Overview of DM
DM is not a single disease entity but rather a
group of metabolic disorders sharing the common
underlying feature of hyperglycemia
Hyperglycemia in DM results from
Defects in insulin secretion, insulin action, or,
most commonly, both
It affects more than 120 million people world-wide
It is estimated that it will affect 220 million by
the yr 2020
4
5.
Overview of DM…
Type 1 DM
An autoimmune disease in which islet
destruction is caused primarily by
• T lymphocytes reacting against as yet poorly
defined β-cell antigens, resulting in a
reduction in β-cell mass
Genetic susceptibility & environmental influences
play important roles in the pathogenesis
Most commonly develops in childhood, becomes
manifest at puberty & progressive with age
5
6.
Overview of DM…
Type 2 DM
Like Type 1 DM, the pathogenesis of type 2 DM
remains enigmatic
Environmental influences, such as a sedentary
life style & dietary habits have a role
Genetic factors are more important than in type 1
DM
The 2 metabolic defects that characterize type 2
DM
• Insulin resistance
• ↓ed ability of peripheral tissues to respond to insulin
6
7.
Overview of DM…
β-cell dysfunction
• Manifested as inadequate insulin secretion in
the face of insulin resistance & hyperglycemia
NB: In most cases, insulin resistance is the 10
event
& followed by ↑sing degrees of β-cell dysfunction
Type 3 DM
The type 3 designation refers to multiple other
specific causes of an elevated blood glucose:
pancreatectomy, pancreatitis, non-pancreatic
diseases, drug therapy, etc
7
8.
Overview of DM…
Type 4 DM
Gestational diabetes (GDM) is defined as any
abnormality in glucose levels noted for the 1st
time
during pregnancy
During pregnancy, the placenta & placental hormones
create an insulin resistance that is most pronounced in
the last trimester
Risk assessment for DM is suggested starting at the 1st
prenatal visit
High-risk women should be screened immediately
Screening may be deferred in lower-risk women until the
24th to 28th wk of gestation
8
What are therisksfactorsassociatedwith
GDM?
• Althoughany womancan develop GDMduringpregnancy,
someof thefactors thatmay↑the riskinclude thefollowing:
• Overweightor obesity
• Family history of DM
• Havinggivenbirth previously to avery largeinfant,astill
birth,ora childwitha birthdefect
• Age (women who are older than25areata greater risk for
developing GDM than youngerwomen)
• Race (womenwho areAfrican-American,American Indian,
AsianAmerican,Hispanic/Latino, or PacificIslander havea
higher risk)
• Prediabetes
9.
Types of AntidiabeticAgents
A. Injectable antidiabetic agents: Insulins
B. Oral antidiabetic agents
Both aim to produce normal blood glucose states
9
10.
A. Insulin preparations:
Role of Insulin
The actions of insulin on cells include:
• Increased glycogen synthesis
• Increased fatty acid synthesis
• Increased esterification of fatty acids
• Decreased proteinolysis
• Decreased lipolysis
• Decreased gluconeogenesis
• Increased amino acid uptake
• Increased potassium uptake
10
11.
Insulin preparations
4principal types of injected insulins are available:
Rapid-acting→ very fast onset & short duration
Short-acting → rapid onset of action
Intermediate-acting →slow onset of action
Long-acting: → slow onset of action
11
12.
Insulin preparations …
Rapid acting
Most rapid onset of action (5-15 min)
Shorter duration
• Insulin aspart, Insulin lispro
Short acting
Regular insulin
The only insulin product that can be given by IV bolus,
IV infusion, or even IM
NB: Injected rapid acting & short-acting insulins are
dispensed as clear solutions at neutral pH & contain small
amts of zinc to improve their stability and shelf life
12
13.
Insulin preparations …
Intermediate acting
Isophane insulin suspension (also called NPH)
Insulin zinc suspension (also called Lente)
Both have a cloudy appearance
Slower in onset & more prolonged duration than
endogenous insulin
Long acting
Glargine: Clear, colorless solution
Extended insulin Zn suspension (Ultralente)
• White, opaque solution
13
15
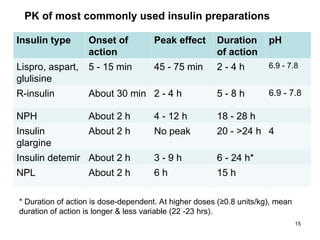
PK of mostcommonly used insulin preparations
Insulin type Onset of
action
Peak effect Duration
of action
pH
Lispro, aspart,
glulisine
5 - 15 min 45 - 75 min 2 - 4 h 6.9 - 7.8
R-insulin About 30 min 2 - 4 h 5 - 8 h 6.9 - 7.8
NPH About 2 h 4 - 12 h 18 - 28 h
Insulin
glargine
About 2 h No peak 20 - >24 h 4
Insulin detemir About 2 h 3 - 9 h 6 - 24 h*
NPL About 2 h 6 h 15 h
* Duration of action is dose-dependent. At higher doses (≥0.8 units/kg), mean
duration of action is longer & less variable (22 -23 hrs).
16.
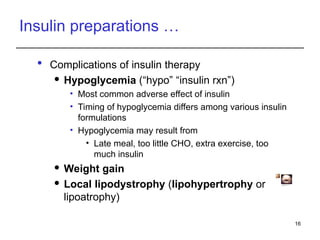
Insulin preparations …
Complications of insulin therapy
Hypoglycemia (“hypo” “insulin rxn”)
• Most common adverse effect of insulin
• Timing of hypoglycemia differs among various insulin
formulations
• Hypoglycemia may result from
• Late meal, too little CHO, extra exercise, too
much insulin
Weight gain
Local lipodystrophy (lipohypertrophy or
lipoatrophy)
16
Fig. lipoatrophy
Fig: Abdomen siteof injection showing
hypertrophyand scars
17.
B. Oral AntidiabeticAgents
Used for type 2 DM
Tx for type 2 DM includes lifestyle modifications
Diet, exercise, smoking cessation, wt loss
Oral antidiabetic agents may not be effective
unless the pt also makes behavioral or lifestyle
changes
17
18.
a) Sulfonylureas
Drugsincludes: glibenclamide, glipizide, glimepride
Stimulate release of insulin from pancreas to lower
blood glucose
Must have functioning pancreatic beta cells
Side effects: Hypoglycemia, N, skin reactions
(including photosensitivity), & abnormal liver
function tests, Wt gain
Administer 30 minutes before meals
18
Fig. One model of control of insulin release from the pancreatic beta
cell by glucose and by sulfonyl urea drugs
19.
b) Biguanide: metformin
Increases use of glucose by muscle & fat cells
Decreases hepatic glucose production
Decreases intestinal absorption of glucose
Most common SEs of metformin are GI, including
A metallic taste in the mouth, mild anorexia, N, D,
abdominal discomfort
Lactic acidosis is an uncommon SE
C/I in serious hepatic or renal impairment or other
conditions that may ↑ lactate production- potentially
fatal lactic acidosis
Administer with meals
19
– In pts with renal disease, alcoholism, hepatic
disease, or
– Conditions predisposing to tissue anoxia (eg,
chronic cardiopulmonary dysfunction)
– b/c of the increased risk of lactic acidosis
induced by this drug
Metformin is C/I:
20.
c) Meglitinides
Includes:Repaglinide & nateglinide
Similar action to sulfonylureas- stimulate
pancreatic secretion of insulin
Short-acting glucose-lowering drugs given alone or
in combination with metformin
Efficacy when taken just 15 minutes before meals
A duration of effect of no more than 3 hrs
Similar risk for wt gain as sulfonylureas but
possibly less risk of hypoglycemia
20
21.
d) Glitazones (Thiazolidinediones)
Includes: Rosiglitazone, pioglitazone
Reduce insulin resistance in the tissues
↑ insulin sensitivity by acting on adipose, Ms, &
liver to ↑glucose utilization & ↓ glucose production
Use cautiously in pts with CHF: ↑ plasma volume &
may cause fluid retention
Administer with meals
21
22.
e) Alpha-Glucosidase Inhibitors
Includes: Acarbose, Miglitol
Inhibit digestive enzymes in GIT (such as sucrase,
maltase, amylase) responsible for release of glucose
from consumed CHO, so absorption is delayed
C/I in inflammatory or malabsorptive intestinal
disorders
Administer just before meals
22
23.
Antidiabetic Agents: Nursing
Implications
Before giving any drugs that alter glucose levels,
obtain & document:
A thorough history
Vital signs
Blood glucose level
Potential complications & drug interactions
23
24.
Nursing Implications…
Beforegiving any drugs that alter glucose levels:
Assess the pt’s ability to consume food
Assess for N or V
Hypoglycemia may be a problem if antidiabetic
agents are given & the pt does not eat
If a pt is NPO for a test or procedure, consult
physician to clarify orders for antidiabetic drug
therapy
24
25.
Nursing Implications…
Keepin mind that overall concerns for any diabetic
pt ↑when the pt:
Is under stress
Has an infection
Has an illness or trauma
Is pregnant
Thorough pt education is essential regarding:
Disease process
Diet & exercise recommendations
Self-administration of insulin or oral agents
Potential complications
25
26.
Nursing Implications…
Wheninsulin is ordered, ensure:
Correct route
Correct type of insulin
Timing of the dose
Correct dosage
Insulin order & prepared dosages are second-
checked with another nurse
26
27.
Nursing Implications…
Insulin
Check blood glucose level before giving insulin
Roll vials b/n hands instead of shaking them to mix susp
Ensure correct storage of insulin vials
ONLY insulin syringes, calibrated in units, are to be used to
measure & give insulin
Ensure correct timing of insulin dose with meals
When drawing up 2 types of insulin in one syringe, always
withdraw the regular insulin first
Provide thorough pt education regarding self-administration of
insulin injections, including timing of doses, monitoring blood
glucoses, & injection site rotations
27
28.
Nursing Implications…
Oralantidiabetic agents
Always check blood glucose levels before giving
Usually given 30 minutes before meals
Alpha-glucosidase inhibitors are given with the
first bite of each main meal
Metformin is taken with meals to reduce GI effects
28
29.
Nursing Implications…
Assessfor signs of hypoglycemia
If hypoglycemia occurs:
Give glucagon
Have the pt eat glucose tabs or gel, corn syrup,
honey, fruit juice or non-diet soft drink
Or have the pt eat a small snack such as
crackers or half a sandwich
29
30.
Nursing Implications…
Monitorblood glucose levels
Monitor for therapeutic response
↓ in blood glucose levels to the level
prescribed by physician
Watch for hypoglycemia & hyperglycemia
Measure hemoglobin A1c to monitor long-term
compliance to diet & drug therapy
30
Overview
The thyroidgland is located in the neck in front of
the trachea
This highly vascular gland manufactures &
secretes 2 hormones: thyroxine (T4) &
triiodothyronine (T3)
Iodine is an essential element for the manufacture
of both of these hormones
The activity of the thyroid gland is regulated by
thyroid-stimulating hormone, produced by the
anterior pituitary gland
32
33.
Overview
Two diseasesare related to the hormone-producing
activity of the thyroid gland:
Hypothyroidism—a decrease in the amt of
thyroid hormones manufactured & secreted
Hyperthyroidism—an ↑ in the amt of thyroid
hormones manufactured & secreted
• A severe form of hyperthyroidism, called
thyrotoxicosis or thyroid storm, is
characterized by high fever, extreme
tachycardia, & altered mental status
33
34.
A. Drugs forHypothyroidism
Thyroid hormone influences many systems &
processes in the body, including the following:
Metabolic: energy levels, body temp, wt, lipids,
appetite
CV: HR, heart rhythm, BP, fluid distribution
Skin & hair: composition, thickness, texture
GI: motility
Musculoskeletal: bone growth, tendon reflexes
Hematologic: erythropoiesis
Reproductive: ovulation & spermatogenesis
34
35.
Drugs for Hypothyroidism…
Thyroid hormone preparations include:
Levothyroxine Na
Others: Liothyronine, liotrix, thyroid (desiccated)
Levothyroxine Na
Dosage Forms: Tabs, injection
Indication: Hypothyroidism from any cause
35
36.
Drugs for Hypothyroidism…
Levothyroxine Na…
Adverse reactions: most common
• Fatigue, ↑ed appetite, wt loss, heat intolerance,
hyperhidrosis
Adverse reactions: rare/severe/important
• Hair loss, menstrual irregularities, nervousness,
irritability, insomnia
C/Is:
• Caution must be exercised in conditions in which
tachycardia is dangerous (CAD, aortic stenosis,
mitral stenosis)
36
37.
Drugs for Hypothyroidism…
Levothyroxine Na: Nursing considerations
The Tx is initiated slowly (with small doses) &
gradually increased
Store medications in cool dark place
Take complete nursing history
Note if the client is taking antidiabetic drugs &
document
Take baseline ECG. then at regular intervals
Monitor thyroid function closely
Observe client for side effects
37
38.
Drugs for Hypothyroidism…
Levothyroxine Na: Nursing considerations…
Monitor PT & PTT closely since the drug ↑
hypoprothrombinemia
Monitor HR & BP closely for cardiac pts
Instruct the client to report SEs e.g. wt loss &
nervousness to physician
Have dietitian counsel clients regarding diet
according to the energy demands
Female client should record menstrual irregularities
Encourage the client to keep follow-up visits
38
39.
B. Drugs forHyperthyroidism
Drugs for Hyperthyroidism
Thionamides: propylthiouracil (PTU) &
methimazole
Radioactive Iodine (131
I)
Nonradioactive Iodine: Strong Iodine Solution
(Lugol's Solution), Na Iodide (IV), K Iodide
Beta blockers
• can suppress tachycardia & other symptoms
of Hyperthyroidism
39
40.
Drugs for Hyperthyroidism...
1.Thionamides: propylthiouracil (PTU)
Act primarily by blocking the synthesis of thyroid
hormone
Require about 3 to 12 wks to exert their effects b/c
of the thyroid precursors of thyroid synthesis that are
stored inside the thyroid gland
Adverse Effects:
• The most common (in 6% to 10% of pts) are skin rash,
fever, & arthralgia (sore joints)
• Serious, Rare Side Effects : Agranulocytosis,
Hepatotoxicity, Vasculitis
40
41.
Drugs for Hyperthyroidism...
PTU has 4 therapeutic applications in
hyperthyroidism:
Reduction of thyroid hormone production in
Graves' disease
Control of hyperthyroidism until the effects of
radiation on the thyroid become manifest
Suppression of thyroid hormone production prior
to subtotal thyroidectomy
Treatment of thyrotoxic crisis
41
42.
Drugs for Hyperthyroidism...
PTU: Nursing implication
Obtain serum levels of free T3 & free T4 as a
baseline data
Use with caution during pregnancy & lactation
Instruct the pt to take PTU at regular intervals
around-the-clock (usually every 8 hrs)
Evaluate Tx by monitoring for wt gain, ↓ed HR, &
other indications that levels of thyroid hormone have
declined
Inform pts about early signs of agranulocytosis
(fever, sore throat), & instruct them to notify the
physician if these develop
42
43.
Drugs for Hyperthyroidism...
2.Radioactive iodine (131
I)
Destroys the thyroid gland via radiation
Indications: Hyperthyroidism, Thyroid cancer
Adverse effects:
• Hypothyroidism: Almost all pts require lifelong thyroid
replacement after radioactive ablation
• Sialadenitis: Inflammation of the salivary glands
occurs b/c of uptake of 131
I
• Salivary damage can result in xerostomia (dry
mouth), altered taste, ↑ed dental caries, & pain
• Cancer: Although very small, a risk of cancer arises
from the radiation from the 131
I
43
44.
Drugs for Hyperthyroidism...
C/Is:
Absolutely C/I in pregnancy pregnancy &
lactation
• Furthermore, pregnancy must be avoided for
6 months following administration of 131
I
Relatively contraindicated in children: There is a
small risk of cancer
44
45.
Drugs for Hyperthyroidism...
3.Strong iodine solution (lugol's solution)
Therapeutic Goal:
• Suppression of thyroid hormone production
in preparation for subtotal thyroidectomy
• Also used to suppress thyroid hormone
release in pts experiencing thyroid storm
Baseline Data: Obtain tests of thyroid function
Administration:
• Advise pts to dilute strong iodine solution with
fruit juice or some other beverage to increase
palatability
45
46.
Drugs for Hyperthyroidism...
Mild Toxicity
Inform pts about Sx of iodism (brassy taste, burning
sensations in the mouth, soreness of gums & teeth), &
instruct them to discontinue Tx & notify the prescriber if
these occur
Symptoms fade upon drug withdrawal
Severe Toxicity
Iodine solution can cause corrosive injury to the GIT
Instruct pts to discontinue the drug & notify the prescriber
immediately if severe abdominal distress develops
Tx includes gastric lavage & giving Na thiosulfate
46
Editor's Notes
#5 There is a long preclinical period (up to 9 -13 yrs) marked by the presence of immune markers when β-cell destruction is thought to occur
Hyperglycemia occurs when 80% - 90% of β- cells are destroyed
It generally develops in childhood or early adulthood & results from immunemediated destruction of pancreatic β-cells, resulting in an absolute deficiency of insulin
Accounts for 5%-10% of all diabetes cases
#6 , as will become evident when obesity is considered
#7 Unlike type 1 DM, however, the disease is not linked to genes involved in immune tolerance & regulation
#8 Some of these hormones (estrogen, cortisol, and human placental lactogen) can have a blocking effect on insulin
#13 Injected intermediate-acting NPH insulins have been modified to provide prolonged action and are dispensed as a turbid suspension at neutral pH with protamine in phosphate buffer (neutral protamine Hagedorn [NPH] insulin)
#16 Lipohypertrophy is the formation of fatty lumps at or around insulin injection sites
#27 Storage
Vials of insulin not in use should be refrigerated. Extreme temperatures (<36 or >86°F, <2 or >30°C) and excess agitation should be avoided to prevent loss of potency, clumping, frosting, or precipitation
. Insulin in use may be kept at room temperature to limit local irritation at the injection site, which may occur when cold insulin is used.
#40 Antithyroid drugs inhibit the manufacture of thyroid hormones
They do not affect existing thyroid hormones that are circulating in the blood or stored in the thyroid gland
For this reason, therapeutic effects of the antithyroid drugs may not be observed for 3 to 4 wks
Thionamides: propylthiouracil (PTU)