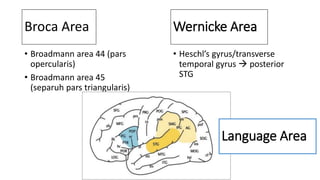
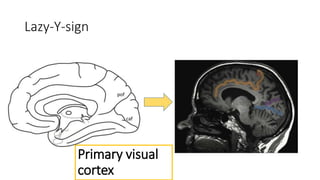
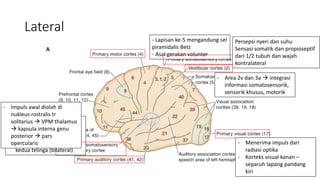
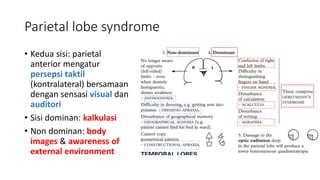
Dokumen ini membahas anatomi dan fungsi kortikal, termasuk area-area Brodmann dan sindrom otak regional yang terkait dengan berbagai lobus otak seperti frontal, parietal, temporal, dan occipital. Setiap lobus dijelaskan dengan gejala dan gangguan terkait, seperti afasia di daerah Wernicke dan sindrom Foster Kennedy. Penekanan pada interaksi antara fungsi motorik, sensori, dan proses kognitif di berbagai area otak akan menjelaskan dampak dari lesi yang terjadi.