Day 1_Avanzini -Epilepsy Seizure and Classification.pptx
1.
EPILEPSY AND SEIZUE
CLASSIFICATION
GiulianoAvanzini
Istituto Neurologico C. Besta
Milano. Italy
21° San Servolo Advanced Epilepsy Course July 21-August 1 San Ser and new volo ,
Venice Italy
Bridging basic with Clinical Epileptology (8)
Contribution of non neuronal cells to epilepsy and new therapautic strategies
2.
“There are twoways of investigating
diseases, and two kinds of classification
corresponding thereto, the empirical and
the scientific. The former is to be illustrated
by the way in which a gardener classifies
plants, the latter by the way in which a
botanist classifies them.”
Johns Hughlings Jackson (1874)
On classification and on methods
of investigation” 1874
3.
The gardener arrangeshis plants as they
are fit for food, for ornament
etc. His object is the direct application of
knowledge The botanist classification (the
classification properly so-called) is rather
for the better organisation of existing
knowledge and for discovering the
relations of new facts, it is also of
utilitarian value, but not directly
Classifications reflect the state of
knowledge in a scientific field.
6.
Taxomic Rules
Classifiers: Reflectbiological classes conceptual
justification an directly impact
clinical managment (utilitarian justification):
1. Main seizure classes
2. Seizure types
3. Level of consciousness
Descriptors: represent key seizure characteristic which
aid seizure managment when combined with other
clinical data.
4. Semeiological features
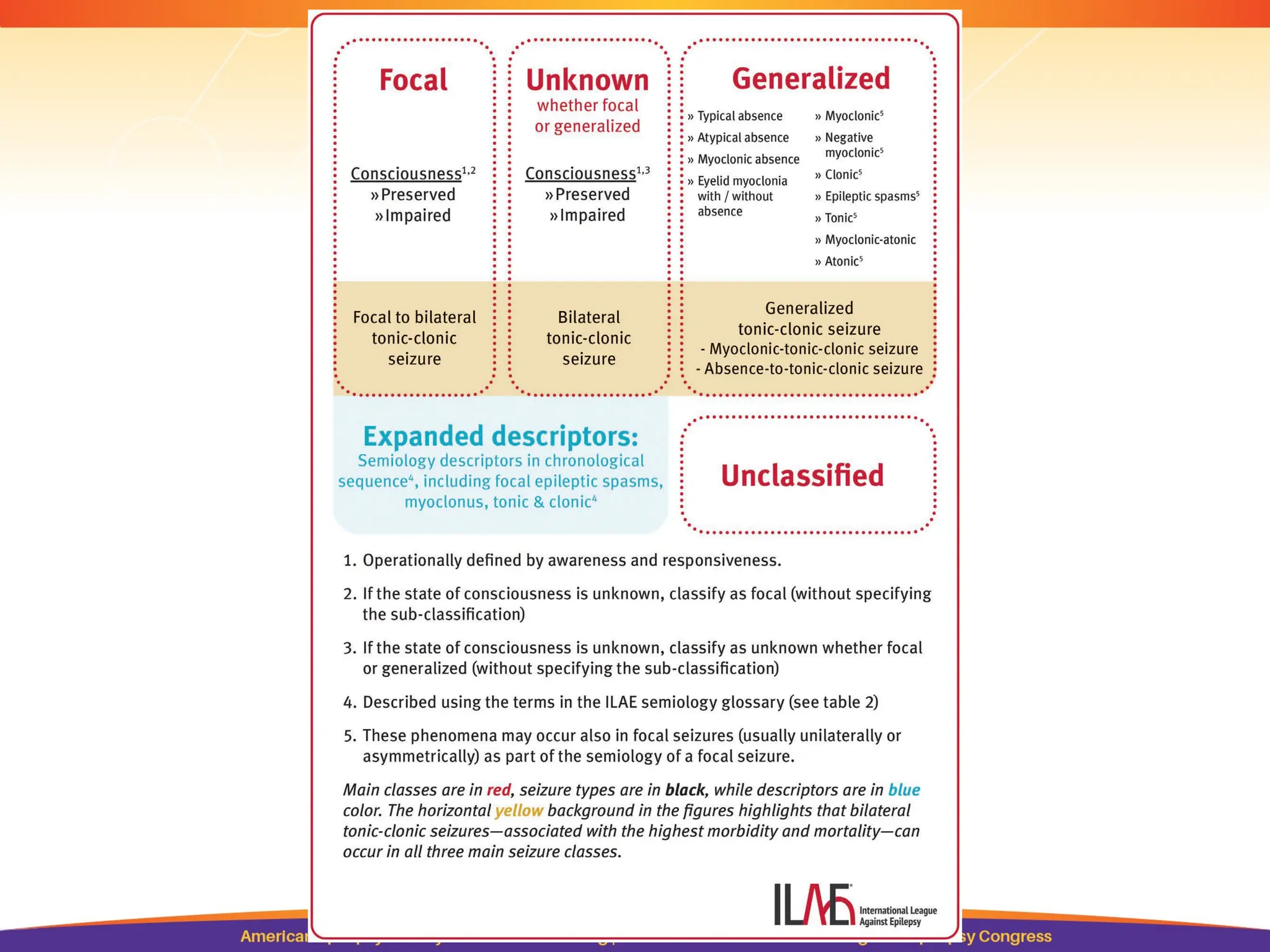
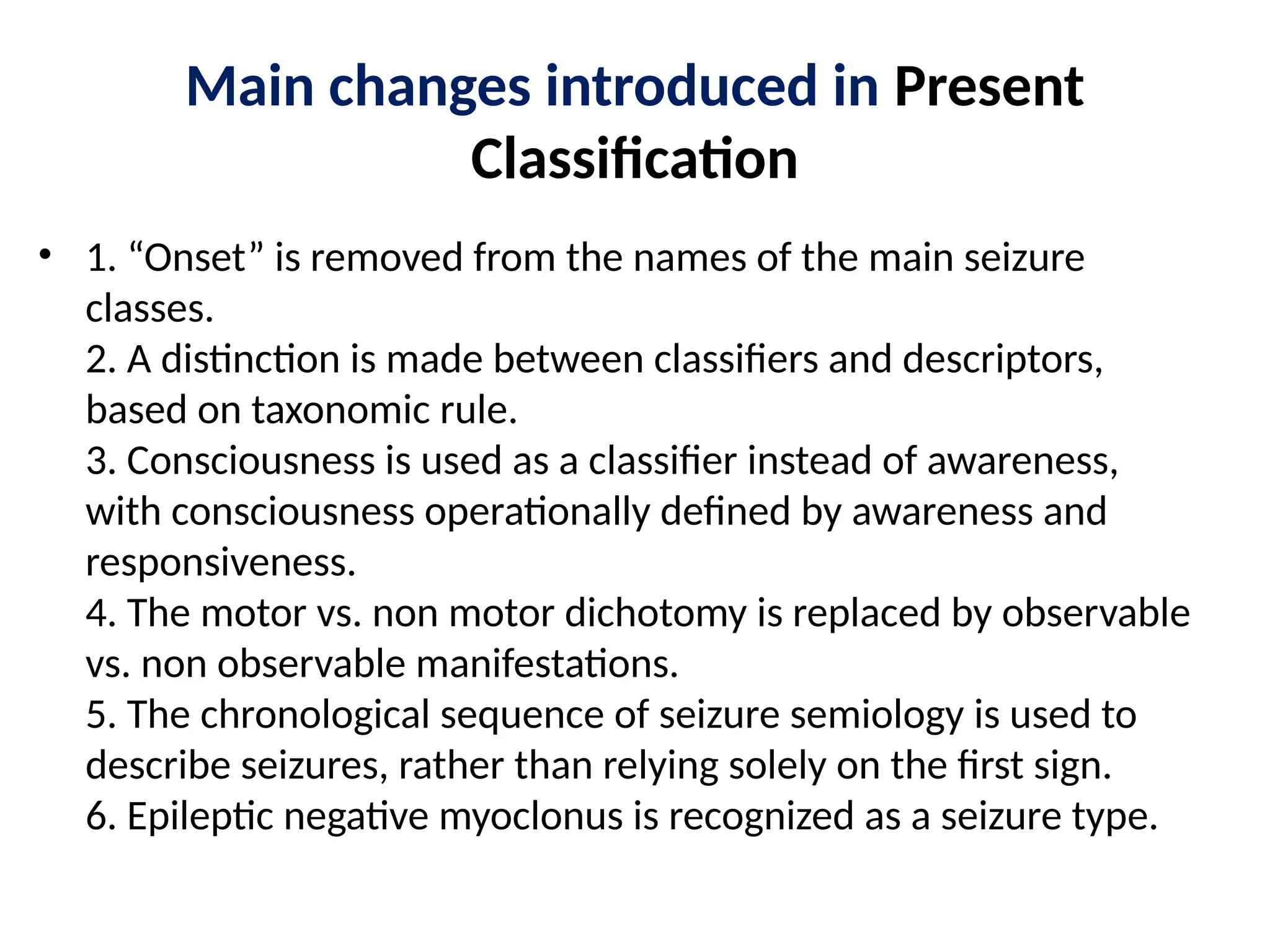
Main changes introducedin Present
Classification
• 1. “Onset” is removed from the names of the main seizure
classes.
2. A distinction is made between classifiers and descriptors,
based on taxonomic rule.
3. Consciousness is used as a classifier instead of awareness,
with consciousness operationally defined by awareness and
responsiveness.
4. The motor vs. non motor dichotomy is replaced by observable
vs. non observable manifestations.
5. The chronological sequence of seizure semiology is used to
describe seizures, rather than relying solely on the first sign.
6. Epileptic negative myoclonus is recognized as a seizure type.
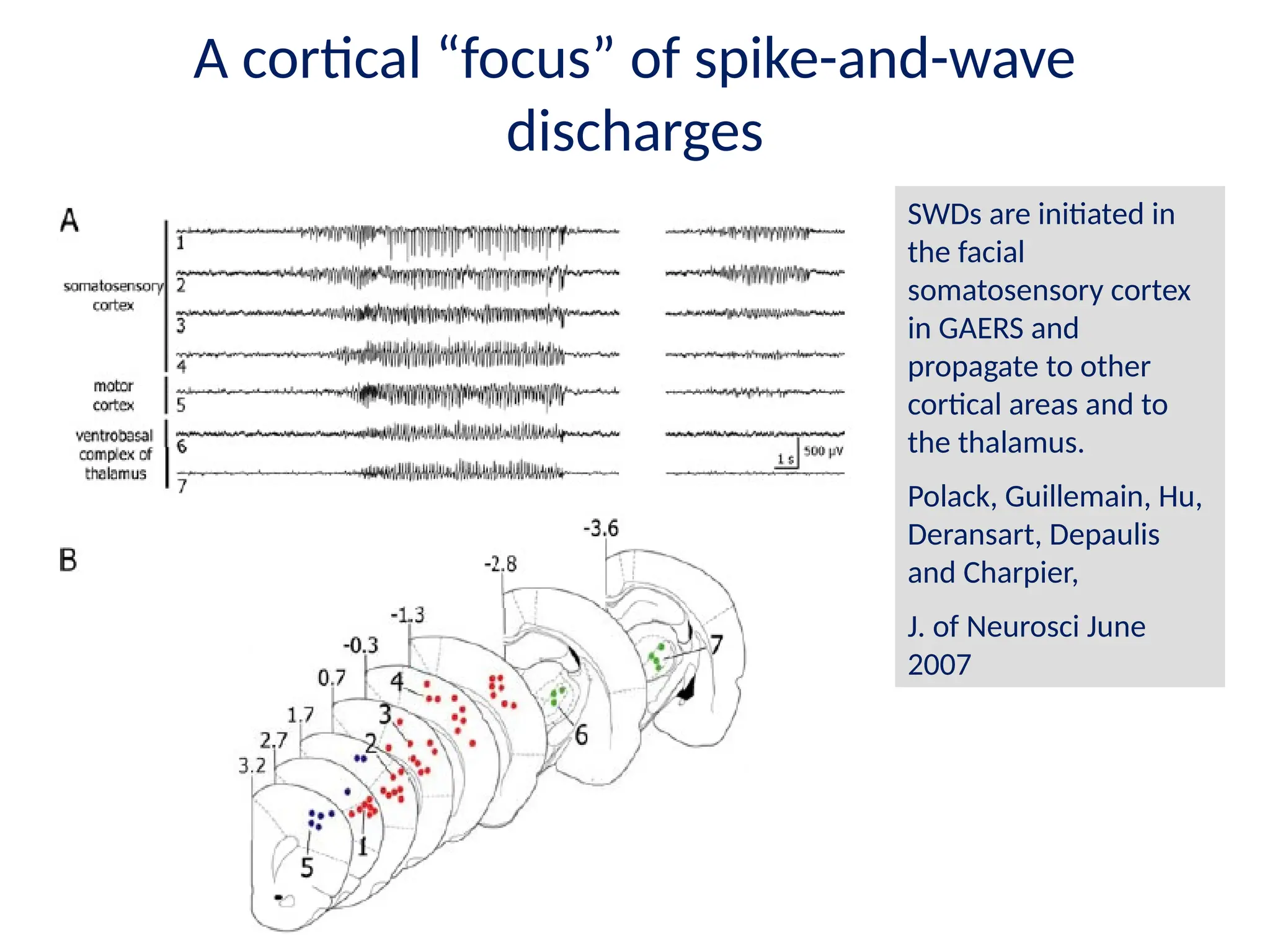
A cortical “focus”of spike-and-wave
discharges
SWDs are initiated in
the facial
somatosensory cortex
in GAERS and
propagate to other
cortical areas and to
the thalamus.
Polack, Guillemain, Hu,
Deransart, Depaulis
and Charpier,
J. of Neurosci June
2007
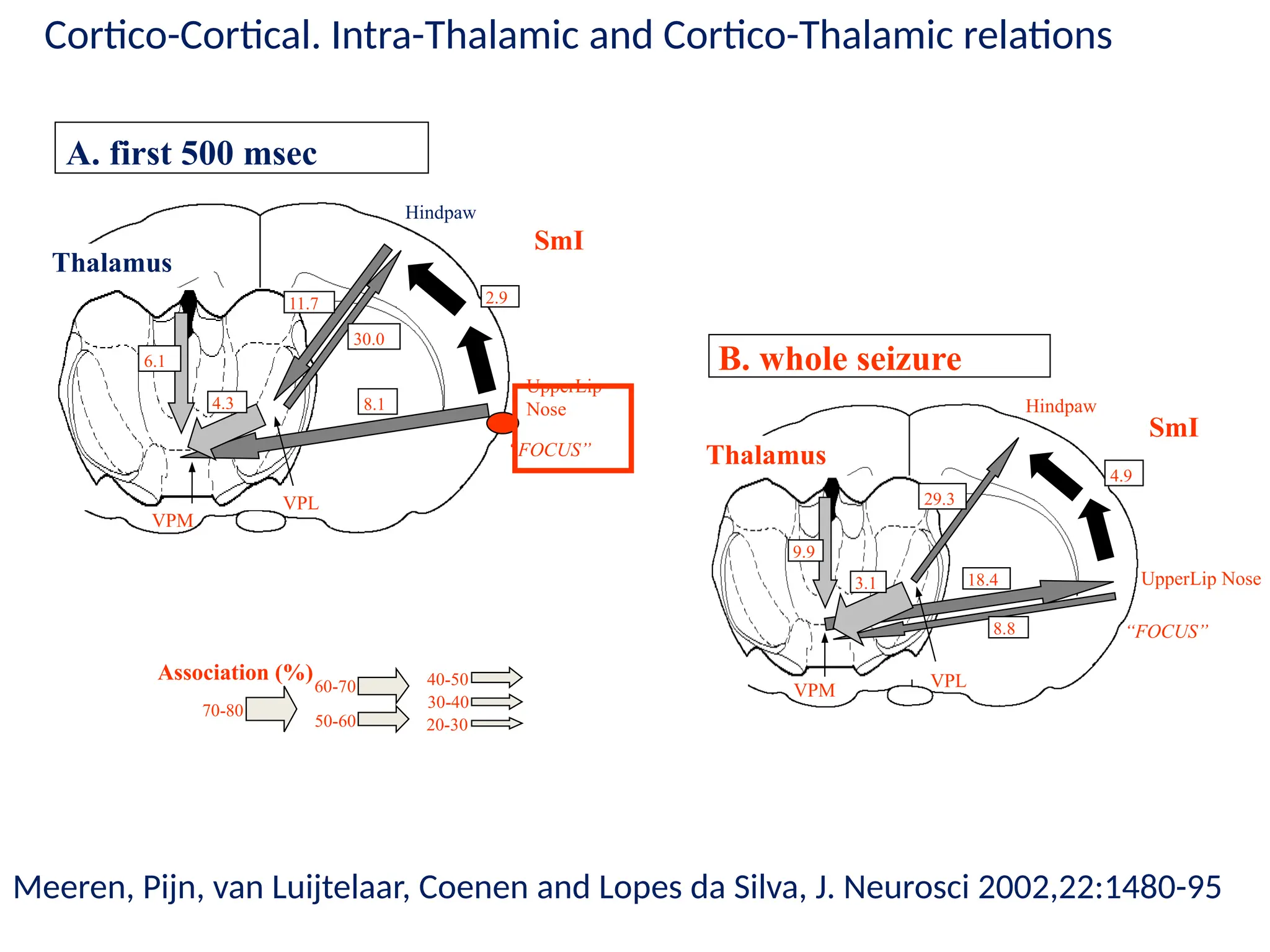
12.
VPM VPL
18.4
8.8
29.3
3.1
9.9
Hindpaw
UpperLip Nose
“FOCUS”
SmI
Thalamus
B.whole seizure
4.9
A. first 500 msec
VPM
2.9
8.1
11.7
30.0
4.3
6.1
VPL
UpperLip
Nose
“FOCUS”
SmI
Thalamus
Hindpaw
20-30
40-50
30-40
70-80
50-60
60-70
Association (%)
Meeren, Pijn, van Luijtelaar, Coenen and Lopes da Silva, J. Neurosci 2002,22:1480-95
Cortico-Cortical. Intra-Thalamic and Cortico-Thalamic relations
13.
CONSCIOUSNESS
• Consciousness: awarenessof self, of his own mental
contents and of the objects to which it turns (Descartes
Kant, Hegel, Jaspers, Husserl)
• The source of every type of human experience or
knowledges is somebody’s content of consciousness and is
therefore not accessible to any type of objectve analysis
(Hartwig Kuhlenbeck)
• If we metaphorically describe consciousness as the only
window trough which we can observe the world then when
we look through this window we cannot see it (Peter Gloor)
• You are conscious when you are actively interacting with
the world (Alva Noe)
14.
EPILEPTIC SEIZURES &EPILEPSIES
• An epileptic seizure is a transient occurrence of
signs and/or symptoms due to abnormal
excessive or synchronous neuronal activity in
the brain.
• Epilepsy is a chronic condition of the brain
characterized by an enduring propensity to
generate epileptic seizures, and by the
neurobiological, cognitive, psychological, and
social consequences of this condition.
15.
ILAE EPILEPSY (EPILEPTICSYNDROMES)
CLASSIFICATION
IDIOPATHIC SYMPTOMATIC
Generalized Generalized
Partial/localization related Partial/localization related
16.
IDIOPATHIC PARTIAL EPILEPSIES
•The concept of benign partial epilepsies (BPE) that
emerged in the late fifties and early sixties (Bancaud et al
1958, Nayrac and Beaussard 1958, Faure and Loiseau
1960, Lombroso 1967) introduced a novel view in the
pathophysiological concepts founded by John Hughlings
Jackson.
• Besides epilepsies due to focal epileptogenic lesions and
“functional” epilepsies due to a dysfunction of diffusely
projecting “centrencephalic” structures a new category of
epilepsies due to a dysfunction affecting a cortical area in
which no evidence of lesion was demonstrable was then
established.
17.
These localization-related epilepsiescould
not be attributed to an epileptic focus in
an anatomic sense but rather to an age-
related hyperexcitable condition of a given
cortical region, most frequently the
sensory-motor and visual ones, with no
detectable structural alteration.
18.
EPILEPSY SYNDROME
A complexof signs and symptoms that
define a unique epilepsy condition
with different etiologies. This must
involve more than just the seizure
type; thus frontal lobe seizures per se,
for instance, do not constitute a
syndrome.
19.
Idiopathic epilepsy syndrome:A syndrome that
is only epilepsy, with no underlying structural
brain lesion or other neurologic signs or
symptoms. These are presumed to be genetic
and are usually age dependent.
Symptomatic epilepsy syndrome: A syndrome
in which the epileptic seizures are the result of
one or more identifiable structural lesions of the
brain.
Probably symptomatic or cryptogenic epilepsy
syndrome: syndromes that are believed to be
symptomatic, but no etiology has been
identified.
20.
CURRENT CLASSIFICATION OFTHE EPILEPSIES (1)
IDIOPATHIC EPILEPSIES
GENERALIZED
• Benign neonatal (familial) seizures
• Benign myoclonic epilepsy in infancy
• Childhood absence epilepsy
• Juvenile myoclonic epilepsy
• Juvenile absence epilepsy
• Generalized epilepsy with tonic-clonic seizures (on
awakening, during sleep, at random)
PARTIAL
• Benign childhood epilepsy with centro-temporal spikes
• Childhood epilepsy with occipital paroxysms
21.
SYMPTOMATIC/CRYPTOGENIC EPILEPSIES
GENERALIZED
• earlyinfantile encephalopathies with suppression
burst
• infantile spasms (West syndrome)
• severe myoclonic epilepsy in infancy
• Lennox-Gastaut syndrome
Progressive epileptogenic encephalopathies
(ceroidolipofuscinoses, sialidoses, Lafora disease, Unverricht-
Lundborg disease etc.)
PARTIAL
• mesial temporal lobe epilepsy
• others (defined according to the location of the
epileptogenic zone)
CURRENT CLASSIFICATION OF THE EPILEPSIES (2)
22.
SITUATION RELATED EPILEPSIES:
•Reflex epilepsies
• Febrile seizures
STATUS EPILEPTICUS
• Non age related status epilepticus
• Rare age-related syndromes
presenting with electrical or clinical
status
CURRENT CLASSIFICATION OF THE EPILEPSIES (3)