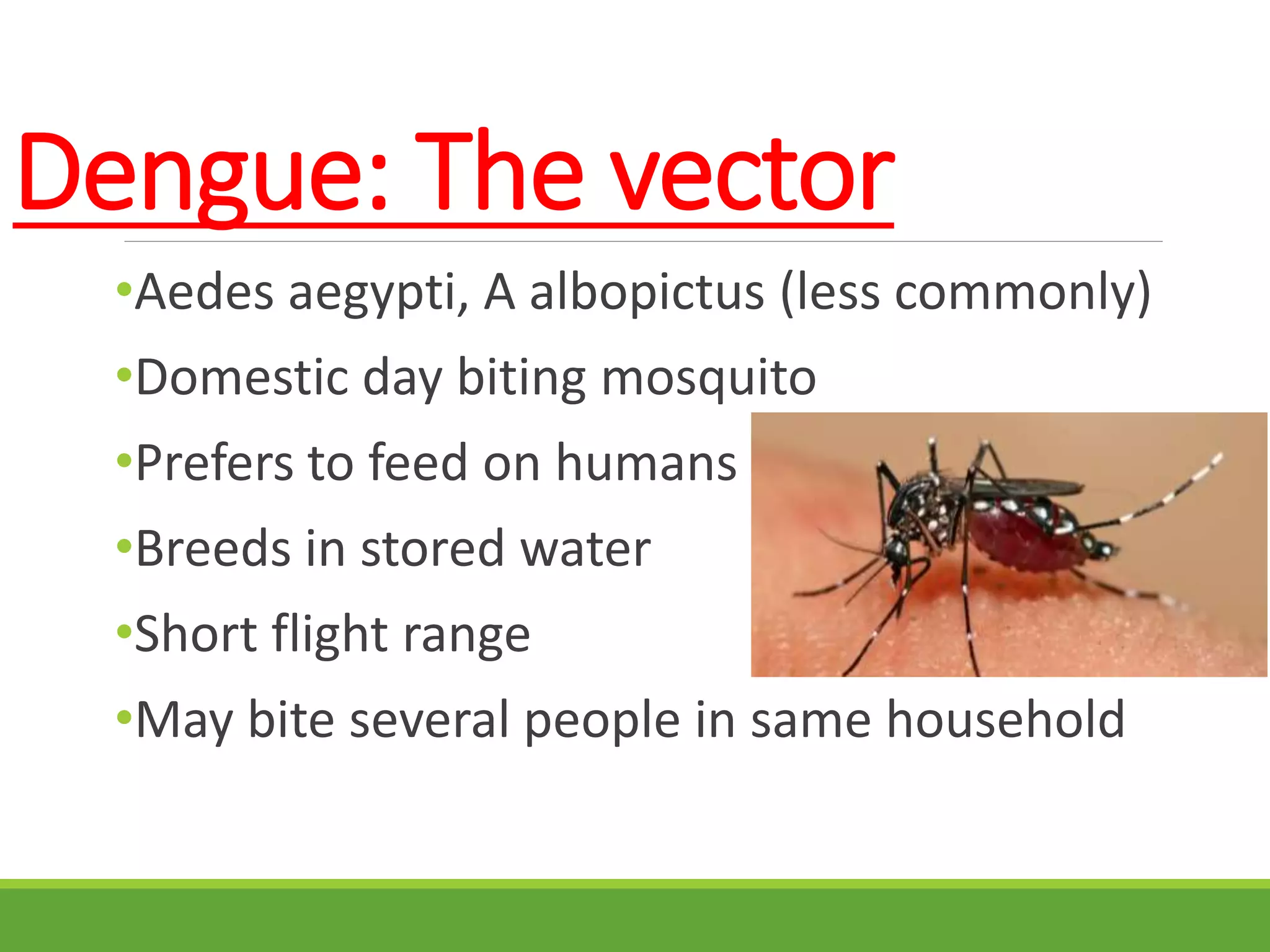
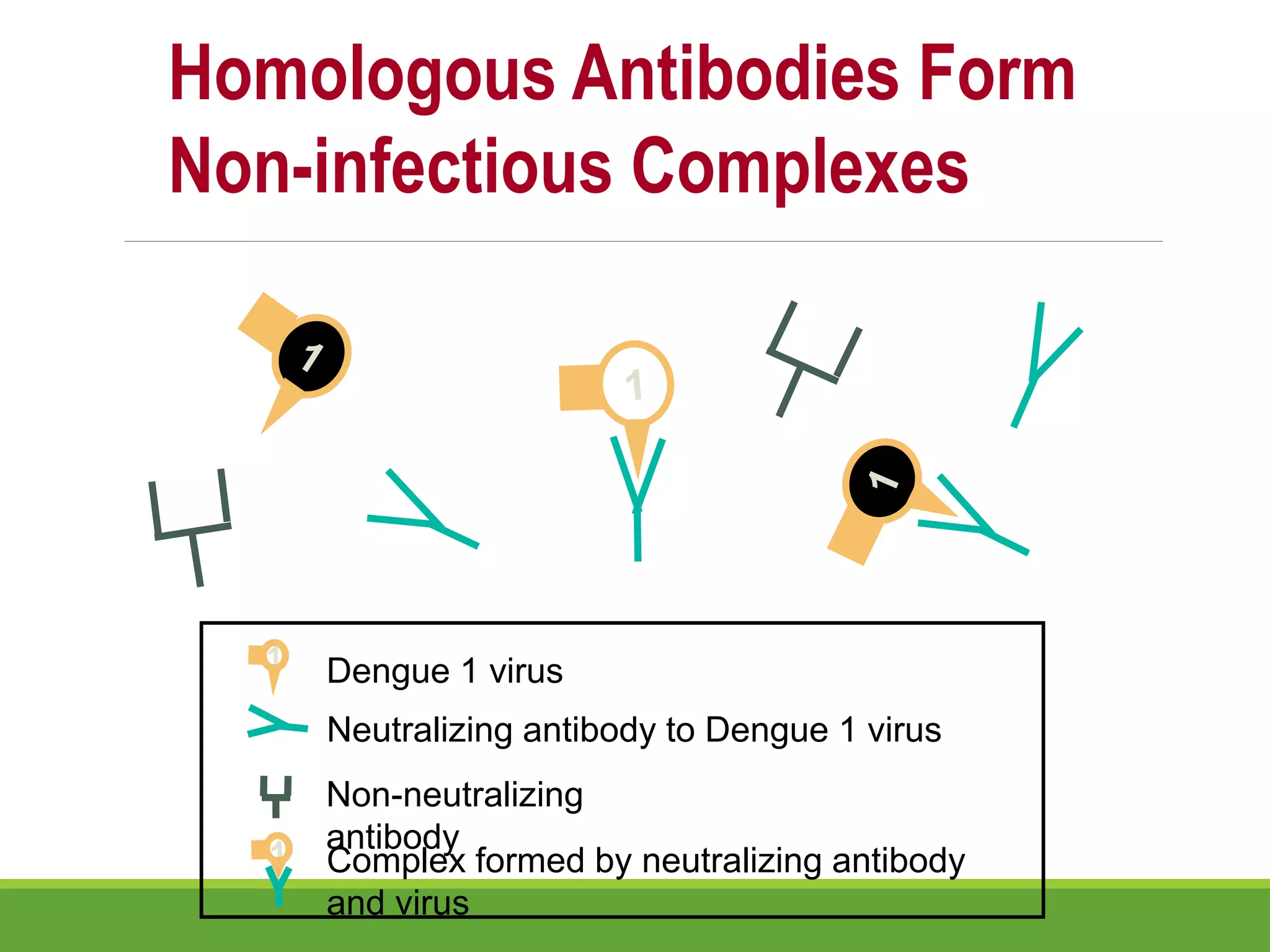
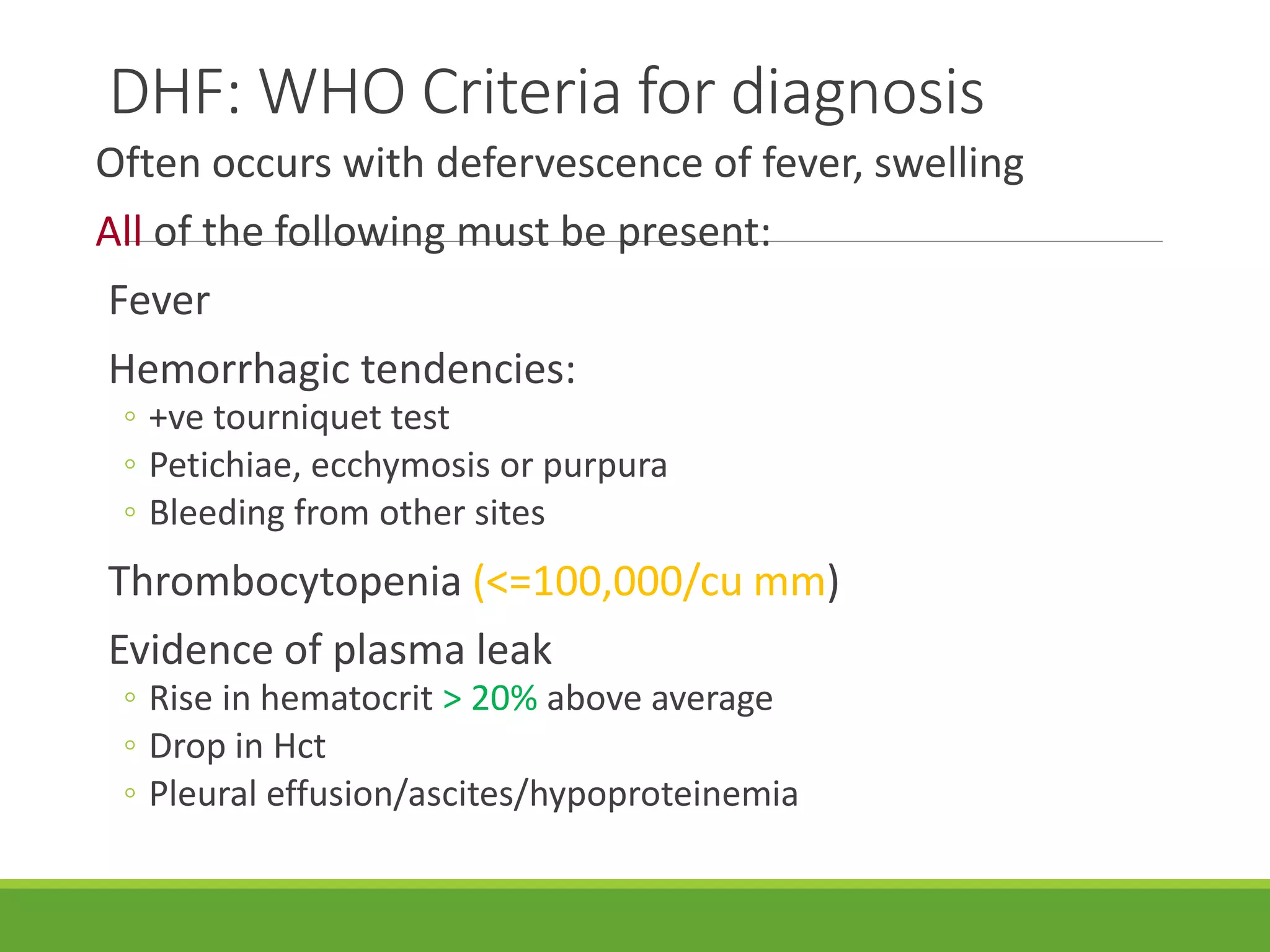
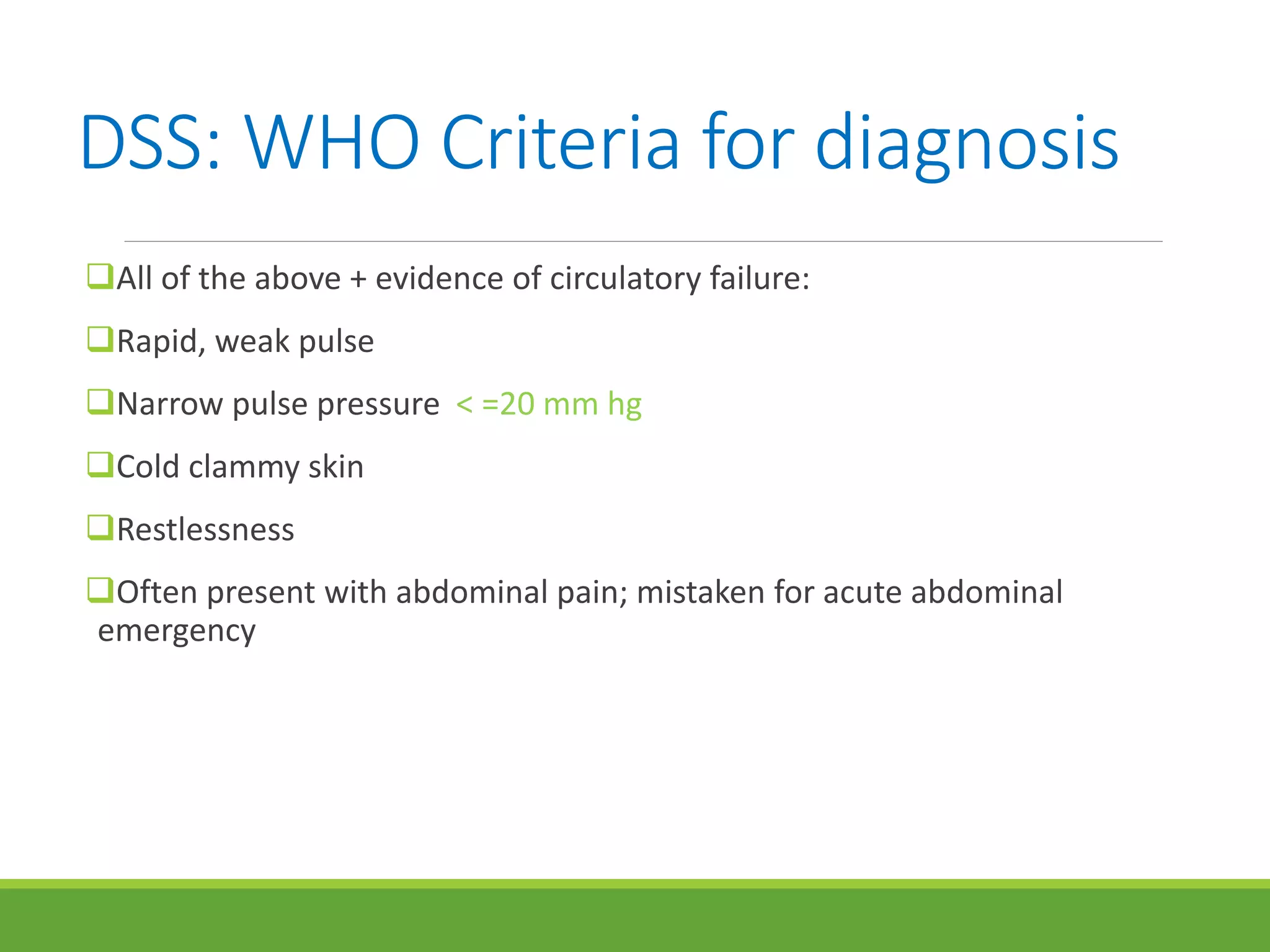
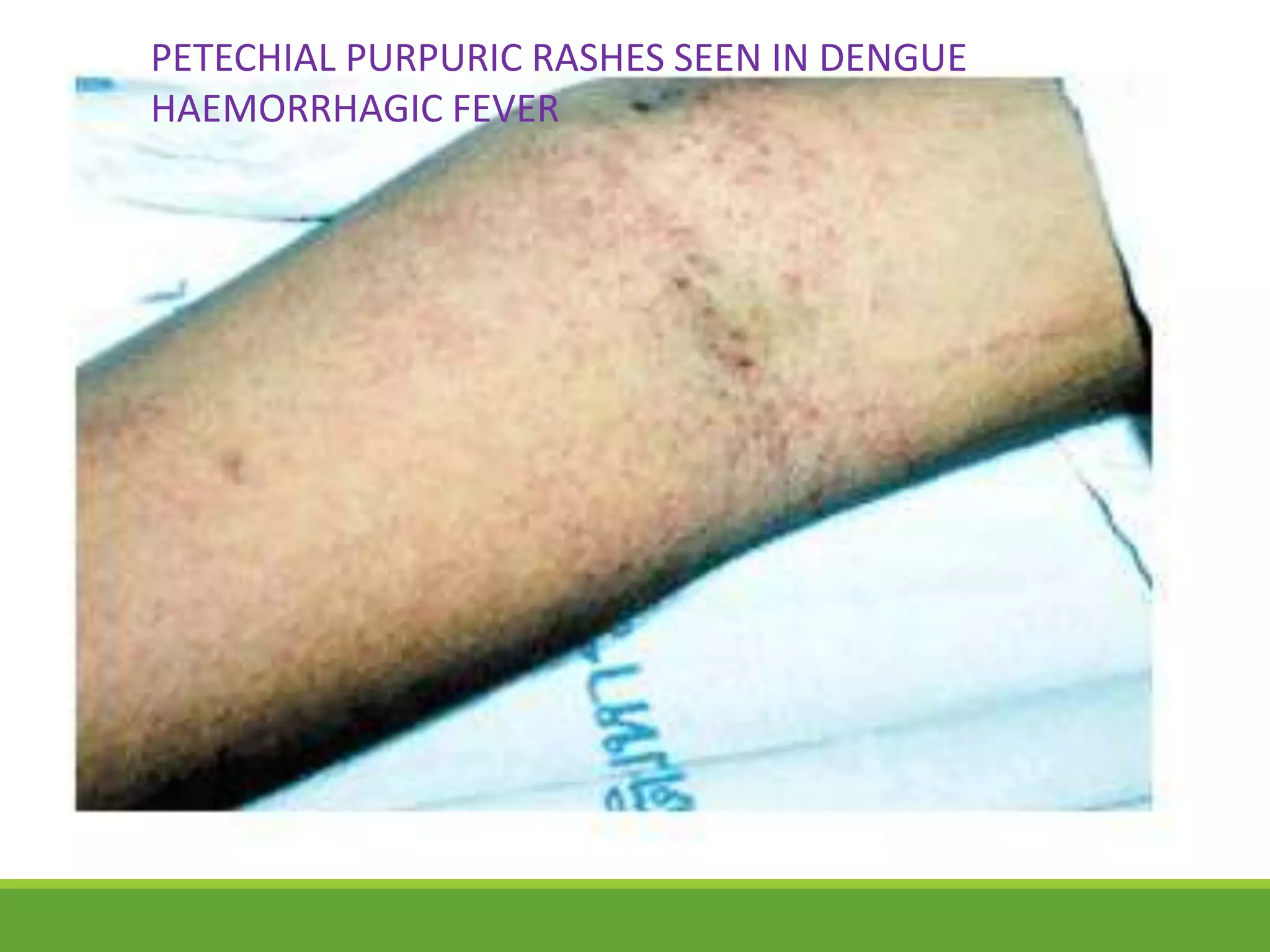
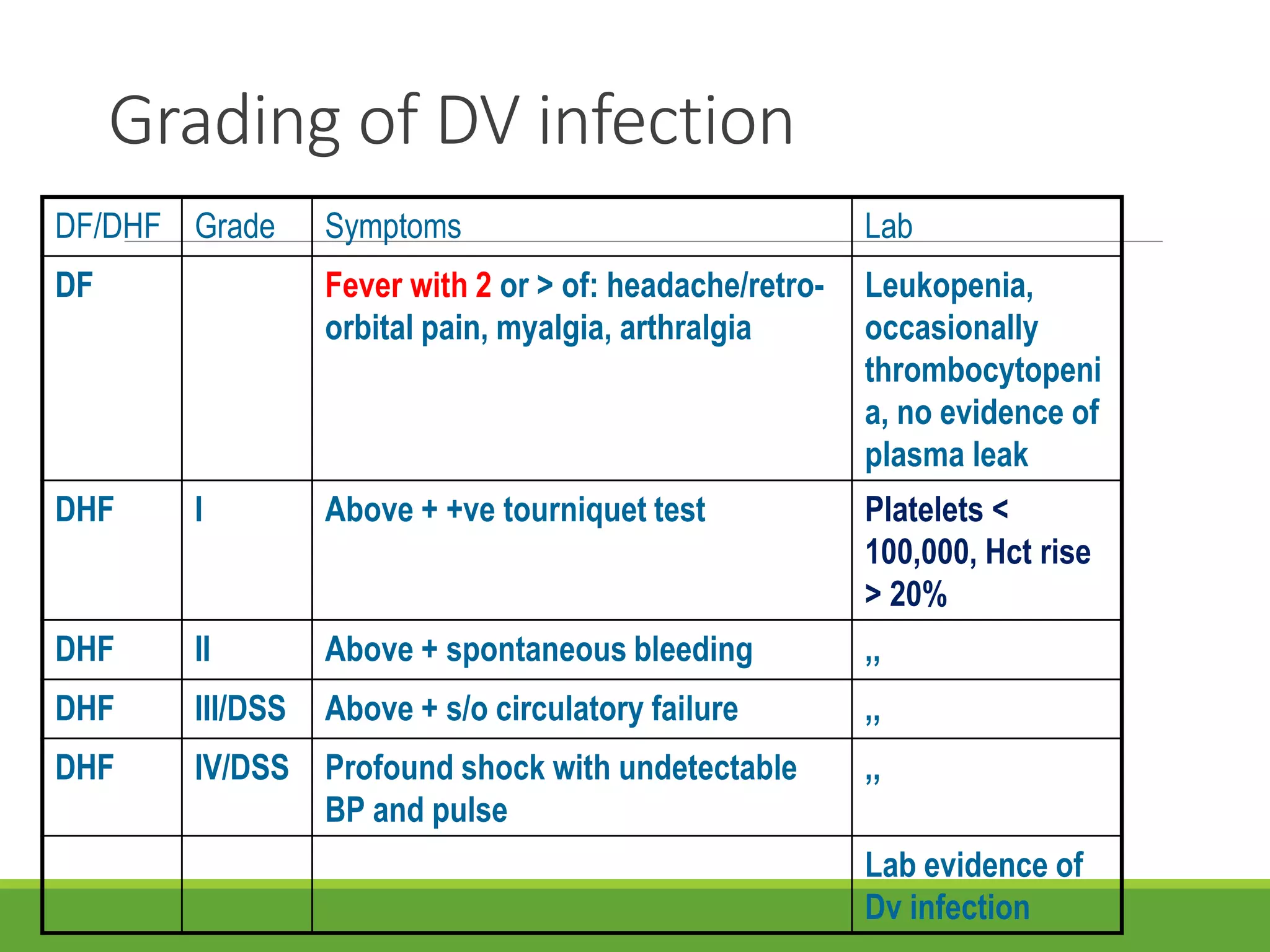
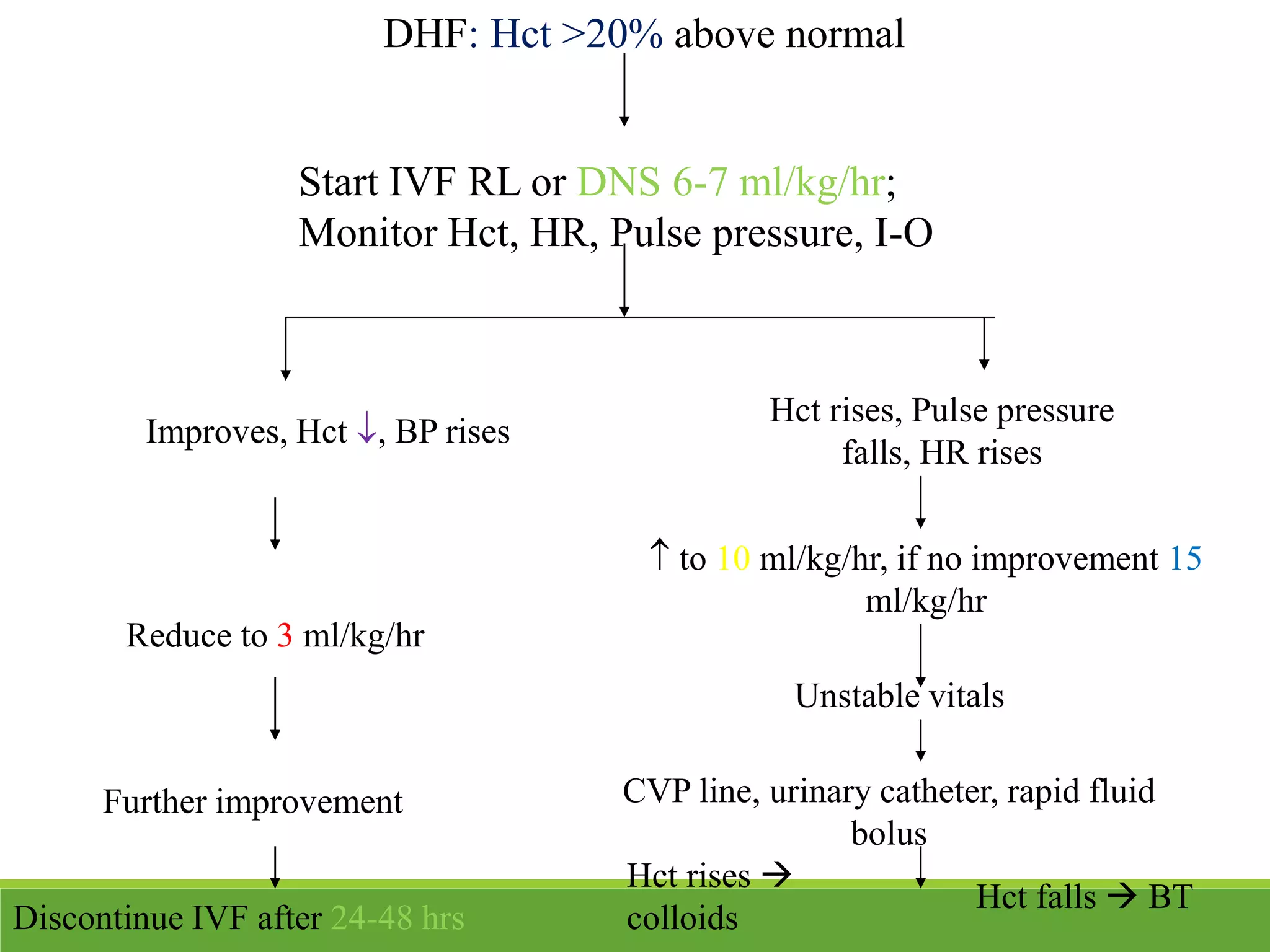
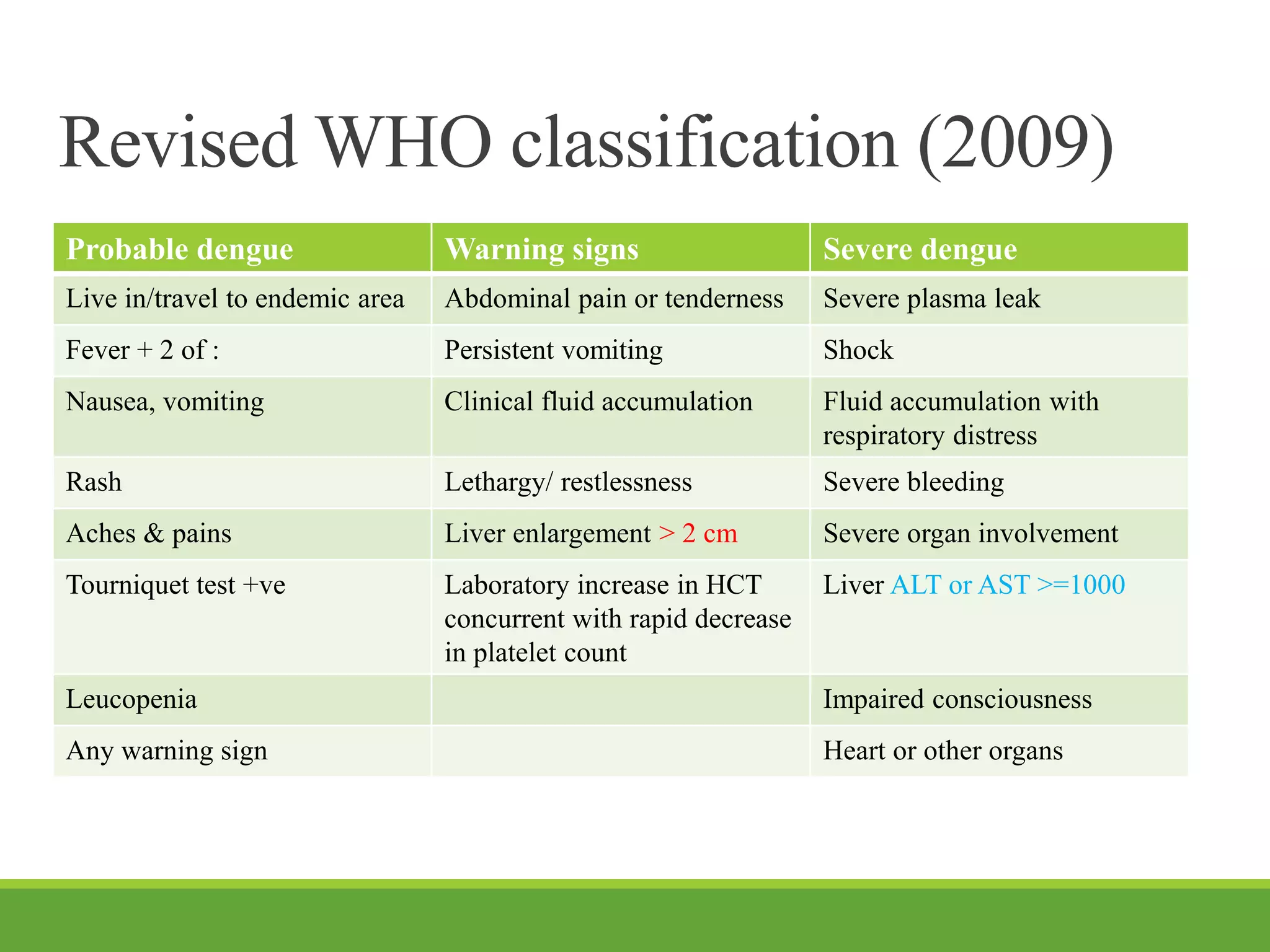
This document discusses dengue fever and dengue hemorrhagic fever (DHF). It is caused by a virus transmitted by Aedes mosquitoes. There are four serotypes of the virus. Secondary infection with a different serotype can cause DHF through antibody-dependent enhancement. DHF is characterized by fever, bleeding, thrombocytopenia, and plasma leakage. It can progress to dengue shock syndrome (DSS) with circulatory failure. Management of DHF involves fluid resuscitation to treat plasma leakage. Prevention focuses on eliminating mosquito breeding sites and using nets/repellents. A pediatric dengue vaccine also shows promise.