Download to read offline


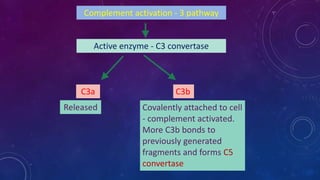
![• Histamine stored in mast cell granules are release by
degranulation in response to various stimuli:
1. Physical injuries such as trauma cold heat
2. Antibody mediated hypersensitivity allergic reaction
3. Complement products C3a, C5a [ anaphylatoxin ]
4. Neuropeptides [substance P]
5. Cytokines [ interleukin 1 interleukin 8]](https://image.slidesharecdn.com/chemicalmediatorsahscls-231127071203-2f7cae1e/85/chemical-mediators-AHS-cls-pptx-8-320.jpg)


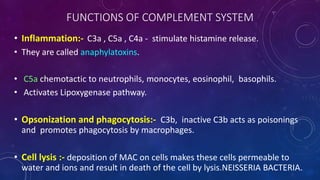
![C5 convertase
Cleaves C5 into
C5a released C5b - attached to cell surface
C5b binds to late
components(C6 to C9). Thus
forming membrane attack
complex[composed of
multiple C9 molecules].](https://image.slidesharecdn.com/chemicalmediatorsahscls-231127071203-2f7cae1e/85/chemical-mediators-AHS-cls-pptx-34-320.jpg)
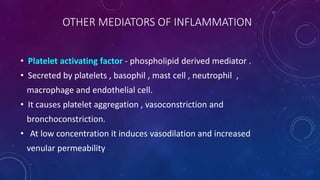
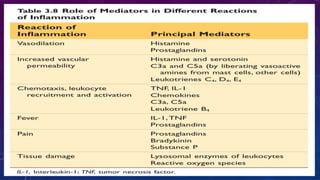


Chemical mediators initiate and regulate inflammatory reactions. They can be cell-derived or plasma-derived and include vasoactive amines, lysosomal components, platelet activating factor, cytokines, arachidonic acid metabolites, kinins, components of the clotting, fibrinolytic, and complement systems. Mediators are short-lived and stimulate the production of other mediators. They cause effects like increased vascular permeability, vasodilation, chemotaxis, and pain.



































































