Dental implants |Limitations |
biomaterials
Topic
Oct 2025
Dr Adnan Sunny
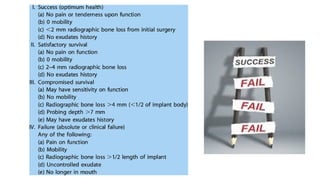
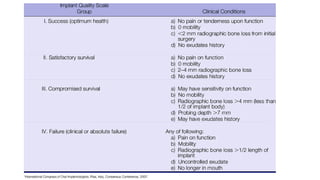
2.
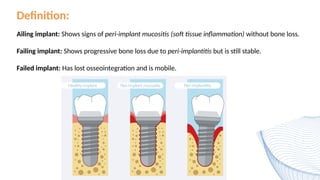
Definition:
Ailing implant: Showssigns of peri-implant mucositis (soft tissue inflammation) without bone loss.
Failing implant: Shows progressive bone loss due to peri-implantitis but is still stable.
Failed implant: Has lost osseointegration and is mobile.
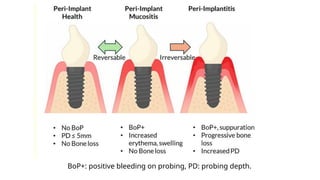
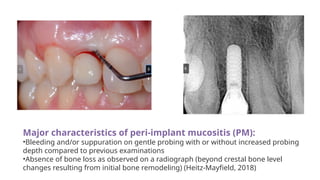
Major characteristics ofperi-implant mucositis (PM):
•Bleeding and/or suppuration on gentle probing with or without increased probing
depth compared to previous examinations
•Absence of bone loss as observed on a radiograph (beyond crestal bone level
changes resulting from initial bone remodeling) (Heitz-Mayfield, 2018)
5.
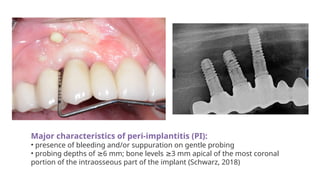
Major characteristics ofperi-implantitis (PI):
• presence of bleeding and/or suppuration on gentle probing
• probing depths of 6 mm; bone levels 3 mm apical of the most coronal
≥ ≥
portion of the intraosseous part of the implant (Schwarz, 2018)
Implant failure (FI):
•Implant presenting 50% of bone loss
≥
• Mobile implant
• Loss of osseointegration
• Persistent inflammation described by presence of profuse bleeding and/or
suppuration and a radiographically documented continuous bone loss despite
treatment (Misch, 2008).
10.
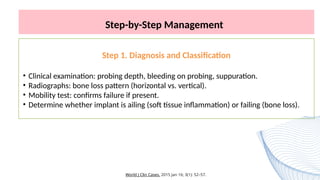
Step-by-Step Management
Step 1.Diagnosis and Classification
• Clinical examination: probing depth, bleeding on probing, suppuration.
• Radiographs: bone loss pattern (horizontal vs. vertical).
• Mobility test: confirms failure if present.
• Determine whether implant is ailing (soft tissue inflammation) or failing (bone loss).
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
Step 3. Nonsurgical(Conservative) Management
Applicable to ailing and early failing implants:
1. Mechanical debridement: plastic/titanium instruments, ultrasonic with plastic tip.
2. Antiseptic treatment: 0.12–0.2% chlorhexidine irrigation and maintenance.
3. Local antibiotic therapy: minocycline microspheres or doxycycline gel.
4. Laser or photodynamic therapy: to decontaminate the surface.
5. Occlusal adjustment: reduce overload or premature contacts.
6. Cement removal: if peri-implantitis is cement-induced.
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
13.
Step 4. SurgicalManagement
Indicated for advanced failing implants with bone loss:
• Flap reflection and debridement to access contaminated threads.
• Mechanical decontamination: titanium brushes, air abrasion, laser decontamination.
• Chemical decontamination: citric acid, tetracycline, EDTA, chlorhexidine.
• Regenerative approach: bone graft + membrane for contained defects.
• Resective surgery: implantoplasty + apically positioned flap for non-contained defects.
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
14.
Step 5. Maintenanceand Follow-up
• Recall every 3–6 months.
• Reinforce hygiene, remove calculus, monitor probing depth and radiographs.
• Success depends on early detection and complete debridement.
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
15.
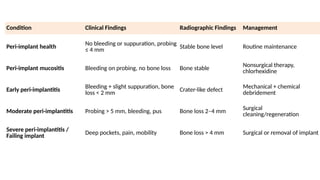
Condition Clinical FindingsRadiographic Findings Management
Peri-implant health No bleeding or suppuration, probing
≤ 4 mm Stable bone level Routine maintenance
Peri-implant mucositis Bleeding on probing, no bone loss Bone stable Nonsurgical therapy,
chlorhexidine
Early peri-implantitis
Bleeding + slight suppuration, bone
loss < 2 mm Crater-like defect
Mechanical + chemical
debridement
Moderate peri-implantitis Probing > 5 mm, bleeding, pus Bone loss 2–4 mm Surgical
cleaning/regeneration
Severe peri-implantitis /
Failing implant
Deep pockets, pain, mobility Bone loss > 4 mm Surgical or removal of implant
16.
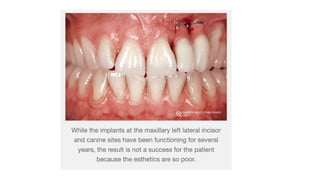
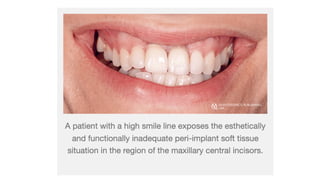
Implant Crown EstheticIndex (ICAI)
Developed by Fürhauser et al. (2005) to objectively evaluate the esthetic outcome of
implant-supported single crowns, especially in the anterior maxilla.
17.
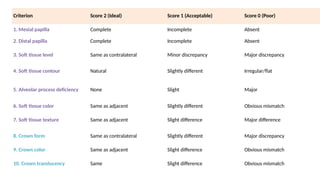
Criterion Score 2(Ideal) Score 1 (Acceptable) Score 0 (Poor)
1. Mesial papilla Complete Incomplete Absent
2. Distal papilla Complete Incomplete Absent
3. Soft tissue level Same as contralateral Minor discrepancy Major discrepancy
4. Soft tissue contour Natural Slightly different Irregular/flat
5. Alveolar process deficiency None Slight Major
6. Soft tissue color Same as adjacent Slightly different Obvious mismatch
7. Soft tissue texture Same as adjacent Slight difference Major difference
8. Crown form Same as contralateral Slightly different Major discrepancy
9. Crown color Same as adjacent Slight difference Obvious mismatch
10. Crown translucency Same Slight difference Obvious mismatch
Implant biomaterials?
• Thosematerials that are compatible with the living tissues
• The main goal of biomaterials research has is to develop implant materials that induce
predictable, control-guided and rapid healing of the tissues
• The materials biocompatibility (tissue response) is dependent on the basic bulk and surface
properties
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
Biocompatibility
This is property of implant material to show favorable response in given biological
environment in a particular function. It depends on the corrosion resistance and
cytotoxicity of corrosion products.
23.
PROPERTIES OF ANIMPLANT BIOMATERIAL
Bulk properties
Modulus of elasticity: Implant material with modulus of elasticity comparable to bone
(18 GPa) must be selected to ensure more uniform distribution of stress at implant and
to minimize the relative movement at implant bone interface.
Tensile, compressive and shear strength: An implant material should have high tensile
and compressive strength to prevent fractures and improve functional stability.
Improved stress transfer from the implant to bone is reported interfacial shear strength
is increased, and lower stresses in the implant.
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
24.
PROPERTIES OF ANIMPLANT BIOMATERIAL
Bulk properties
Yield strength, fatigue strength: An implant material should have high yield
strength and fatigue strength to prevent brittle fracture under cyclic loading.
Ductility: According to ADA a minimum ductility of 8% is required for dental
implant. Ductility in implant is necessary for contouring and shaping of an
implant.
Hardness and Toughness: Increase in hardness decreases the incidence of wear
of implant material and increase in toughness prevents fracture of the implants.
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
25.
PROPERTIES OF ANIMPLANT BIOMATERIAL
Corrosion and corrosion resistance: It is the loss of metallic ions from metal
surface to the surrounding environment
Clinical significance of corrosion:
Corrosion can result in roughening of the surface, weakening of the restoration,
release of elements from the metal or alloy, toxic reactions. Adjacent tissues may be
discolored and allergic reactions in patients may result due to release of elements.
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
26.
Bio-
inert
Materials that donot chemically bond with bone; they are
biocompatible but form only a mechanical attachment.
Commercially pure titanium.
Mere physical contact.
Bio-
tolerant
.
Bio-
active
Materials that chemically bond with surrounding bone and stimulate
biological responses (osseointegration + bioactivity).
World
J
Clin
Cases.
2015
Jan
16;
3(1):
52–57.
Bio tolerant are those that are not necessarily rejected when implanted into
living tissue ie co cr alloys, stainless and polymers
Hydroxyapatite (HA) coated titanium
27.
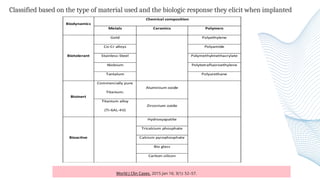
Classified based onthe type of material used and the biologic response they elicit when implanted
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
28.
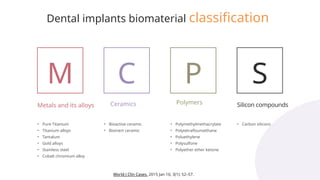
Dental implants biomaterialclassification
M C P S
Metals and its alloys Ceramics Polymers Silicon compounds
• Pure Titanium
• Titanium alloys
• Tantalum
• Gold alloys
• Stainless steel
• Cobalt chromium alloy
• Bioactive ceramic
• Bioinert ceramic
• Polymethylmethacrylate
• Polytetraflouroethane
• Poluethylene
• Polysulfone
• Polyether ether ketone
• Carbon silicons
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
29.
Metal and metalalloys
Most used are: titanium and it alloys, tantalum and alloys of aluminum,
vanadium, cobalt, chromium, molybdenum and nickel
Pure Titanium
And it alloys
Cobalt chromium
alloys
Iron-Chromium-N
ickel Based Alloys 17
World Wide Office
Total studio we have
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
30.
T i ta n i u m
• Titanium most commonly used implant
material.
• Titanium – Gold standard.
• Composition of Commercially pure titanium
• Titanium 99.75% – Iron 0.05% – Oxygen
0.1% – Nitrogen 0.03% – Hydrogen 0.012%
– Carbon 0.05%
• Ti is a dimorphic metal i.e. below 882.5 °C it exists
as -phase and above this temperature it changes
α
form - phase to phase
α β
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
31.
T i ta n i u m
Excellent biocompatibility, corrosion
resistant.
Commercially pure titanium is
available in four grades (1-4) which
vary according to the oxygen (0.18-
0.40 wt)
• Pure titanium forms several oxides
TiO,TiO2,Ti2O3
• TiO2 most stable
• Cp titanium grade I (0.18% Oxygen)
• Cp titanium grade II (0.25% Oxygen)
• Cp titanium grade III (0.35% Oxygen)
• Cp titanium grade IV (0.40% Oxygen)
Grade I is the purest and softest form
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
32.
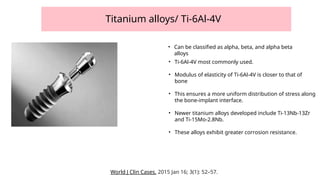
Titanium alloys/ Ti-6Al-4V
•Ti-6Al-4V most commonly used.
• Modulus of elasticity of Ti-6Al-4V is closer to that of
bone
• This ensures a more uniform distribution of stress along
the bone-implant interface.
• Newer titanium alloys developed include Ti-13Nb-13Zr
and Ti-15Mo-2.8Nb.
• These alloys exhibit greater corrosion resistance.
• Can be classified as alpha, beta, and alpha beta
alloys
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
33.
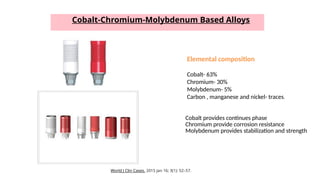
Cobalt-Chromium-Molybdenum Based Alloys
Cobaltprovides continues phase
Chromium provide corrosion resistance
Molybdenum provides stabilization and strength
Elemental composition
Cobalt- 63%
Chromium- 30%
Molybdenum- 5%
Carbon , manganese and nickel- traces.
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
34.
Iron-Chromium-Nickel
Based Alloys
The compositionof these alloys is typically
30-35% Nickel,
19-23% Chromium
and a minimum of 39.5% Iron.
The high concentration of iron has led to the
reclassification of these alloys as stainless steel.
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
35.
CERAMICS
Nonorganic, nonmetallic, nonpolymeric
materialsmanufactured by compacting and
sintering at elevated temperatures
• Bioactive: Bioglass /Glass ceramic
• Bioinert: Alumina, zirconia and carbon
According to the tissue response they are
categorized as
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
• Aluminium oxide (Al2O3)
• Zirconium oxide
• Hydroxyapatite (HA)
• Tricalcium phosphate
• Tetracalcium phosphate
• Calcium pyrophosphate Fluorapatite
• Brushite
• Bioglass etc
36.
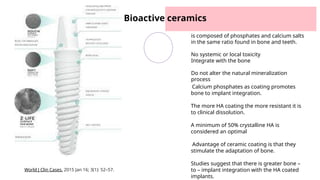
Bioactive ceramics
is composedof phosphates and calcium salts
in the same ratio found in bone and teeth.
No systemic or local toxicity
Integrate with the bone
Do not alter the natural mineralization
process
Calcium phosphates as coating promotes
bone to implant integration.
The more HA coating the more resistant it is
to clinical dissolution.
A minimum of 50% crystalline HA is
considered an optimal
Advantage of ceramic coating is that they
stimulate the adaptation of bone.
Studies suggest that there is greater bone –
to – implant integration with the HA coated
implants.
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
37.
POLYMERS
PTFE=polytetrafluoroethylene
PMMA = polymethylmethacrylate
PP= polypropylene
PSF = polysulfone
PDS = polydimethyl siloxane
SR = silicon rubber
PEEK= polyether ether ketone
Disadvantages
• Sensitive to sterilization
• Tend gather dust
• Require high care to preserve
quality
• Deformed easily/low strength
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
38.
modifications can increasethe degree of surface
roughness. •
This roughness shows a higher success rate when
compared with smooth surface implants . which
Improves implant early stability
Shorten the healing time.
Implant
surface
modifications
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
39.
1
2
3
c la ssi fi c a tio n
Modifications can be basically classified
into
Micro-level surface
modification
Macro-level surface modification..
Nano-level surface
modification.
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
40.
Related to implantgeneral design,
for example
• Implant design and topography
• Thread shape
• Thread depth
• Thread width
• Thread pitch
• Thread helix angle
Macro-level surface
modification
World J Clin Cases. 2015 Jan 16; 3(1): 52–57.
41.
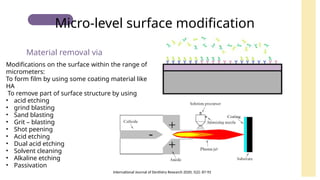
Modifications on thesurface within the range of
micrometers:
To form film by using some coating material like
HA
To remove part of surface structure by using
• acid etching
• grind blasting
• Sand blasting
• Grit – blasting
• Shot peening
• Acid etching
• Dual acid etching
• Solvent cleaning
• Alkaline etching
• Passivation
Material removal via
Micro-level surface modification
International Journal of Dentistry Research 2020; 5(2): 87-92
42.
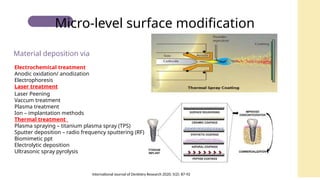
Electrochemical treatment
Anodic oxidation/anodization
Electrophoresis
Laser treatment
Laser Peening
Vaccum treatment
Plasma treatment
Ion – implantation methods
Thermal treatment
Plasma spraying – titanium plasma spray (TPS)
Sputter deposition – radio frequency sputtering (RF)
Biomimetic ppt
Electrolytic deposition
Ultrasonic spray pyrolysis
Material deposition via
Micro-level surface modification
International Journal of Dentistry Research 2020; 5(2): 87-92
43.
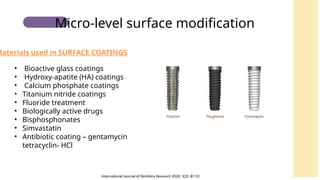
• Bioactive glasscoatings
• Hydroxy-apatite (HA) coatings
• Calcium phosphate coatings
• Titanium nitride coatings
• Fluoride treatment
• Biologically active drugs
• Bisphosphonates
• Simvastatin
• Antibiotic coating – gentamycin
tetracyclin- HCl
Materials used in SURFACE COATINGS
Micro-level surface modification
International Journal of Dentistry Research 2020; 5(2): 87-92
44.
•Modifications within nanometers.
Canincrease the surface area of implants.
Believed to improve bone formation process.
Organic nanoscale self-assembled monolayers
Hydrogels on titanium surface
Titanium nanotubes
Nano-level surface modification
International Journal of Dentistry Research 2020; 5(2): 87-92
45.
CURRENT TRENDS
The introductionof nanotechnology has opened a new door in the field
of implant dentistry. In recent years, advent of nanostructured
materials such as polymer nano composites has provided us the
opportunity for the development of computer model designed new
implant materials with pre determined shapes and porosities
International Journal of Dentistry Research 2020; 5(2): 87-92
46.
CONCLUSION
Since long titaniumand titanium alloys have been most
frequently used materials due to their excellent
biocompatibility and superior mechanical properties. Zirconia-
based ceramics have higher biocompatibility and better
aesthetics than titanium-based alloys; on the contrary titanium-
based implants have shown to have significantly better
mechanical properties, longer history of application and
therefore, achieved reliability over time. Thus, zirconia stands is
known to have a promising future in upcoming years
International Journal of Dentistry Research 2020; 5(2): 87-92
47.
1. A 30-year-oldpatient requires implant placement. When selecting an implant
material, which of the following allows the formation of new bone on its surface but
does not allow chemical bonding at the bone-implant interface?
A) Bioactive materials
B) Bioinert materials
C) Biotolerant materials
D) Both bioactive and bioinert materials
Answer:
B) Bioinert materials
48.
2. A clinicianis selecting the appropriate commercially pure (Cp) titanium grade for a dental implant
procedure. The decision must consider the mechanical properties required for implant stability and long-term
durability. Which of the following statements is TRUE regarding the grades of Cp titanium available for dental
implants?
A) Grade I Cp titanium has the highest oxygen content
B) Grade II Cp titanium is softer than Grade IV but has lower oxygen content.
C) Grade IV Cp titanium, with the highest oxygen content (0.40%)
D) Grade III Cp titanium, with 0.18% oxygen content
Answer:
C) Grade IV Cp titanium, with the highest oxygen content (0.40%)