09/07/2025 2
Diabetes Mellitus
•Definition:Diabetes mellitus (DM) refers to a group of
common metabolic disorders that share the phenotype
of hyperglycemia.
•Several distinct types of DM are caused by a complex
interaction of genetics and environmental factors.
09/07/2025 5
Regulation ofGlucose Homeostasis
Insulin is most important regulator of hepatic glucose
production & peripheral glucose uptake & utilization.
Fasting state: Low insulin levels
•Hepatic gluconeogenesis & glycogenolysis by
glucagon and increases glucose production:
•Reduce glucose uptake in insulin sensitive tissues
•Mobilization of stored precursors: AA & FFAs
6.
09/07/2025 6
Regulation ofGlucose Homeostasis…….
•Postprandial state: rise in insulin
•Illicit fall in glucagon.
• Insulin promotes storage of carbohydrate and fat &
protein synthesis
•Major postprandial glucose is used by skeletal muscles
09/07/2025 8
Insulin Secretion
•Insulinsecretion is regulated through 2 pathways :
•Direct regulation:
• Hyperglycemia sensed by β cells – the major one and
•Indirect
•Physiological stimuli : smell, sight and taste of food
•Diet containing CHOs (glucose) , proteins (AA ).
•Hormones: GH; Prolactin, Catecholamines
•Enteric hormones: Gastrin and Cholicystokinin
9.
09/07/2025 9
Epidemiology
Prevalence oftype 2 DM increasing due to
•Increasing Obesity & decreased activity
•80% 0f diabetics live in low & middle income countries
•DM increases with age
10.
09/07/2025 10
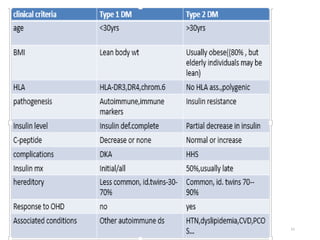
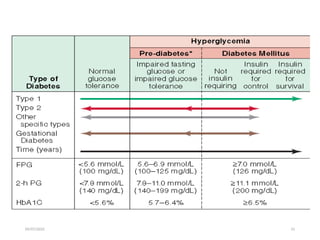
Classification
• Basedon pathogenic process that lead to hyperglycemia
• Two broad categories
• Type 1 DM :
• Complete or near- total insulin deficiency
• Type 2 DM:
a) variable degree of insulin resistance
b) Impaired insulin secretion
c)Increased glucose production
09/07/2025 12
•LADA-late onsetauto immune diabetes of adults
(type 1)
•Age >30yrs, more likely to be <50yrs
•Immune markers for type 1 present, islet cell auto
antibodies (ICA), Glutamic Acid
Decarboxylate(GAD) autoantibodies
•personal or family history of other autoimmune
disease.
•Respond to oral agents early phase, more likely to
require insulin treatment within 5 years
•Complete B-cell destruction over 2-3yrs
•Usually lean body wt(normal BMI)
13.
09/07/2025 13
Classification Cont…
•Maturity-onset diabetes of the young (MODY)
• are subtypes of DM characterized by autosomal
dominant inheritance
• early onset of hyperglycemia (usually <25 years;
sometimes in neonatal period)
• and impaired insulin secretion
14.
09/07/2025 14
Gestational DM
•Glucoseintolerance developing during pregnancy
•Most women revert to normal glucose tolerance
postpartum
•Risk of DM in the next 10-20years : 35-60%
•If diagnosed in early prenatal visit: “Overt” DM
09/07/2025 16
Pathophysiology…Type 1DM
• Interaction of Genetic, Environmental, & auto-immune
factors
• Several factors characterize type 1 DM as auto-immune
condition
• Association with genes of MHC/HLA
• Presence of Islet cell specific auto antibodies
• Frequent occurrence of other auto immune diseases
• 85% of patients have circulating islet cell auto
antibodies( ICA), Anti Insulin( AI), Anti Glutamic Acid
Decarboxylate ( Anti-GAD).
• Excessive secretion of Glucagon
17.
09/07/2025 17
Pathogenesis oftype 2 DM
• Insulin Resistance
•Increased hepatic Glucose production
•Decreased Insulin mediated Glucose
transport
•Impaired beta cell function
09/07/2025 19
Screening
• Widespreaduse screening test for type 2 DM is recommended
because
(1) a large number of individuals who meet the current criteria
for DM are asymptomatic and unaware that they have the
disorder,
(2) epidemiologic studies suggest that type 2 DM may be
present for up to a decade before diagnosis,
(3) some individuals with type 2 DM have one or more
diabetes-specific complications at the time of their diagnosis,
(4) treatment of type 2 DM may favorably alter the natural
history of DM.
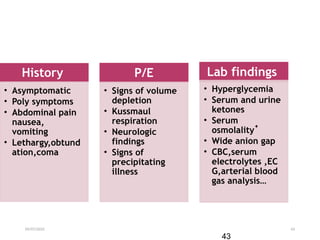
09/07/2025 21
Approach TODM patient
•Hx
•Family hx of DM & its cx
•Wt change
•Risk factors for CVD
•Exercise, alcohol use, smoking, nutritional hx
• Symptoms of hyperglycemia
• polyuria, polydipsia, weight loss, fatigue,
weakness, blurry vision
•Frequent superficial skin infections (vaginitis,
fungal skin infections),
•Delayed wound healing after minor trauma
22.
09/07/2025 22
•If knownDM
•type of Rx
•Level of gycemic control-Hgb A1c,FBS
•frequency of hypoglycemia
•Diabetic cx
•pt’s knowledge about DM, exercise, and
nutrition
•DM-related comorbidities -
HTN,CVD,dyslipidemia
23.
09/07/2025 23
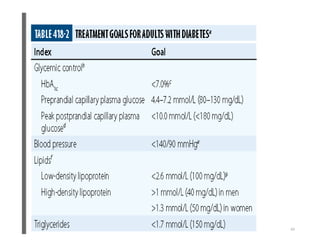
•P/E- complete+special attention on
•BMI.
•> 140/90 mmHg is considered HTN in DM.
•Oral hygiene, teeth and gums, periodontal
disease is more frequent
•Peripheral pulses
•Extremities
•Callus, nail disease
•Fungal superficial infections, ulcer, fissures
•deformity ( hammer or claw toes and Charcot
foot)
09/07/2025 30
Acute complications
•Diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic
state (HHS, also called nonketotic hyperglycemia) are two of
the most serious acute complications of diabetes
31.
09/07/2025 31
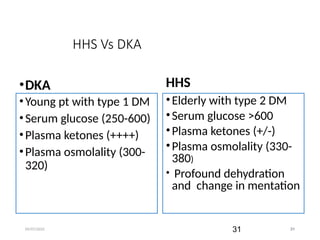
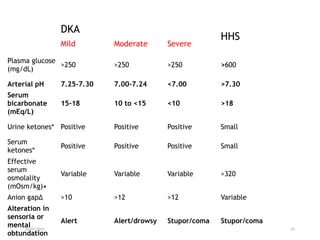
HHS VsDKA
•DKA
•Young pt with type 1 DM
•Serum glucose (250-600)
•Plasma ketones (++++)
•Plasma osmolality (300-
320)
HHS
•Elderly with type 2 DM
•Serum glucose >600
•Plasma ketones (+/-)
•Plasma osmolality (330-
380)
• Profound dehydration
and change in mentation
31
32.
09/07/2025 32
Diabetic Ketoacidosis
anacute, life threatening metabolic
acidosis complicating type 1DM and some
cases of type 2 DM.
usually coupled with an increase in glucagon
concentration with two metabolic
consequences:
1) Maximal gluconeogenesis with impaired
peripheral utilization of glucose
2) activation of the ketogenic process and
development of metabolic acidosis.
33.
09/07/2025 33
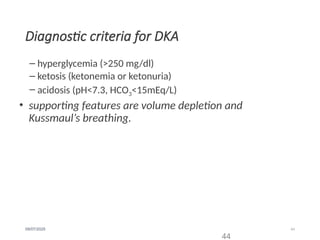
DKA…..
DKA ischaracterized by the triad of
hyperglycemia, metabolic acidosis, and
ketonemia. Metabolic acidosis is often the
major finding.
The serum glucose concentration is usually
greater than 250mg/dL and less than 600
mg/dL
However, serum glucose concentrations
may exceed 900 mg/dL (50 mmol/L) in
patients with DKA who are comatose
34.
09/07/2025 34
DKA …….
Mortalityin DKA is primarily due to the
underlying precipitating illness and only
rarely to the metabolic complications of
hyperglycemia or ketoacidosis
The prognosis of DKA is substantially
worse at the extremes of age and in the
presence of coma and hypotension
35.
35
09/07/2025
PATHOGENESIS
DKA results fromrelative or absolute insulin
deficiency combined with counterregulatory
hormone excess( glucagon, catecholamines,
cortisol, and growth hormone)
promotes gluconeogenesis, glycogenolysis, and
ketone body formation in the liver, as well as
increases in substrate delivery from fat and
muscle (free fatty acids, amino acids) to the
liver.→ hyperglycemia
Insulin deficiency also reduces levels of the GLUT4
glucose transporter
35
36.
36
09/07/2025
Ketogenesis
KETOGENESIS occurs asa results of high
glucagon/insulin ratio:
1) increased liberation of free fatty acids due to the loss
of the inhibitory action of insulin on the hormone
sensitive lipase.
2) activation of the transport system.
Normally, these free fatty acids are converted to
triglycerides or VLDL in the liver.
However, in DKA, hyperglucagonemia alters
hepatic metabolism to favor ketone body
formation.
36
37.
37
09/07/2025
As a resultof the hyperglycemia resultant osmotic
diuresis produces polyuria, urinary losses of
electrolytes, dehydration, and compensatory
polydipsia
Ketosis results in high levels of acetone,
acetoacetate and -hydroxybutyrate )→
metabolic acidosis
37
39
09/07/2025
Precipitating factors…..
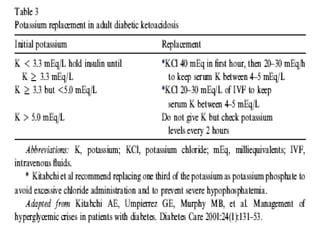
Electrolyte derangements
Metabolic acidosis and osmotic diuresis lead to total
body hypokalemia
The measured serum sodium is reduced as a
consequence of the hyperglycemia
Total-body stores of chloride, phosphorous, and
magnesium are also reduced in DKA.
39
09/07/2025 48
Principles ofmgt
Fluid replacement
Insulin therapy
Electrolyte replacement
Identification and Rx of ppt factors
Close monitoring
49.
09/07/2025 49
Fluid Replacement
Objectives:
Restoration of circulating volume.
Replacement of sodium and the ECF and intracellular fluid
deficit of water.
•Fluid loss averages 5L, hence replace 5-6L of fluid in the
first 24 hrs
Replace fluids: 2–3 L of 0.9% saline over first 1–3 h (10–20
mL/kg per hour
49
50.
09/07/2025 50
insulin therapyis essential:-
•Normalize blood glucose concentration.
•Suppress lipolysis and ketogenesis and
•Correct acidosis.
•increases peripheral ketone body use
Insulin therapy
50
51.
09/07/2025 51
Insulin
Administer short-actinginsulin: 0.1 units/kg per hour
by continuous IV infusion
Increase two- to threefold if no response by 2–4 h.
If the initial serum potassium is <3.3 mmol/L (3.3
meq/L), do not administer insulin until the potassium
is corrected.
The insulin decreases glucose by 50-70mg/dl per hr.
51
52.
09/07/2025 52
Insulin……
However,if the serum glucose doesn’t fall by 50-
70mg/dl in first hour, double insulin infusion rate every
hour until steady decline is achieved.
Maintain the serum glucose between 150-250mg/dl
Give initial bolus of 10IU IV and 10 IU IM of regular
insulin
Then give 5 IU IV every one hour until blood sugar
falls below 200 and urine ketone is twice negative
52
53.
09/07/2025 53
cont…
In Patientswith known diabetes who were previously
treated with insulin may be given insulin at the dose
they were receiving before the onset of DKA
In insulin-naive patients, insulin regimen should be
started at a dose of 0.5 to 0.8 U/kg per day
Administer long-acting insulin overlapping with
insulin infusion and SC insulin injection for a 2–4
hour
53
09/07/2025 56
Follow up
Clinical
•Vital signs(Q 1-4 hrs)
• Input/output
• Mental status
Lab
• RBS(Q 1-2 hrs)
• Urine ketone(Q 2-4
hrs)
• Serum K+(Q 4hrs for
the 1st
24 hrs)
• RFT
56
57.
09/07/2025 57
Complications ofDKA
Hypoglycemia (common)
Hypokalemia
Cerebral edema,
High mortality
Treat with mannitol, oxygen
ARDS
Fluid overload,
58.
09/07/2025 58
HHS treatment
Similarprinciples of management with DKA
Calculated fluid deficit averages 9-10 L, should be
reversed over the next 1 to 2 days
Patient should be discharged on insulin ( some may
switch to oral agents later.
58
59.
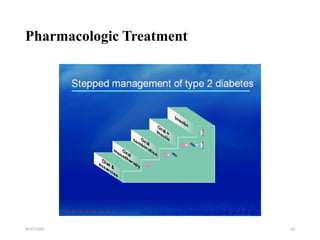
09/07/2025 59
Management ofDM
Pt education
prevention - diet, exercise
Mx during acutes illnesses
Mx of hypoglycemia
foot & skin care
modify risk factors
60.
09/07/2025 60
•Exercise
• ↓CVSrisk ,↓BP,↓body fat,↓blood glucose
• Maintain muscle mass
• Increase insulin sensitivity
• Can lead to hyper/hypoglycemia based on
• Pre exercise glycemic level
• Pre exercise insulin level
• Extent of exercise
61.
09/07/2025 61
Exercise…..
• MonitorRBS before, during & after ex.
• Delay if RBS <100mg/dl or >250
• Eat meal 1-3hr before ex. Or take supplemental CHO
atleast every 30min.
• ↓insulin doses
• Avoid injection of insulin to the exercising limb
09/07/2025 65
Quiz
1) Writefive precipitants of DKA
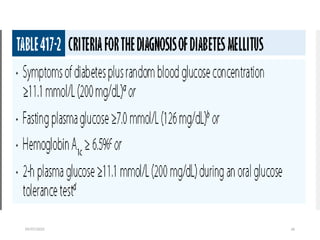
2) Write diagnostic criteria of DM and DKA
3) What are complications of DM
4) Write management principles of DKA
5) What are components of Islets of langrhans