Download to read offline

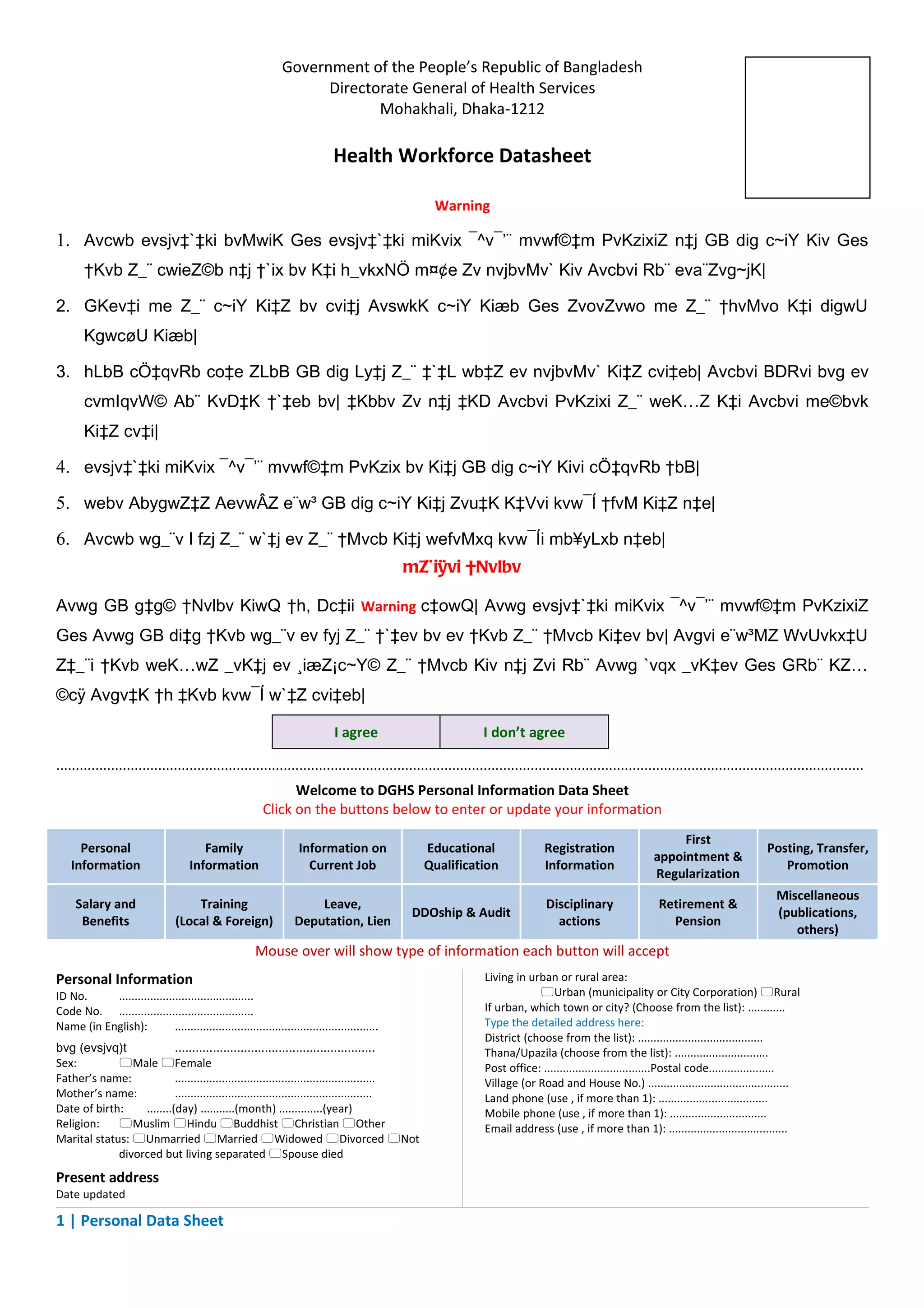




This document provides guidelines for accessing and updating personal information stored in a government health workforce database in Bangladesh. It warns that providing inaccurate information or sharing private details could result in legal penalties. Users must agree to only access the database when necessary and keep all information confidential in order to view their records.















































