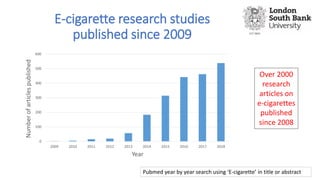
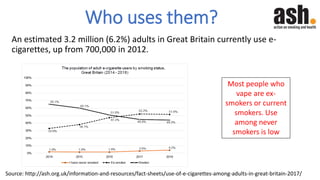
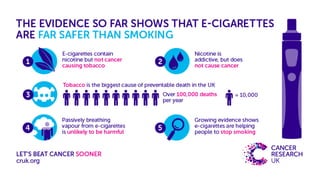
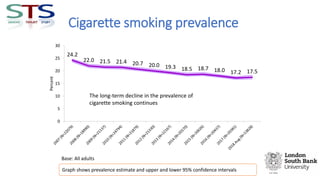
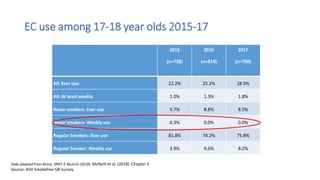
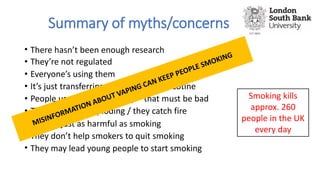
The document presents an evidence update on e-cigarettes by Dr. Lynne Dawkins, covering their regulation, usage among smokers and non-smokers, and potential health effects. It discusses various myths regarding e-cigarettes, emphasizing that while they contain nicotine, they are less harmful than traditional smoking and may aid in quitting. The document also highlights the rising popularity of e-cigarettes among adults and the limited impact on youth smoking rates.