholarly, empirical evidence to support the issue to be communicated. 5. Provide concluding statements that should summarize your overall assignment content. 6. The paper will be no longer than three pages maximum, excluding title and reference page(s). Note: There are several formats of an executive summary in your text or on the internet. As the nurse executive, you may choose which style you prefer. 7. Title and reference page(s) must be in APA format using the sixth edition manual. 8. Use 12 Times New Roman font and one-inch margins on all sides of the paper. 9. Note: After submitting your assignment to the Week 7 assignment area, please also upload your completed assignment to the Week 8 designated threaded discussion to share with your peers. Category Points % Description Introduction 30 13% Introduction clearly introduces your executive summary and purpose of the assignment. Issue and Magnet Model Component 30 13% Issue and component from the Magnet model to be
- 57. communicated to board of directors is identified and clearly articulated. Key Components 80 38% The key components of the executive summary are included and clearly articulated. Evidence 30 13% Minimum of three scholarly, empirical evidence sources to support issue. Conclusion 30 13% Concluding statements summarizing content are present. Text, title page, and references are consistent with APA format 10 4% Text, title page, and references are consistent with APA format. Ideas and information from other sources are cited correctly 10 4% Ideas and information from other sources are cited correctly. Rules of grammar, word usage, and punctuation are followed 5 2% Rules of grammar, word usage, and punctuation are followed. Total 225 100 A quality assignment will meet or exceed all of the above requirements. Chamberlain College of Nursing NR531 Nursing Leadership in Healthcare Organizations
- 58. NR531 Guidelines with rubric.docx Revised 1 2019 3 Grading Rubric Assignment Criteria Exceptional (100%) Outstanding or highest level of performance Exceeds (88%) Very good or high level of performance Meets (80%) Competent or satisfactory level of performance Needs Improvement (38%) Poor or failing level of performance Developing (0) Unsatisfactory level of performance Content Possible Points = 200 Points Introduction 30 points 26 points 24 points 11 Points
- 59. 0 points Introduction introduces your executive summary and purpose clearly. Introduction introduces your executive summary with minor lack of clarity or elements. Introduction of executive summary lacks occasional important element or specificity. Introduction of executive summary has multiple instances of inaccuracies. Introduction of executive summary is not present. Issue and Magnet Model Component 30 points 26 points 24 points 11 Points 0 points Identification of issue and Magnet model component to be communicated to the board of directors is articulated clearly with no inaccuracy. Identification of issue and Magnet model component to be communicated to the board of directors is articulated with rare inaccuracy. Identification of issue and Magnet model component to be communicated to the board of directors lacks occasional important elements or specificity. Identification of issue and Magnet model component to be communicated to the board of directors has multiple instances of inaccuracies. Identification of issue and Magnet model component to be communicated to the board of directors is not present. Key Components 80 points
- 60. 70 points 66 points 30 points 0 points Key components of executive summary are included and clearly articulated Key components of executive summary are articulated with rare inaccuracy. Key components of executive summary lack occasional important element or specificity Key components of executive summary have multiple instances of inaccuracies. Key components of executive summary are not present. Evidence 30 points 26 points 24 points 11 Points 0 points At least three empirical, scholarly evidence sources supporting your issue are included. Empirical, scholarly evidence sources supporting your issue are clearly critiqued and have rare inaccuracy; or only two sources included. Empirical, scholarly evidence sources supporting your issue lack occasional important element or specificity; or less than two sources included. Empirical, scholarly evidence sources supporting your issue have multiple instances of inaccuracies. Empirical, scholarly evidence sources supporting your issue are not present. Conclusion 30 points 26 points
- 61. 24 points 11 Points 0 points Concluding statements summarizing content are present and accurate. Concluding statements summarizing content are present with rare inaccuracy or missing elements. Concluding statements summarizing content lack occasional important element or specificity. Concluding statements summarizing content has multiple instances of inaccuracies. Concluding statements summarizing content are missing. Content Subtotal _____ of 200 points Format Possible Points = 20 points Text, title page, and references are consistent with APA format. 10 points 9 points 8 points 4 points 0 points Text, title page, and references are consistent with APA format. Text, title page, and references are consistent with APA format, with two to four exceptions. There are five to seven APA format errors in the text, title page, and reference pages.
- 62. There are eight to nine APA format errors in the text, title page, and reference pages There are more than 10 APA format errors in the text, title page, and reference pages. Ideas and information from other sources are cited correctly. 10 points 9 points 8 points 4 points 0 points Ideas and information from other sources are cited correctly. Ideas and information from other sources are cited correctly, with two to four exceptions. Ideas and information from other sources are cited with five to seven errors. Ideas and information from other sources are cited with eight to nine errors. Ideas and information from other sources are cited with more than 10 errors. Grammar Possible Points = 5 points Rules of grammar, word usage, and punctuation are followed. 5 points 4 points 3 points 2 points 0 points Rules of grammar, word usage, and punctuation are followed. Rules of grammar, word usage, and punctuation are followed,
- 63. with two to four exceptions. Rules of grammar, spelling, word usage, and punctuation are consistent with formal written work, with five to seven exceptions. Rules of grammar, spelling, word usage, and punctuation are consistent with formal written work, with eight to nine exceptions. Rules of grammar, spelling, word usage, and punctuation are followed with more than 10 exceptions. Format Subtotal _____ of 25 points Total Points _____ of 225 points NR531 Guidelines with Rubric.docx 5 Week 7: Executive Summary Submit Assignment · Due Sunday by 11:59pm · Points 225 · Submitting a file upload NR531 W7 Executive Summary Guidelines and Rubric Purpose The purposes of this assignment are to: a) identify and articulate the results of a Magnet report received from the American Nurses Credentialing Center (ANCC) for Saint Louis Medical Center (SLMC). You, the nurse director, will present
- 64. your findings to the SLMC board of directors, in an executive summary format (CO 2, 3), b) articulate and include the key components of an executive summary in your report (CO 5), and c) provide empirical, scholarly evidence to support your assignment (CO 4). NOTE: As the nurse executive of SLMC, you may choose one item from any of the following Magnet Model Components to discuss and present to the SLMC board of directors, in your executive summary. There is no written report of a Magnet Survey; you have the flexibility to choose what you would like to discuss in this assignment. For example, you may state in your report that your Magnet model component is structural empowerment and you wish to implement a new nurse model since the results of your Magnet report were not acceptable in this area. Magnet Model Components: Transformational Leadership (Links to an external site.) Structural Empowerment (Links to an external site.) Exemplary Professional Practice (Links to an external site.) New Knowledge, Innovations & Improvements (Links to an external site.) Empirical Outcomes (Links to an external site.) Course Outcomes Through this assignment, the student will demonstrate the ability to: (CO2) Synthesize management and leadership theories with a caring, holistic, collaborative approach in preparation of nurse administrator roles: utilizing critical thinking, communication skills and therapeutic intervention strategies, of the professional role related to health outcomes. (PO2, 5). (CO3) Compare and contrast the effect of organizational structures, e.g. organizational charts, standards, resources, philosophy, procedures, and culture on work processes and organizational and patient outcomes; utilizing critical thinking, interprofessional collaboration, communication skills and
- 65. strategies of the professional role. (PO1, 2) (CO4) Apply the use of research in the evaluation of healthcare outcomes; utilizing critical thinking skills, and interprofessional research strategies. (PO4) (CO5) Examine effective verbal and written communication; utilizing communication skills of the professional role to promote and improve quality and safety in healthcare. (PO1, 2, 5) Due Date: Sunday 11:59 p.m. MT at the end of Week 7 Students are given the opportunity to request an extension on assignments for emergent situations. Supporting documentation must be submitted to the assigned faculty. If the student's request is not approved, the assignment is graded and a late penalty is applied as follows: · Monday = 10% of total possible point reduction · Tuesday = 20% of total possible point reduction · Wednesday = 30% of total possible point reduction If the student's request is approved, the student will be informed of the revised due date. Should the student fail to meet the revised due date, the assignment is graded and a late penalty is applied as follows: · Monday = 10% of total possible point reduction · Tuesday = 20% of total possible point reduction · Wednesday = 30% of total possible point reduction Total Points Possible: 225 Requirements: 1. This paper will be graded on quality of paper information, use of citations, use of Standard English grammar, sentence structure, and organization based on the required components. 2. Create this assignment using Microsoft (MS) Word, which is the required format for all Chamberlain documents. You can tell that the document is saved as a MS Word document because it will end in ".docx". 3. Submit to the appropriate assignment area by 11:59 p.m. MT on Sunday of the week due. Any questions about this paper may
- 66. be discussed in the weekly Q & A Discussion topic. 4. The length of the paper is to be no greater than three (3) pages, excluding title page and reference page. 5. APA format using the sixth edition manual is required in this assignment, including a title page and reference page. Use APA level 1 headings for the organizational structure of this assignment. Remember that the introduction does not carry a heading that labels it as a level heading in APA format. The first part of your paper is assumed to be the introduction. See the APA manual sixth edition for details. Use the suggested format and headings to organize your assignment: a. Include introduction (do not label as a heading in APA format) b. Issue and Magnet Model Component Identified c. Key Components of Executive Summary d. Supporting Evidence e. Conclusion Preparing the paper Note: Please use the resources in your Roussel textbook, Chapter 15, to assist with how to write an executive summary format to articulate the results of your Magnet report from ANCC. 1. Clearly introduce your executive summary in the introduction paragraph. Include a sentence that states the purpose of your assignment. 2. Clearly identify and articulate the issue and component from the Magnet model to be communicated to the board of directors at SLMC by you, the nurse executive. Discuss how your choice may affect your healthcare environment and transform healthcare. 3. Key components of an executive summary format, related to the results of the Magnet report, should be included and clearly articulated. (Examples are in your textbook or you may search for them on the web). Include in your executive summary how this assignment relates to the Person-centred Framework by McCormack and McCance (2017).
- 67. 4. Include of a minimum of three sources of scholarly, empirical evidence to support the issue to be communicated. 5. Provide concluding statements that should summarize your overall assignment content. 6. The paper will be no longer than three pages maximum, excluding title and reference page(s). Note: There are several formats of an executive summary in your text or on the internet. As the nurse executive, you may choose which style you prefer. 7. Title and reference page(s) must be in APA format using the sixth edition manual. 8. Use 12 Times New Roman font and one-inch margins on all sides of the paper. 9. Note: After submitting your assignment to the Week 7 assignment area, please also upload your completed assignment to the Week 8 designated threaded discussion to share with your peers. Anxiety and its disorders as risk factors for suicidal thoughts and behaviors: A meta-analytic review Kate H. Bentleya,*, Joseph C. Franklinb, Jessica D. Ribeirob,c, Evan M. Kleimanb, Kathryn R. Foxb, and Matthew K. Nockb aCenter for Anxiety and Related Disorders, Boston University, USA bDepartment of Psychology, Harvard University, USA cMilitary Suicide Research Consortium, USA Abstract
- 68. Suicidal thoughts and behaviors are highly prevalent public health problems with devastating consequences. There is an urgent need to improve our understanding of risk factors for suicide to identify effective intervention targets. The aim of this meta- analysis was to examine the magnitude and clinical utility of anxiety and its disorders as risk factors for suicide ideation, attempts, and deaths. We conducted a literature search through December 2014; of the 65 articles meeting our inclusion criteria, we extracted 180 cases in which an anxiety-specific variable was used to longitudinally predict a suicide-related outcome. Results indicated that anxiety is a statistically significant, yet weak, predictor of suicide ideation (OR=1.49, 95% CI: 1.18, 1.88) and attempts (OR=1.64, 95% CI: 1.47, 1.83), but not deaths (OR=1.01, 95% CI: 0.87, 1.18). The strongest associations were observed for PTSD. Estimates were reduced after accounting for publication bias, and diagnostic accuracy analyses indicated acceptable specificity but poor sensitivity. Overall, the extant literature suggests that anxiety and its disorders, at least when these
- 69. constructs are measured in isolation and as trait-like constructs, are relatively weak predictors of suicidal thoughts and behaviors over long follow-up periods. Implications for future research priorities are discussed. Keywords Suicide; Anxiety; Risk factor; Meta-analysis 1. Introduction Suicidal behavior is a leading cause of injury and death across the globe (Centers for Disease Control and Prevention, 2011), with upwards of one million individuals who take their own lives annually (World Health Organization, 2012). In the United States alone, over 40,000 people die by suicide each year. In addition to completed suicides, approximately 3% of individuals make a suicide attempt during their lifetime (Borges et al., 2010; Nock et al., *Corresponding author at: Center for Anxiety and Related Disorders, Boston University, 648 Beacon Street, 6th Floor, Boston, MA 02215, USA. [email protected] (K.H. Bentley). HHS Public Access
- 70. Author manuscript Clin Psychol Rev. Author manuscript; available in PMC 2016 February 29. Published in final edited form as: Clin Psychol Rev. 2016 February ; 43: 30–46. doi:10.1016/j.cpr.2015.11.008. A u th o r M a n u scrip t A u th o r M a n u scrip t A
- 71. u th o r M a n u scrip t A u th o r M a n u scrip t 2008). It is also estimated that approximately 9% of people report experiencing serious thoughts of suicide during their lives. Unfortunately, the U.S. suicide rate has risen steadily
- 72. over the past decade (Centers for Disease Control and Prevention, 2011) and is projected to continue increasing over upcoming years (Mathers & Loncar, 2006). One promising avenue toward reducing the global impact of suicide is to identify risk factors that predict suicidal thoughts and behaviors. Risk factors are not to be confused with correlates; whereas correlates represent concomitants or consequences of a phenomenon of interest and can be identified through cross-sectional methods, establishing risk factors necessitates longitudinal designs (Kraemer et al., 1997). For example, from a study showing that individuals who attempt suicide are more likely to be diagnosed with an anxiety disorder than those who do not attempt suicide, one may conclude that anxiety is a correlate of suicidal behavior. However, to determine that anxiety functions as a risk factor for suicidal behavior, it would need to be established that anxiety disorders precede and heighten future risk for suicide attempts. Establishing risk factors for suicidality is essential
- 73. for a number of reasons, including improved understanding of underlying mechanisms, identification of at-risk individuals, and development of evidence-based prevention and treatment programs. Most previous studies have focused exclusively on correlates, which are unlikely to be as informative for prediction and intervention purposes. Accordingly, the primary goal of this study was to conduct a meta-analytic review of prospective studies that have evaluated anxiety and its disorders as risk factors for suicidal thoughts and behaviors. In a narrative review, it can be difficult to provide a comprehensive account of all relevant studies, reconcile contradictory findings, account for methodological variations across the literature, and ascertain overall magnitudes of risk factors under investigation. A meta- analysis can overcome these limitations, and thus would be very helpful in summarizing current knowledge about anxiety as a risk factor for suicidality. There are several reasons why we chose to focus on anxiety in this meta-analysis. First, anxiety and its disorders are listed as important risk factors for
- 74. suicide by a number of national organizations (e.g., American Association of Suicidology, 2015; American Foundation for Suicide Prevention, 2015; National Suicide Prevention Lifeline, 2015). Determining the strength of empirical evidence to support this information, which is widely disseminated to clinicians, researchers, and the public, is necessary. Second, anxiety is implicated in many prominent theories of suicide. For example, according to Beck's cognitive model of suicide, once a suicide schema is activated, anxiety (and agitation) can serve as an expression of attentional fixation on suicide, which interacts with hopelessness to increase suicide risk (e.g., Wenzel & Beck, 2008; Wenzel, Brown, & Beck, in press). Although anxiety is not explicitly addressed in Joiner's interpersonal theory of suicide (Joiner, 2005; Van Orden et al., 2010), this model's emphasis on the fearsome nature of suicidal behavior is consistent with evidence showing that acute anxious states (e.g., heightened arousal/agitation, severe panic attacks) are often
- 75. present immediately prior to lethal or near-lethal suicidal acts (e.g., Britton, Ilgen, Rudd, & Conner, 2012; Busch, Fawcett, & Jacobs, 2003; Conrad et al., 2009; Fawcett et al., 1990; Hall, Platt, & Hall, 1999; Ribeiro et al., 2015; Ribeiro, Silva, & Joiner, 2014). These findings align with Fawcett's influential conceptualizations of anxiety/agitation as a determinant for acute suicide risk Bentley et al. Page 2 Clin Psychol Rev. Author manuscript; available in PMC 2016 February 29. A u th o r M a n u scrip t A u th
- 76. o r M a n u scrip t A u th o r M a n u scrip t A u th o r M a n u scrip
- 77. t (e.g., Fawcett, 2001; Fawcett, Busch, Jacobs, Kravitz, & Fogg, 1997), and expert clinical consensus identifying agitation as a “warning sign” for suicide (e.g., Rudd et al., 2006). Furthermore, Baumeister (1990) conceptualizes suicide as the ultimate escape from aversive self-awareness and associated negative affect, which often includes anxiety. Along similar lines, Riskind and colleagues have theorized that a specific cognitive risk factor for anxiety (looming vulnerability), when coupled with hopelessness, enhances urges to escape psychological pain and elevates risk for suicide (e.g., Rector, Kamkar, & Riskind, 2008; Riskind, 1997; Riskind, Long, Williams, & White, 2000). Third, anxiety and related disorders (broadly defined here as anxiety, obsessive–compulsive, trauma and stressor-related, and somatic symptom disorders) have received theoretical and empirical attention as potential risk factors for suicide. First and foremost, these disorders
- 78. are characterized by aversive, avoidant reactions to emotional experiences (Barlow, Sauer- Zavala, Carl, Bullis, & Ellard, 2014). Suicidal thoughts and behaviors have similarly been conceptualized as avoidant or escape-based responses to the experience of strong emotions (Baumeister, 1990; Boergers, Spirito, & Donaldson, 1998; Briere, Hodges, & Godbout, 2010; Bryan, Rudd, & Wertenberger, 2013; Shneidman, 1993), highlighting the potential functional similarities of these phenomena. Further, behavioral avoidance, a hallmark feature of anxiety disorders, often results in significant isolation, reduced quality of life, and impaired functioning (e.g., Massion, Warshaw, & Keller, 1993; Olatunji, Cisler, & Tolin, 2007), which confer additional risk to suicidality (Kanwar et al., 2013; Kaplan, McFarland, Huguet, & Newsom, 2007). Other avoidance strategies (e.g., suppression) often used by individuals with an anxiety disorder have also been shown to exacerbate vulnerability to suicidal thoughts and behaviors (Amir, Kaplan, Efroni, & Kotler, 1999).
- 79. In addition to promising theoretical relevance of anxiety disorders to suicidality, empirical investigations of this relationship generally show that anxiety disorders are independently associated with suicidal thoughts and behaviors. Although several earlier studies indicated that anxiety disorders are not related to suicidality (e.g., Hornig & McNally, 1995; Warshaw, Massion, Peterson, Pratt, & Keller, 1995), converging empirical evidence suggests that a broad range of anxiety and related disorders (including panic disorder, posttraumatic stress disorder [PTSD], social anxiety disorder, and generalized anxiety disorder [GAD]) function as statistically significant risk factors for suicidal thoughts and behaviors (Boden, Fergusson, & Horwood, 2007; Bolton et al., 2008; Borges, Angst, Nock, Ruscio, & Kessler, 2008; Gradus et al., 2010; Nepon, Belik, Bolton, & Sareen, 2010; Nock et al., in press, 2009, 2010a; Noyes, 1991; Sareen, 2011; Sareen et al., 2005; Thibodeau, Welch, Sareen, & Asmundson, 2013; Weissman, Klerman, Markowitz, & Ouellette, 1989;
- 80. Wilcox, Storr, & Breslau, 2009). For example, Nock and colleagues (2010a) observed that anxiety disorders significantly predicted future suicide attempts in a large, nationally representative sample (N = 9282), when controlling for psychiatric comorbidity. Indeed, anxiety disorders produced larger population attributable risk proportions (PARPs), which take into account the prevalence of predictors and distribution of comorbidity, for suicide ideation and attempts than impulse- control and substance use disorders. Among suicide ideators, anxiety disorders played a larger role than mood disorders, impulse-control disorders, and substance use disorders in Bentley et al. Page 3 Clin Psychol Rev. Author manuscript; available in PMC 2016 February 29. A u th o r M
- 82. u th o r M a n u scrip t accounting for subsequent suicide attempts. Findings from a cross-national study by Nock and colleagues (2009) are similar, with anxiety serving as a more powerful predictor of suicide attempts among ideators than mood, impulse-control, and substance use disorders. A recent meta-analysis of 42 studies further supports the notion that anxiety disorders and suicidal behavior are related (Kanwar et al., 2013); however, by including a combination of cross-sectional and longitudinal studies, the conclusions that can be drawn from this previous meta-analysis regarding anxiety (and specific disorders) as risk factors are
- 83. tempered. In summary, researchers, theorists, and clinicians have evidenced a longstanding interest in the role of anxiety and its disorders in suicide. A meta-analysis of longitudinal studies is necessary to synthesize the available literature on anxiety as a risk factor for suicidal thoughts and behaviors. Specifically, we aimed to: (1) estimate the predictive power (i.e., risk factor magnitude and accuracy) of anxiety as a risk factor for suicide-related outcomes, (2) compare the strength of effect sizes across types of anxiety (e.g., disorders, symptoms), and (3) examine potential moderators of the association between anxiety and suicide-related outcomes, including sample type, sample age, and length of follow-up period. To our knowledge, this represents the first effort to provide a comprehensive, quantitative review of the predictive ability of anxiety and its disorders for suicidal thoughts and behaviors. 2. Method This meta-analysis complies with the Preferred Reporting Items for Systematic Reviews and
- 84. Meta-Analyses statement (PRISMA; Moher, Liberati, Tetzlaff, & Altman, 2009). 2.1. Search strategy and selection We conducted a comprehensive literature search of PsycINFO, PubMed, and Google Scholar from database inception through December 2014 to identify studies eligible for the current review. The prediction-related terms longitudinal, longitudinally, predicts, prediction, prospective, prospectively, future, later, and follow- up were entered simultaneously with the self-injury-related terms self-injury, suicidality, self-harm, suicide, suicidal behavior, suicide attempt, suicide death, suicide plan, suicide thoughts, suicide ideation, suicide gesture, suicide threat, self-mutilation, self- cutting, cutting, self-burning, self-poisoning, deliberate self-harm, DSH, nonsuicidal self- injury, and NSSI. Given the inconsistent and ambiguous terminology used to describe self- injury (with or without suicidal intent) in the literature (Nock, 2010), we employed a wide range of self-injury-
- 85. related terms to reduce the likelihood of missing relevant studies. The reference sections of identified articles were also searched for other relevant publications. Fig. 1 presents a PRISMA diagram of the study selection process. A total of 2385 unique publications were identified by initial literature searches; after reviewing each abstract, 642 studies were deemed eligible for further review. The authors then reviewed each full-text study and identified 65 publications that met criteria for inclusion in the meta-analysis (see Appendix A for references for articles included in meta- analyses). Bentley et al. Page 4 Clin Psychol Rev. Author manuscript; available in PMC 2016 February 29. A u th o r M a n u
- 87. o r M a n u scrip t 2.2. Inclusion and exclusion criteria To be included in this meta-analysis, studies had to first include a longitudinal analysis predicting one or more of the following suicide-related outcomes: suicide ideation, suicide plan, suicide gesture, suicide attempt, or suicide death. Correspondingly, we excluded studies with outcomes that included nonsuicidal self-injury (NSSI) only. We also excluded studies that lumped nonsuicidal and suicidal behavior together into a single outcome (e.g., “deliberate self-harm”) because including these combined variables would render it difficult to draw strong conclusions about the association between anxiety and suicidal outcomes specifically. Second, included studies had to use one or more of
- 88. the following anxiety- specific predictors: any individual anxiety diagnosis (i.e., agoraphobia, anxiety disorder not otherwise specified, GAD, panic disorder, social anxiety disorder, specific phobia) or anxiety diagnosis grouping (e.g., “any anxiety disorder” as defined by study authors), any obsessive–compulsive or related disorder (e.g., OCD), any trauma or stressor-related disorder (e.g., adjustment disorder, PTSD), any somatic symptom disorder, symptoms of anxiety (diagnosis-specific and general; e.g., scores on self- report and clinician-rated measures such as the Beck Anxiety Inventory [BAI; Beck, Epstein, Brown, & Steer, 1988], Hamilton Anxiety Rating Scale [HARS; Hamilton, 1959], or Yale-Brown Obsessive Compulsive Scale [Y-BOCS; Goodman et al., 1989], panic attacks). Correspondingly, we excluded studies only examining constructs or symptoms broadly related but not specific to anxiety (e.g., neuroticism, negative affect, emotion dysregulation). We also excluded studies combining anxiety and mood disorders into a single variable
- 89. (e.g., internalizing problems, “mood or anxiety diagnosis”) because including these overlapping predictors would undermine our conclusions regarding the specific effect of anxiety on suicidal thoughts and behaviors. Finally, studies had to provide sufficient statistical information to conduct the present analyses, appear in a publication, and present original data not already reported in another study. 2.3. Data abstraction Authors systematically extracted relevant information from each article included in the present meta-analysis using a predefined coding strategy. Recorded information included: (a) year of study publication, (b) sample age (i.e., adult, adolescent, mixed), (c) sample size, (d) sample type (i.e., general, clinical, or history of prior SITBs), (e) length of study follow- up (in months), (f) statistical information for each unique prediction case (i.e., any instance using an anxiety-specific variable to longitudinally predict a suicide-related outcome), and