Parasympathetic Nervous
System
REST ANDDIGESTION
•Prepares Body For Rest
•Promotes Digestion, GI Peristalsis
•Slows Heart Rate
•Constricts Pupil
•Empties Bladder
•Relaxes Sphincters.
5.
Sympathetic Nervous System
“Fightor Flight” system
Activation
•Increases Heart Rate
•Increases Sweating
•Dilates Pupil
•Inhibits GI Movement
•Closes Sphincters.
6.
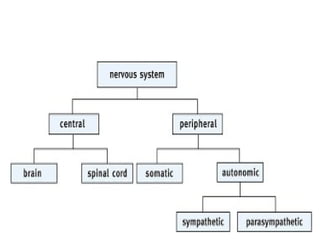
Receptors Of AutonomicNervous System
• Receptors Of Parasympathetic Nervous Systm:
• Muscarinic receptors.
• Nicotinic receptors.
• Receptors Of Sympathetic Nervous Systm:
• Alpha 1,
• Alpha 2.
• Beta 1,
• Beta 2,
• Beta 3.
• D 1,
• D 2.
10.
CHOLINERGIC RECEPTORS
• Thereare two types of Cholinergic Receptors:
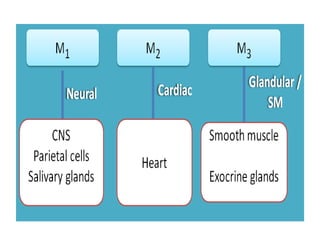
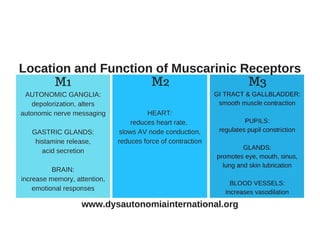
• 1. Muscarinic Receptors:
• There are five subclasses of Muscarinic
Receptors:
• M1,
• M2,
• M3,
• M4,
• M5.
15.
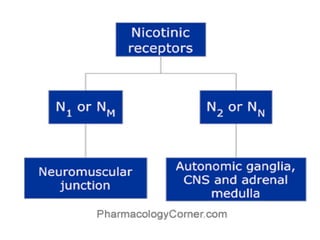
Nicotinic receptors
• Nicotinicreceptors are of 2 types.
• Nicotinic receptors are located in the CNS,
Adrenal Medulla, Autonomic Ganglia, and the
Neuromuscular Junction. Those at the
Neuromuscular Junction are sometimes
designated NM and the others NN.
16.
MECHANISM OF ACTION
•MUSCURINIC RECEPTORS are G protein
coupled receptors. M1 and M3 are Gq coupled
receptors. They activate Phospholipase C.
• Phospholipase C leads to the release of
Diacylglycerol (DAG) and Inositol 1,4,5
triphosphate (IP3).
• IP3 releases the Calcium from intracellular
storage sites and results in contraction of
smooth muscle.
17.
• M2 receptorsare Gi coupled receptors.
they inhibits Adenylyl Cyclase and
increases K+ conductance, to which the
heart responds with a decrease in rate
and force of contraction.
18.
MECHANISM OF ACTION
•NICOTINIC RECEPTORS: They are ligand gated
ion channels.
• When activated they open ion channels.
• Produces contraction of the cells.
19.
CHOLINERGIC AGONISTS
• CholinergicAgonists Are Divided Into:
I. Direct acting cholinergic agonists.
II.Indirect acting cholinergic agonists
20.
Direct-Acting Cholinergic Agonists
•They mimic the effects of acetylcholine by
binding directly to cholinoceptors.
• These agents may be broadly classified into
two groups:
• 1.Choline esters: which include Acetylcholine,
and Synthetic Esters of Choline, such as
Carbachol and Bethanechol.
• 2. Naturally occurring alkaloids, such as
Pilocarpine and Nicotine.
21.
• All directacting cholinergic agonist are
different in their spectrum of action and
in their pharmacokinetics.
22.
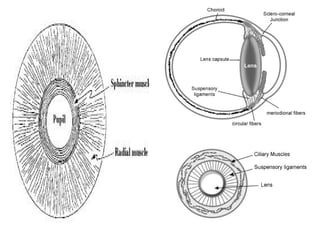
Effect On TissuesAnd Organs
• ON EYE:
• Cholinergic agonist causes contraction of
smooth muscle of pupillae Sphincter (resulting in
Miosis).
• Contraction of ciliary muscle (resulting in
accomodation).
• Both actions fasilitate aqueous humour outflow
and decreases IoP (Intraoccular Pressure).
24.
• On CVS:
•They causes vasodilation and decreases blood
pressure.
• Reflex tachycardia.
• Bradycardia due to their parasympathetic
stimulation.
25.
• ON GIT:
•They increases the secretory and motor
activity of GUT.
• Salivary and gastric glands are also strongly
stimulated.
• Peristaltic activity also increased throughout
the Gut.
26.
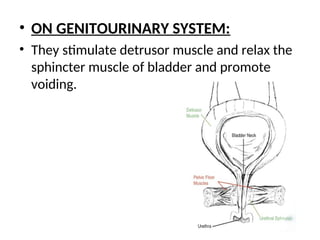
• ON GENITOURINARYSYSTEM:
• They stimulate detrusor muscle and relax the
sphincter muscle of bladder and promote
voiding.
27.
Clinical Uses
• Glaucoma.
•Sjogren’s Syndrome.
• Loss Of Normal Pans Activity In
Bowel And Bladder,
• Cessation Of Smoking.
ACETYLCHOLINE:
• is aquaternary ammonium
compound that cannot penetrate
membranes. it is therapeutically of
No Importance because of its
multiple actions and its rapid
inactivation by the cholinesterases.
• Acetylcholine has both muscarinic
and nicotinic activity.
31.
• Its ActionsInclude:
• Decrease In Blood Pressure:
• Acetylcholine causes vasodilation and lowering
of blood pressure by activating M3 receptors
found on endothelial cells lining of the smooth
muscles of blood vessels This results in the
production of EDRF; NITRIC OXIDE.
• Nitric oxide then diffuses to vascular smooth
muscle cells to stimulate protein kinase G
production, leading to hyperpolarization and
smooth muscle relaxation
32.
Decrease In HeartRate And Cardiac
Output:
• The actions of acetylcholine on the heart
mimic the effects of vagal stimulation.
• AcH produces a brief decrease in cardiac
rate (bradycardia) as a result of a
reduction in the rate of firing at the
sinoatrial (SA) node.
33.
:Other Actions:
• Inthe gastrointestinal tract, acetylcholine
increases salivary and Gastric secretions and
stimulates intestinal secretions and motility.
• In the genitourinary tract, the tone of the
detrusor muscle is increased, causing
expulsion of urine.
• In the eye, acetylcholine is involved in
stimulating ciliary muscle contraction for near
vision (Accomodaion) and constriction of the
pupillae sphincter muscle, causing Miosis.
34.
BETHANECHOL
• is structurallyrelated to acetylcholine.
• It is not hydrolyzed by acetylcholinesterase
(due to the addition of carbonic acid),
although it is inactivated through hydrolysis
by other esterases.
• Its major actions are on the smooth
musculature of the bladder and
gastrointestinal tract.
• It has a duration of action of about 1 hour
35.
• ACTIONS:
• Bethanecholdirectly stimulates muscarinic
receptors, causing increased intestinal motility
and tone.
• It also stimulates the detrusor muscles of the
bladder whereas the trigone and sphincter are
relaxed, causing expulsion of urine.
• Therapeutic applications: In urologic
treatment, bethanechol is used to stimulate
the atonic bladder, particularly in postpartum
or postoperative cases.
36.
• ADVERSE EFFECTS:
•Bethanechol causes the effects of generalized
cholinergic stimulation. These include:
• Sweating,
• Salivation,
• Decreased Blood Pressure,
• Nausea,
• Abdominal Pain,
• Diarrhea.
37.
CARBACHOL
• has bothmuscarinic as well as nicotinic
actions.
• Like bethanechol, carbachol is a poor
substrate for acetylcholinesterase.
• It is biotransformed by other esterases,
but at a much slower rate.
38.
PILOCARPINE
• is alkaloidwith a tertiary amine and is stable
to hydrolysis by ACETYLCHOLINESTERASE.
• Compared with acetylcholine and its
derivatives, it is far less potent.
• Pilocarpine exhibits Muscarinic activity and is
used primarily in Ophthalmology.
39.
• Pilocarpine producesrapid Miosis
and Spasm Of Accomodation.
• It is potent stimulator of secretions.
40.
• Nicotine:
• Itactivates nicotinic receptors.
• Used in cessation of smoking.