

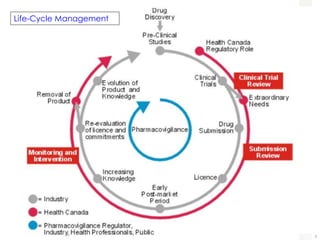
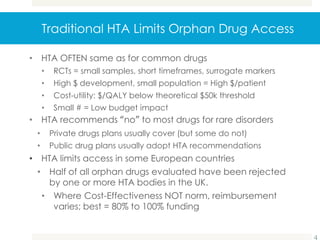
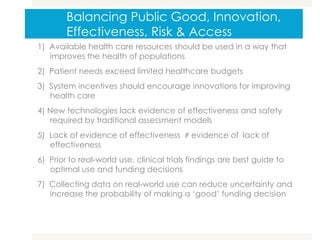

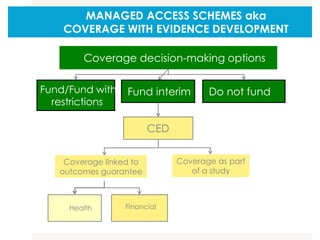
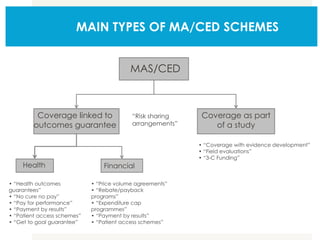
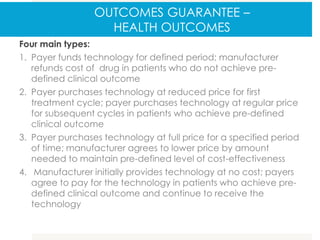
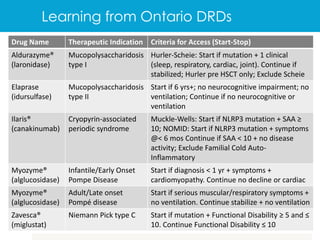


The document discusses Canada's orphan drug regulatory framework and opportunities to improve access to rare disease drugs across Canada. It advocates for a life-cycle approach and managed access schemes where drugs are approved with evidence collection requirements. Traditional health technology assessment limits orphan drug access by rejecting drugs that are not cost-effective based on small clinical trials. The document recommends performance-based managed access programs with national guidelines and risk-sharing between provinces, patients, and companies to improve access while collecting long-term evidence on benefits, harms, and costs.















































































