



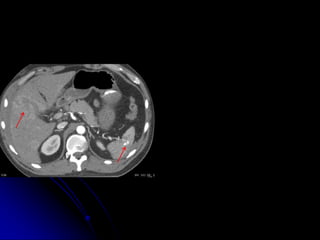
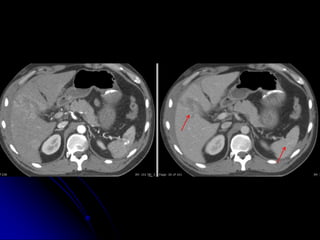




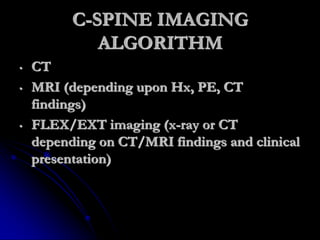


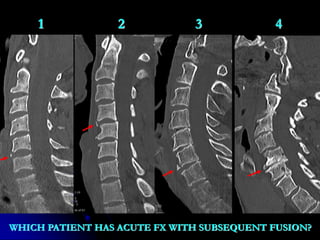






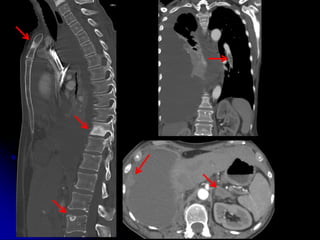







This document discusses challenges in diagnostic imaging for elderly patients aged 60 and up. It outlines various imaging modalities like X-ray, CT, MRI, and ultrasound that are useful for diagnosing acute injuries in older patients. It notes that comorbidities and incidental findings can complicate the imaging evaluation process. The value of communication among healthcare providers is emphasized. Protocols for head/spine and whole body CT imaging are provided, along with an algorithm for cervical spine imaging. Examples demonstrate challenges in identifying acute fractures versus incidental findings or prior fusion. Communication among the diagnostic imaging team is highlighted as key.
























































