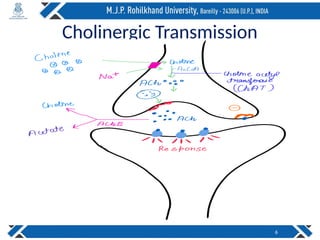
The document discusses cholinergic transmission and receptors, detailing how acetylcholine (ACh) is synthesized, released, and its actions mediated via nicotinic and muscarinic receptors. It explains the biochemical impacts of ACh, including its role in neural functions and muscle contraction, and outlines different muscarinic receptor subtypes (M1-M5) and their functions. Lastly, it highlights the involvement of G-proteins in receptor signaling and the clinical implications of drugs that affect cholinergic transmission.