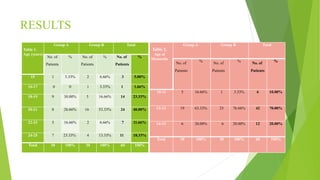
The document presents a dissertation on a comparative study assessing the utility of Kent's Repertory and Boger Boenninghausen's Characteristics and Repertory (BBCR) in managing primary dysmenorrhea and improving quality of life in women aged 15-25 years. It includes sections on aim and objectives, methodology, sample size estimation, results, discussion, and conclusion. The study involved 60 subjects divided into two groups, with Group A treated using Kent's Repertory and Group B treated using BBCR. Various statistical tests were used to analyze results and compare the effectiveness of the two repertories in improving symptoms and quality of life. Key findings from the results section include demographic characteristics of subjects and comparisons of effectiveness between the












![SAMPLE SIZE CALCULATION FORMULA
[Based on standard deviation]
Sample size is calculated using the standard deviation formula: n = 2 (a+b)2σ2 / d2
Where,
n = Sample size
a = Probability of falsely rejecting a true null hypothesis = 1.96 (5% level)
b = Probability of failing to reject a false null hypothesis = 1.2816 (90% power)
σ = Standard deviation of the outcome measure or population being studied = 2.3
d = Size of the effect that is clinically worthwhile to detect = 2
SAMPLE SIZE CALCULATION:
n = 2 ( 1.96 + 1.2816) 2 × ( 2.3 )2 / 22
= 2 ( 3.2416 ) 2 × 5.29 / 4
= 2 × 10.50797056 × 5.29 / 4
= 111.17432852 / 4
= 27.79 ≈28.
In the view of 5% drop outs, sample size was considered 30 in each group.](https://image.slidesharecdn.com/dissertationpresentation-220816135705-7e2c13c2/85/DISSERTATION-PRESENTATION-pptx-14-320.jpg)




























![Boenninghausen’s therapeutic pocket book[btpb]](https://cdn.slidesharecdn.com/ss_thumbnails/boenninghausenstherapeuticpocketbookbtpb-170801133521-thumbnail.jpg?width=640&height=640&fit=bounds)













































