The ventricles Move in a fast and disorganized way instead of contracting normally.
No blood is pumped out of the heart → this causes cardiac arrest.
⚠️ Medical emergency — needs CPR and defibrillation (electric shock) immediately
History
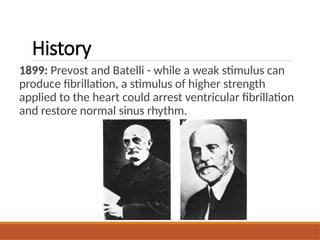
1899: Prevost andBatelli - while a weak stimulus can
produce fibrillation, a stimulus of higher strength
applied to the heart could arrest ventricular fibrillation
and restore normal sinus rhythm.
History
1966: Belfast Ambulancetransported physicians
performed first pre-hospital defibrillation.
1969: First pre-hospital defibrillation by non physicians.
1970’s: Diack, Wellborn and Rullman developed first
automated external defibrillator AED’s.
6.
Chain of Survival
EarlyRecognition and Assessment
• Early Access
• Early CPR
• Early Defibrillation
• Early Advanced Cardiac Life Support
8
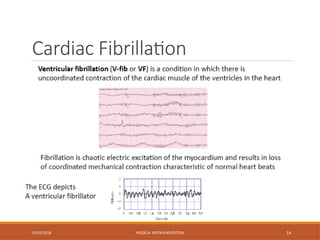
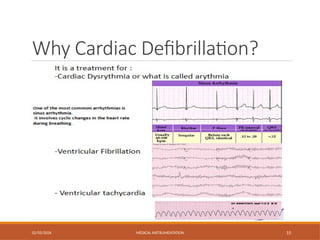
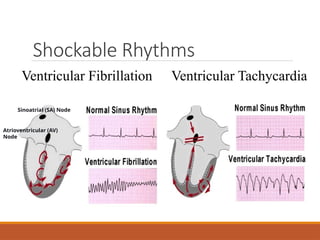
Ventricular Fibrillation (VF)
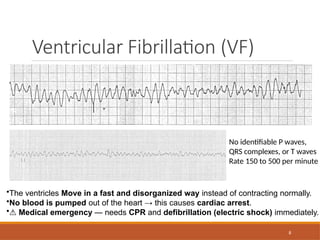
•Theventricles Move in a fast and disorganized way instead of contracting normally.
•No blood is pumped out of the heart → this causes cardiac arrest.
•⚠️Medical emergency — needs CPR and defibrillation (electric shock) immediately.
No identifiable P waves,
QRS complexes, or T waves
Rate 150 to 500 per minute
9.
9
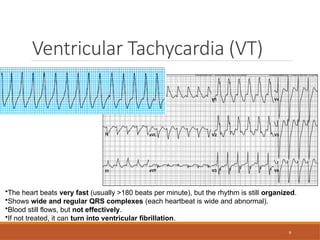
Ventricular Tachycardia (VT)
•Theheart beats very fast (usually >180 beats per minute), but the rhythm is still organized.
•Shows wide and regular QRS complexes (each heartbeat is wide and abnormal).
•Blood still flows, but not effectively.
•If not treated, it can turn into ventricular fibrillation.
10.
10
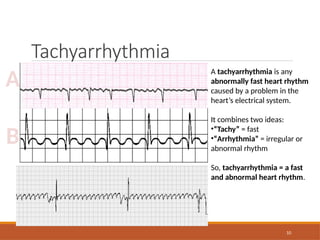
Tachyarrhythmia
A
B
A tachyarrhythmia isany
abnormally fast heart rhythm
caused by a problem in the
heart’s electrical system.
It combines two ideas:
•“Tachy” = fast
•“Arrhythmia” = irregular or
abnormal rhythm
So, tachyarrhythmia = a fast
and abnormal heart rhythm.
11.
11
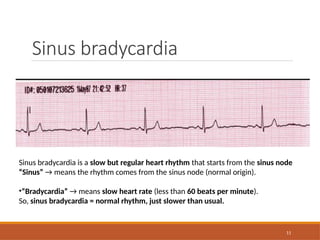
Sinus bradycardia
Sinus bradycardiais a slow but regular heart rhythm that starts from the sinus node
“Sinus” → means the rhythm comes from the sinus node (normal origin).
•“Bradycardia” → means slow heart rate (less than 60 beats per minute).
So, sinus bradycardia = normal rhythm, just slower than usual.
13
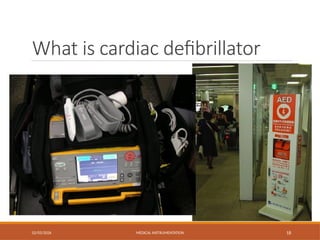
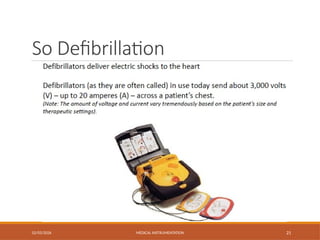
DEFIBRILLATORS
Cardiac fibrillation isa condition where in the
individual myocardial cells contract asynchronously
with only very local patterns relating to the
contraction of one cell and that of the next. This
serious condition reduces the cardiac output to near
zero, and it must be corrected as soon as possible
to avoid damage to the patient and death. Electric
shock to the heart can be used to reestablish a more
normal cardiac rhythm. Electric machines that
produce the energy to carry out this function are
known as defibrillators.
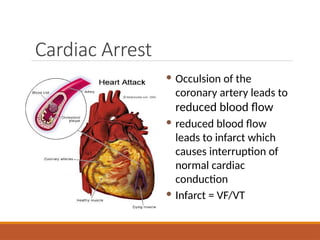
Cardiac Arrest
Occulsionof the
coronary artery leads to
reduced blood flow
reduced blood flow
leads to infarct which
causes interruption of
normal cardiac
conduction
Infarct = VF/VT
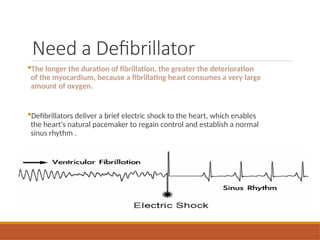
The longer theduration of fibrillation, the greater the deterioration
of the myocardium, because a fibrillating heart consumes a very large
amount of oxygen.
Defibrillators deliver a brief electric shock to the heart, which enables
the heart's natural pacemaker to regain control and establish a normal
sinus rhythm .
Need a Defibrillator
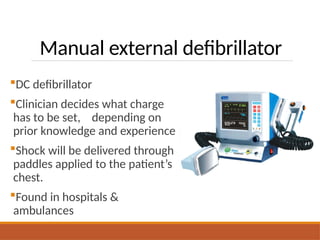
Manual external defibrillator
DCdefibrillator
Clinician decides what charge
has to be set, depending on
prior knowledge and experience
Shock will be delivered through
paddles applied to the patient’s
chest.
Found in hospitals &
ambulances
26.
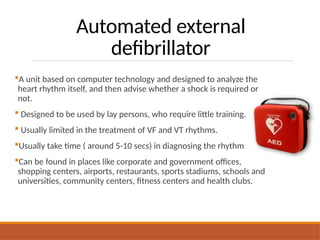
Automated external
defibrillator
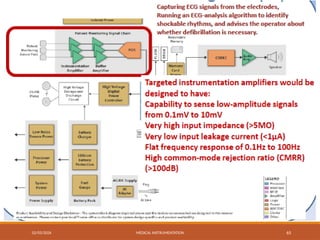
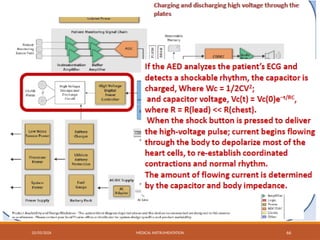
A unitbased on computer technology and designed to analyze the
heart rhythm itself, and then advise whether a shock is required or
not.
Designed to be used by lay persons, who require little training.
Usually limited in the treatment of VF and VT rhythms.
Usually take time ( around 5-10 secs) in diagnosing the rhythm
Can be found in places like corporate and government offices,
shopping centers, airports, restaurants, sports stadiums, schools and
universities, community centers, fitness centers and health clubs.
28.
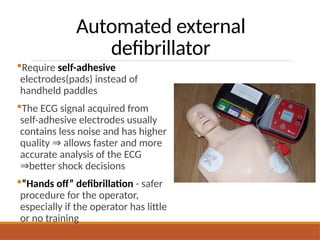
Automated external
defibrillator
Require self-adhesive
electrodes(pads)instead of
handheld paddles
The ECG signal acquired from
self-adhesive electrodes usually
contains less noise and has higher
quality allows faster and more
⇒
accurate analysis of the ECG
better shock decisions
⇒
“Hands off” defibrillation - safer
procedure for the operator,
especially if the operator has little
or no training
29.
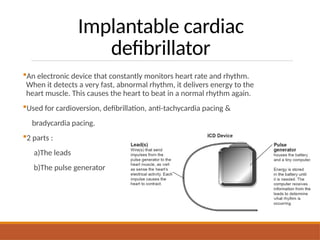
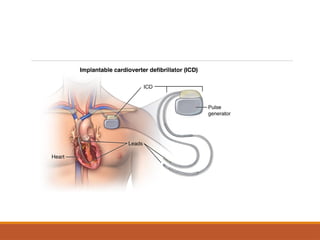
Implantable cardiac
defibrillator
An electronicdevice that constantly monitors heart rate and rhythm.
When it detects a very fast, abnormal rhythm, it delivers energy to the
heart muscle. This causes the heart to beat in a normal rhythm again.
Used for cardioversion, defibrillation, anti-tachycardia pacing &
bradycardia pacing.
2 parts :
a)The leads
b)The pulse generator
How does itwork?
Electronic counter-shock between to paddles or pads
Depolarises all cardiac cells and interrupts arrhythmia
Allows Sinoatrial (SA) node to recommence its
dominant role
Defibrillation is the most time critical intervention in a patient with a
shockable rhythms
33.
How does itwork?
Thoracic Impedance
Impedance is the natural resistance to the flow of
electrical current, measured in Ohms.
Impedance is determined by a number of factors, such
as:
◦ Underlying structures and pathology
◦ Paddle or adhesive pad position
34.
How does itwork?
Monophasic Defibrillation
Delivers ‘shock’ in one phase
Adult: 200J, 300J, 360J, all subsequent shocks at 360J
Child: 2J/Kg, 2J/Kg, 4J/Kg, all subsequent shocks at 4J/Kg
35.
How does itwork?
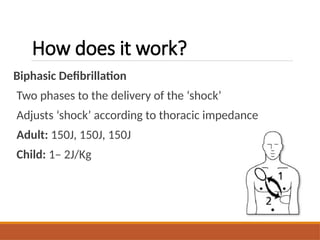
Biphasic Defibrillation
Two phases to the delivery of the ‘shock’
Adjusts ‘shock’ according to thoracic impedance
Adult: 150J, 150J, 150J
Child: 1– 2J/Kg
36.
How does itwork?
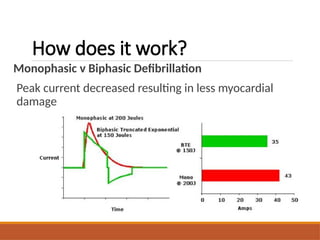
Monophasic v Biphasic Defibrillation
Peak current decreased resulting in less myocardial
damage
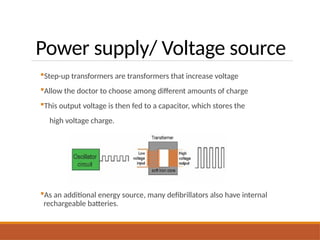
Power supply/ Voltagesource
Step-up transformers are transformers that increase voltage
Allow the doctor to choose among different amounts of charge
This output voltage is then fed to a capacitor, which stores the
high voltage charge.
As an additional energy source, many defibrillators also have internal
rechargeable batteries.
44.
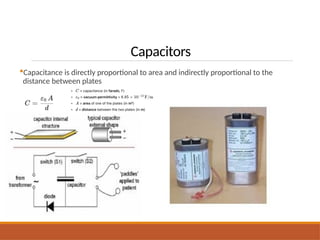
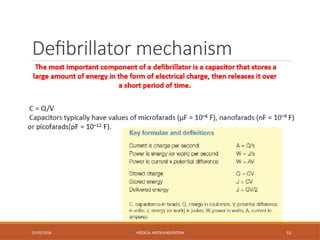
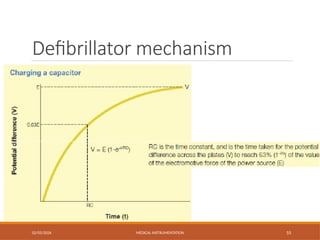
Capacitors
Capacitors store alarge amount of energy in the form of
electric charge
This stored energy is released over a short period of time
“Capacitance” describes a capacitor quantitatively
C = Q/V
A capacitor has 1 farad of capacitance if a potential difference of 1 volt
is present across its plates, when they hold a charge of 1 coulomb.
Capacitors typically have values of microfarads
Inductors
Coils of wirethat produce a magnetic field
when current flows through them, prolong the
duration of current flow
Inductors generate electricity that opposes the
motion of current passing through it
This opposition is called “inductance (L)”.
Inductors typically have values of microhenries
(µH).
47.
02/03/2026 MEDICAL INSTRUMENTATION47
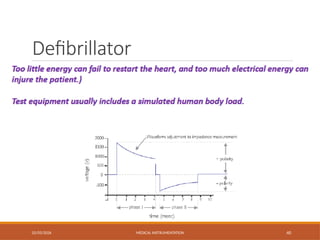
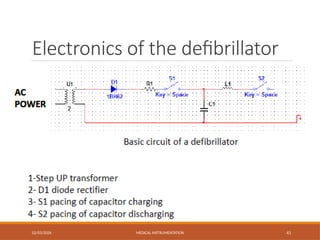
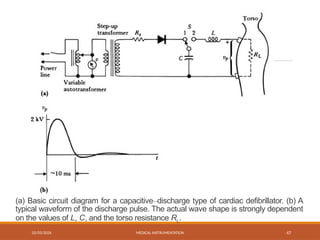
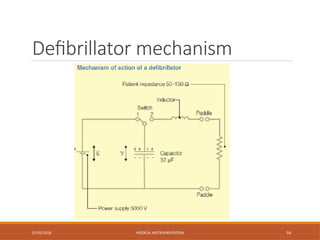
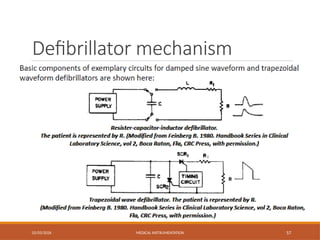
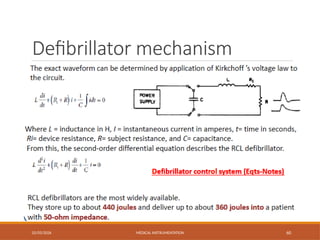
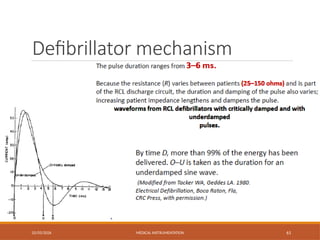
(a) Basic circuit diagram for a capacitive–discharge type of cardiac defibrillator. (b) A
typical waveform of the discharge pulse. The actual wave shape is strongly dependent
on the values of L, C, and the torso resistance RL.
48.
48
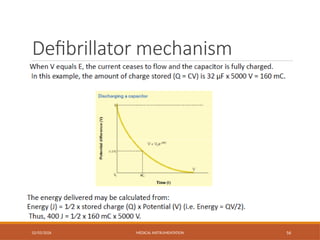
Defibrillators
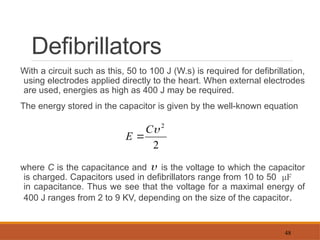
With a circuitsuch as this, 50 to 100 J (W.s) is required for defibrillation,
using electrodes applied directly to the heart. When external electrodes
are used, energies as high as 400 J may be required.
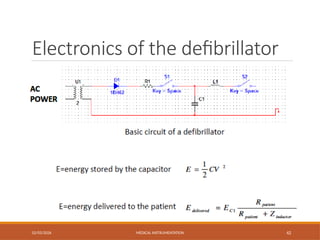
The energy stored in the capacitor is given by the well-known equation
where C is the capacitance and is the voltage to which the capacitor
is charged. Capacitors used in defibrillators range from 10 to 50 μF
in capacitance. Thus we see that the voltage for a maximal energy of
400 J ranges from 2 to 9 KV, depending on the size of the capacitor.
2
2
C
E
49.
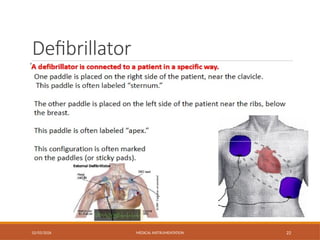
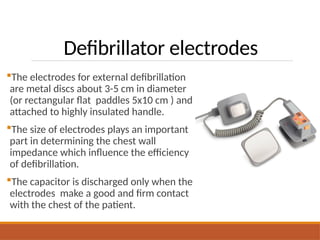
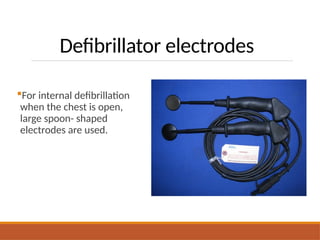
Defibrillator electrodes
The electrodesfor external defibrillation
are metal discs about 3-5 cm in diameter
(or rectangular flat paddles 5x10 cm ) and
attached to highly insulated handle.
The size of electrodes plays an important
part in determining the chest wall
impedance which influence the efficiency
of defibrillation.
The capacitor is discharged only when the
electrodes make a good and firm contact
with the chest of the patient.
02/03/2026 MEDICAL INSTRUMENTATION52
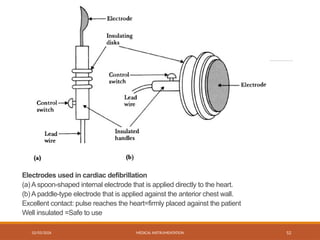
Electrodes used in cardiac defibrillation
(a) A spoon-shaped internal electrode that is applied directly to the heart.
(b) A paddle-type electrode that is applied against the anterior chest wall.
Excellent contact: pulse reaches the heart=firmly placed against the patient
Well insulated =Safe to use
CARDIOVERTER
02/03/2026 MEDICAL INSTRUMENTATION70
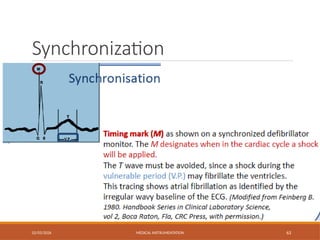
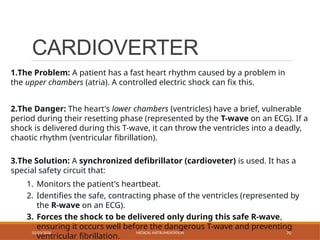
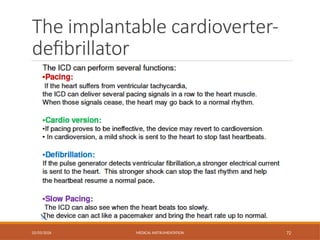
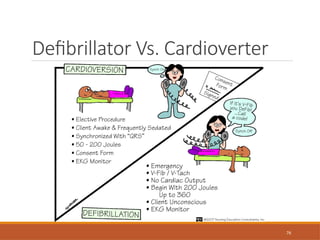
1.The Problem: A patient has a fast heart rhythm caused by a problem in
the upper chambers (atria). A controlled electric shock can fix this.
2.The Danger: The heart's lower chambers (ventricles) have a brief, vulnerable
period during their resetting phase (represented by the T-wave on an ECG). If a
shock is delivered during this T-wave, it can throw the ventricles into a deadly,
chaotic rhythm (ventricular fibrillation).
3.The Solution: A synchronized defibrillator (cardioveter) is used. It has a
special safety circuit that:
1. Monitors the patient's heartbeat.
2. Identifies the safe, contracting phase of the ventricles (represented by
the R-wave on an ECG).
3. Forces the shock to be delivered only during this safe R-wave,
ensuring it occurs well before the dangerous T-wave and preventing
ventricular fibrillation.
02/03/2026 MEDICAL INSTRUMENTATION73
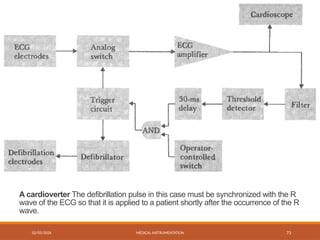
A cardioverter The defibrillation pulse in this case must be synchronized with the R
wave of the ECG so that it is applied to a patient shortly after the occurrence of the R
wave.
73.
74
Cardioverters
The signal fromthe electrodes passes through a
switch that is normally closed. The operator can
observe the patient’s ECG to see whether the
cardio version was successful. The output is
also filtered and passed through a threshold
detector that detects the R wave. This activates
a delay circuit that delays the signal by 30 ms
and then activates a trigger circuit that opens the
switch connecting the ECG electrodes to the
amplifier. At the same time, it closes a switch
that discharges the defibrillator capacitor.
Defibrillator maintenance
policy
First, Thedaily test procedure - 30 J self test
‑ : is a low energy
test to check the charging circuits & the integrity of cables.
Second, a weekly check - is carried out to test at higher energy
level using ECG simulator.
Third, the detailed half yearly test procedure-
‑ should be
performed by the biomedical department in a hospital
77.
Daily low energytest
Step 1 : Put the defibrillator on Battery mode and ensure
machine
is disconnected from the AC power supply .
Turn the selector switch to ON and select Manual mode
Select leads to PADDLES/PADS
Step 2 : Ensure the universal cable is connected to the paddles
Place paddles in paddle wells
Step 3 : Select the ENERGY to 30 J
Step 4 : Press the CHARGE button
Step 5 : The unit charges to 30J, then the red LED charge
indicator illuminates and the charge tone sounds
78.
Step 6 :Ensure DEFIB 30J READY displays on screen
Step 7 : Press and hold both paddles SHOCK buttons
Step 8 : The unit discharges. The TEST OK message displays and
the red LED turns off
Step 9 : The above TEST OK message conforms that low energy
circuits are in proper working condition
79.
Weekly test: Defibrillator
internaldischarge test
Repeat the steps from 1 to 9
Step 10 : Select ENERGY button to maximum energy level 200J displays
Step 11 : The unit charges to 200J, then the red LED charge indicator
illuminates and the charge tone sounds
Step 12 : Ensure DEFIB 200J READY displays on screen
Step 13 : Ensure the machine holds the charge for 50 seconds by giving a long
continuous sound
Step 14 : This confirms the unit is fully functional
80.
1) Duration ofVF
- the longer VF lasts, the harder it is to cure
- the quicker the better
- shock early, shock often
- likelihood of resuscitation decrease by 7-10% with every
passing minute (Ann Emerg Med. 1993;22:1652–1658 )
Factors to consider during defibrillation
81.
2) Myocardial environment/ condition
Hypoxia, acidosis, hypothermia, electrolyte imbalance,
drug toxicity – impede conversion.
DO NOT DELAY SHOCK trying to correct these problems.
Factors to consider during defibrillation
82.
3) Heart size/ Body type
Pediatric requirement lower than adult
2J /kg initial shock
4J /kg repeat shock
Higher dose (up to 10J/kg)
Or adult maximum dose
Direct size / energy relationship in adults unknown
Factors to consider during defibrillation
83.
4) Use largestsize paddles
- completely contact chest without paddles touching each
other
- In pediatric minimum of 3cm distance between pads.
NOTE :-
- Small paddles : concentrate current, burn heart.
- Large paddles : reduces current density
Factors to consider during defibrillation
84.
5) Previous countershock
- repeated shocks lower resistance
- give one shock at a time & then continue CPR
- subesquent shock either equal or higher energy
6) Paddle size
( as discussed before)
Factors to consider during defibrillation
85.
7) Paddle placement
-In pacemaker / ICD
at least 12cm from generator
90 degree toAICD electrode
avoid placing pads directly over
no delay in defibrillation
- for other as described before…….
Factors to consider during defibrillation
86.
8) Paddles –Skin interface
- only gel should be used (ECG gelly)
- cream, paste, saline pads etc.- not recommended
- gel decreases resistance to the flow of current
- never use alcohol
9) Paddle contact pressure
- firm pressure of 25 pounds
- in child <10kgs --- 3kg pressure
- in large children >10kgs --- 5kg pressure
- deflate lung, shortens the path of current
- do not lean on paddles : they slip
Factors to consider during defibrillation
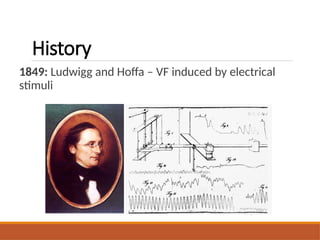
#2 1849: Written history of fibrillation and defibrillation goes back to the pioneering work of Carl Ludwig’s laboratory. In 1849, Ludwig’s student M. Hoffa was the first to witness and, most importantly, to document the onset of ventricular fibrillation, which he induced by electrical stimulus. This picture from their paper shows rapid contractions produced by electrical stimulation, which resulted in cardiac arrest.
#3 1899: Further experiments with “faradization” of the heart were conducted by two physiologists from University of Geneva, Switzerland, J.-L. Prevost and F. Batelli. They discovered that, while a weak stimulus can produce fibrillation, a stimulus of higher strength applied to the heart could arrest ventricular fibrillation and restore normal sinus rhythm. This discovery was made in 1899. Unfortunately, unlike discovery of contemporary electrocardiogram, defibrillation did not enjoy similar attention and success. They did this using dogs!
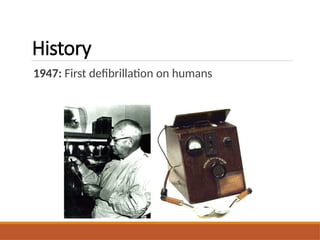
#4 Work of Carl J. Wiggers in the Department of Physiology of Western Reserve University was well known to the thoracic surgeon Claude S. Beck from the University Hospitals in Cleveland, which are adjacent to the Western Reserve University. In 1947, Dr. Beck successfully applied defibrillation therapy and saved the first human life by this method (C.S. Beck, W.H. Pritchard, H.S. Feil, Ventricular fibrillation of long duration abolished by electric shock. Jour. Amer. Med. Assoc. 135: 985, 1947). His success triggered the immediate acceptance of this method by the clinical community and started a wide front of basic and clinical research of fibrillation and defibrillation.
#5 Work of Carl J. Wiggers in the Department of Physiology of Western Reserve University was well known to the thoracic surgeon Claude S. Beck from the University Hospitals in Cleveland, which are adjacent to the Western Reserve University. In 1947, Dr. Beck successfully applied defibrillation therapy and saved the first human life by this method (C.S. Beck, W.H. Pritchard, H.S. Feil, Ventricular fibrillation of long duration abolished by electric shock. Jour. Amer. Med. Assoc. 135: 985, 1947). His success triggered the immediate acceptance of this method by the clinical community and started a wide front of basic and clinical research of fibrillation and defibrillation.
#8 VF:
Chaotic irregular deflections of varying amplitude
No identifiable P waves, QRS complexes, or T waves
Rate 150 to 500 per minute
#9 VT:
Shows wide and regular QRS complexes (each heartbeat is wide and abnormal).
The rhythm is fast but organized — you can still see a repeating pattern.
Rate: usually between 150–250 beats per minute.
Wide QRS complex
Tachycardia
Atrioventricular AV dissociation
#44 C = capacitance of the capacitor (in farads, F)
Q = charge stored on one plate (in coulombs, C)
V = potential difference or voltage across the plates (in volts, V)
#73 The diagram shows how an AED works: It listens to the heart (ECG Electrodes), cleans up the signal (Amplifier, Filter), analyzes it (Threshold Detector) to see if a shock is needed, and then waits for human confirmation (Operator Switch) before delivering the shock (Trigger, Defibrillator, Electrodes). The AND Gate is the crucial safety feature ensuring a shock can never be given automatically without the rescuer's consent.
#82 1. Hypoxia
A condition where tissues receive insufficient oxygen to maintain normal cellular functions.
➡️ Causes: respiratory failure, anemia, circulatory issues.
➡️ Effect: reduces energy (ATP) production in cells.
2. Acidosis
An abnormal increase in acidity (low pH) of blood or body tissues.
➡️ Causes: buildup of CO₂ (respiratory acidosis) or metabolic acids (metabolic acidosis).
➡️ Effect: interferes with enzyme activity and cellular metabolism.
3. Hypothermia
A state in which body temperature drops below normal (< 35°C).
➡️ Causes: exposure to cold, anesthesia, shock.
➡️ Effect: slows metabolic reactions and enzyme function.
4. Electrolyte Imbalance
An abnormal level of ions (like Na⁺, K⁺, Ca²⁺, Cl⁻) in the body.
➡️ Causes: dehydration, kidney problems, medications.
➡️ Effect: disrupts nerve conduction, muscle contraction, and enzyme activity.
5. Drug Toxicity
A harmful effect of excessive or inappropriate drug concentration in the body.
➡️ Causes: overdose, impaired metabolism, drug interactions.
➡️ Effect: damages organs and interferes with normal biochemical processes.