Causes ofcell injury
General mechanisms of cell injury
Pathogenesis of cell injury
Free radical induced cell injury
Examples of reversible cell injury
Learning objectives
3.
COMPETENCY PA 2.1,2.2-Describe the causes,mechanisms,types, effects of cell injur
& their clinical significance
OBJECTIVES:
At the end of the lecture the student should be
able to
Define cell injury
Enumerate the Causes /etiology of cell injury
Describe the salient mechanisms
/pathogenesis of cell injury
Classify the cellular responses to cell injury &
their clinical significance
4.
Pathology isthe study of the structural,
biochemical, and functional changes in cells,
tissues, and organs that underlie disease.
The four aspects of a disease process that form
the core of pathology are its cause (etiology),
The biochemical and molecular mechanisms of its
development (pathogenesis),
The structural alterations induced in the cells and
organs of the body (morphologic
changes), and
The functional consequences of these changes
(clinical manifestations).
5.
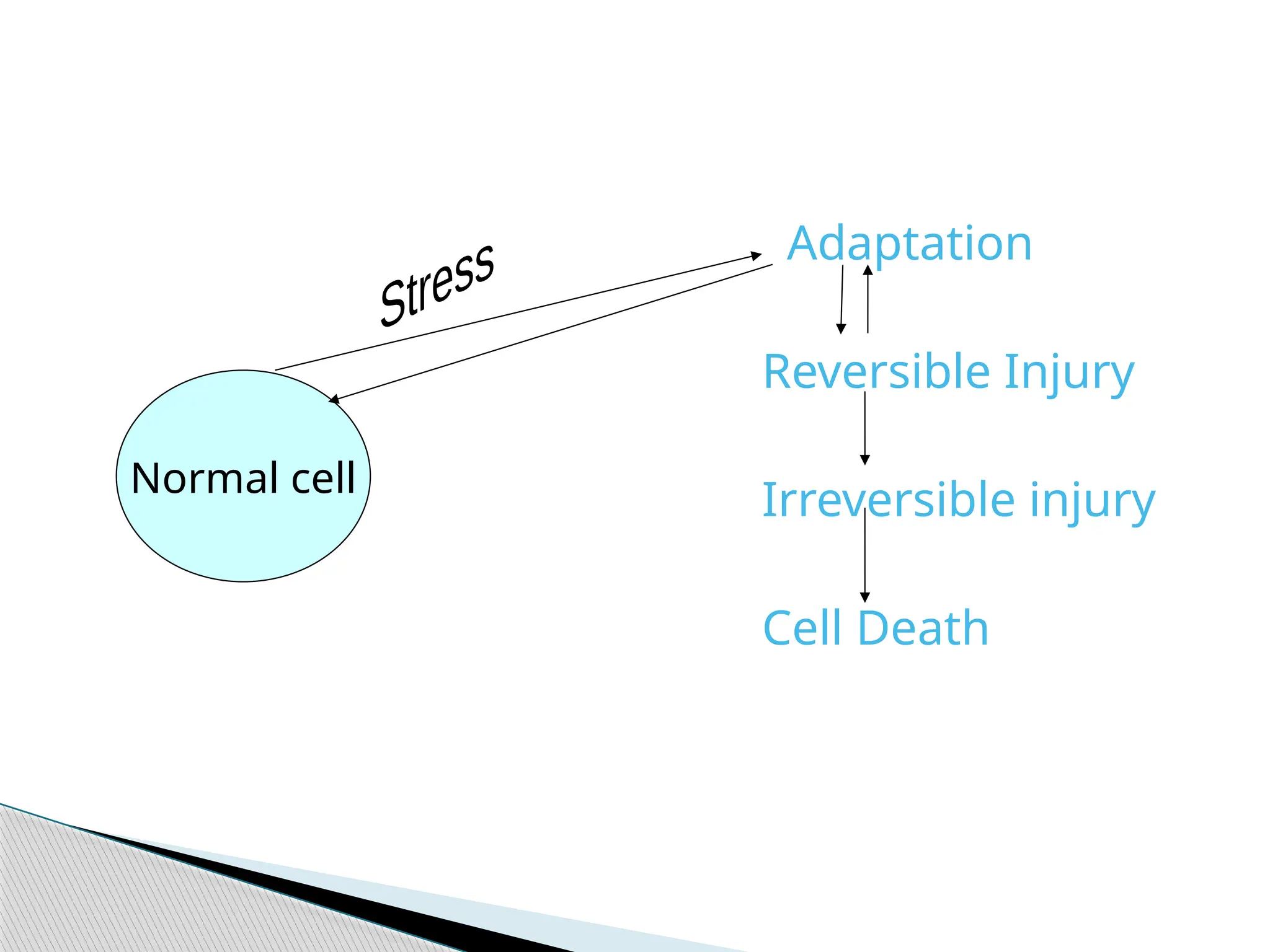
Normal cellshave a fairly narrow range of
function or steady state. HOMEOSTASIS.
Excess physiologic or pathologic stress may
force the cell to a new steady state.
ADAPTATION.
Too much stress exceeds the cells adaptive
capacity. INJURY.
Cell injury can be reversible or irreversible.
Reversiblity depends on the type, severity and
duration of injury.
Cell death is the result of irreversible injury.
Key concepts
6.
STATUS, ADAPTABILITY OFTARGET CELL:
Skeletal muscle can withstand hypoxic injury
for long-time,
Cardiac muscle suffers Irreversible cell injury
Hypoxia
Reduced bloodflow(ischemia)
Inadequate oxygenation of the blood due to
cardiorespiratory failure.
Decreased oxygen carrying capacity of the
blood as in anaemia and CO poisoning.
Severe blood loss.
Causes of Cell Injury:
10.
Physical—agents: Mechanicaltrauma,
radiation, extremes of temperature.
Chemical—agents: Cyanide, arsenic,
mercury.
Infectious—agents: Bacteria, fungi,
parasites.
Immunological—reactions:Auto-immune ds.
Genetic-Rearrangements: Chromosomal
anomalies, inborn errors of metabolism.
Nutritional—imbalance: PEM, Vit. Def.
Causes of Cell Injury:
11.
Cell membraneintegrity Injury at 1
Aerobic respiration locus leads to wide
Protein synthesis ranging
secondary
Genetic apparatus effects
Depending on : Type
Duration of Injury
Severity
Sites of Damage
12.
5 Mechanisms
ATPdepletion
Mitochondrial Damage
Loss of calcium homeostasis
Defects in membrane
permeability
Free radical injury
Mechanisms of cell injury
Reduced oxidativephosphorylation & ATP
depletion,
Cellular swelling & blebbing of plasma
membrane: due to changes in ion concentrations
and water influx,
Swelling of ER & Mitochondria,
Clumping of chromatin.
Reversible Cell Injury:
Mitochondrial Damage
Formation ofa high conductance channel
in the mitochondrial membrane, called the
membrane permeability transition pore
Loss of mitochondrial membrane
Failure of normal oxidative phosphorylation
Depletion of ATP
The mitochondria sequesterCytochrome c bet
their outer and inner membranes
Mitochondrial Damage
Increased permeability of the outer
mitochondrial membrane
Leakage of cytochrome C into the cytosol
APOPTOSIS
19.
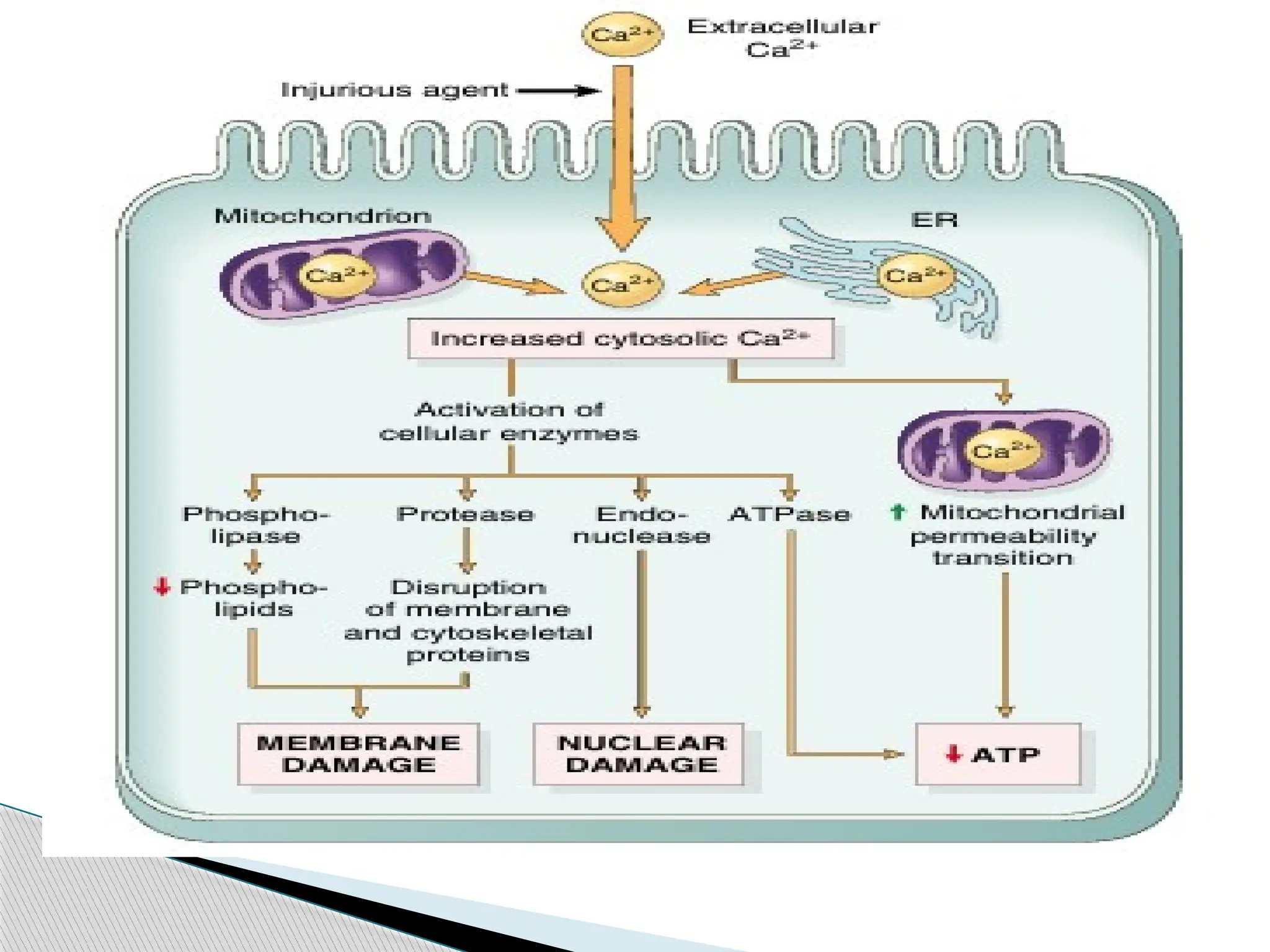
Intracellular freecalcium is very low compared
with extracellular levels.
Most intracellular calcium is sequestered in
mitochondria and ER.
Injury cause an increase in cytosolic calcium
due to
1.Increased influx across the plasma membrane.
2.Release of calcium from intracellular stores
(mitochondria and ER)
Calcium Homeostasis
20.
Increased cytosoliccalcium activates number
of enzymes
1.Phospholipases(Membrane Damage)
2.Proteases(breakdown both membrane and
cytoskeletal proteins)
3.Endonucleases(DNA fragmentation)
4. ATPases(hastening ATP depletion)
Opening ofthe mitochondrial permeability
transition pore
1.Failure of ATP generation
2.Formation of ROS
3.Release of cytochrome C -APOPTOSIS
Mitochondrial injury
24.
Loss of osmoticbalance
Efflux of fluids and ions
Loss of cellular contents
Leak metabolites that are vital for the
reconsititution of ATP
Plasma membrane damage
25.
Lysosomes containRNases, DNases, proteases,
phosphatases,glucosidases and cathepsins
Lysosomal membrane damage
Leakage of their enzymes into the cytoplasm
Enzymatic digestion of proteins,RNA,DNA,and
glycogen
Necrosis
Lysosomal membrane Damage
28.
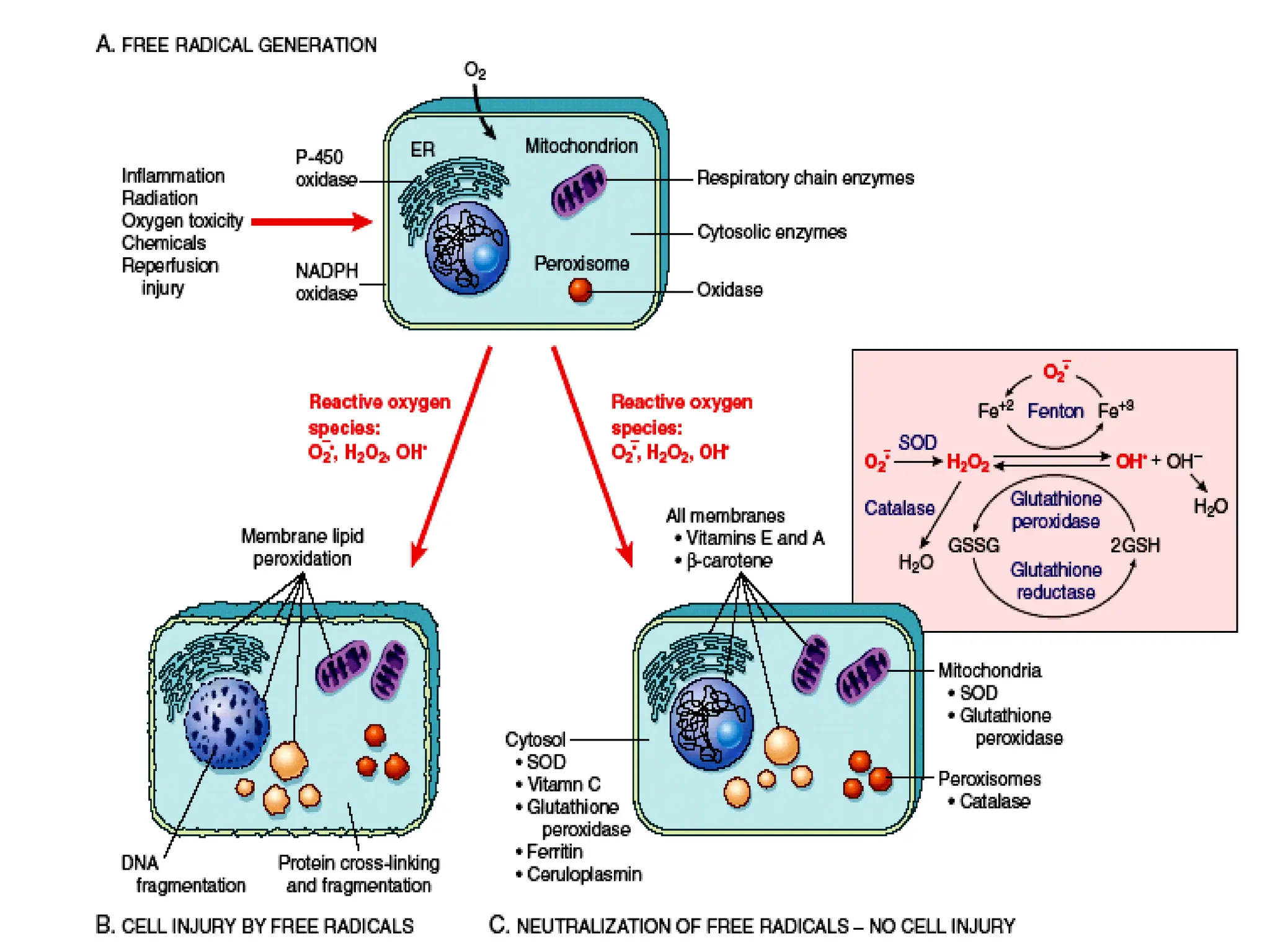
Free radicalshave single unpaired electron in
its outer orbit.
Unpaired electrons are highly reactive and
attack and modify -proteins, lipids,
carbohydrates, nucleic acids.
Generated within mitochondrial inner
membrane.
Free radicals Generation
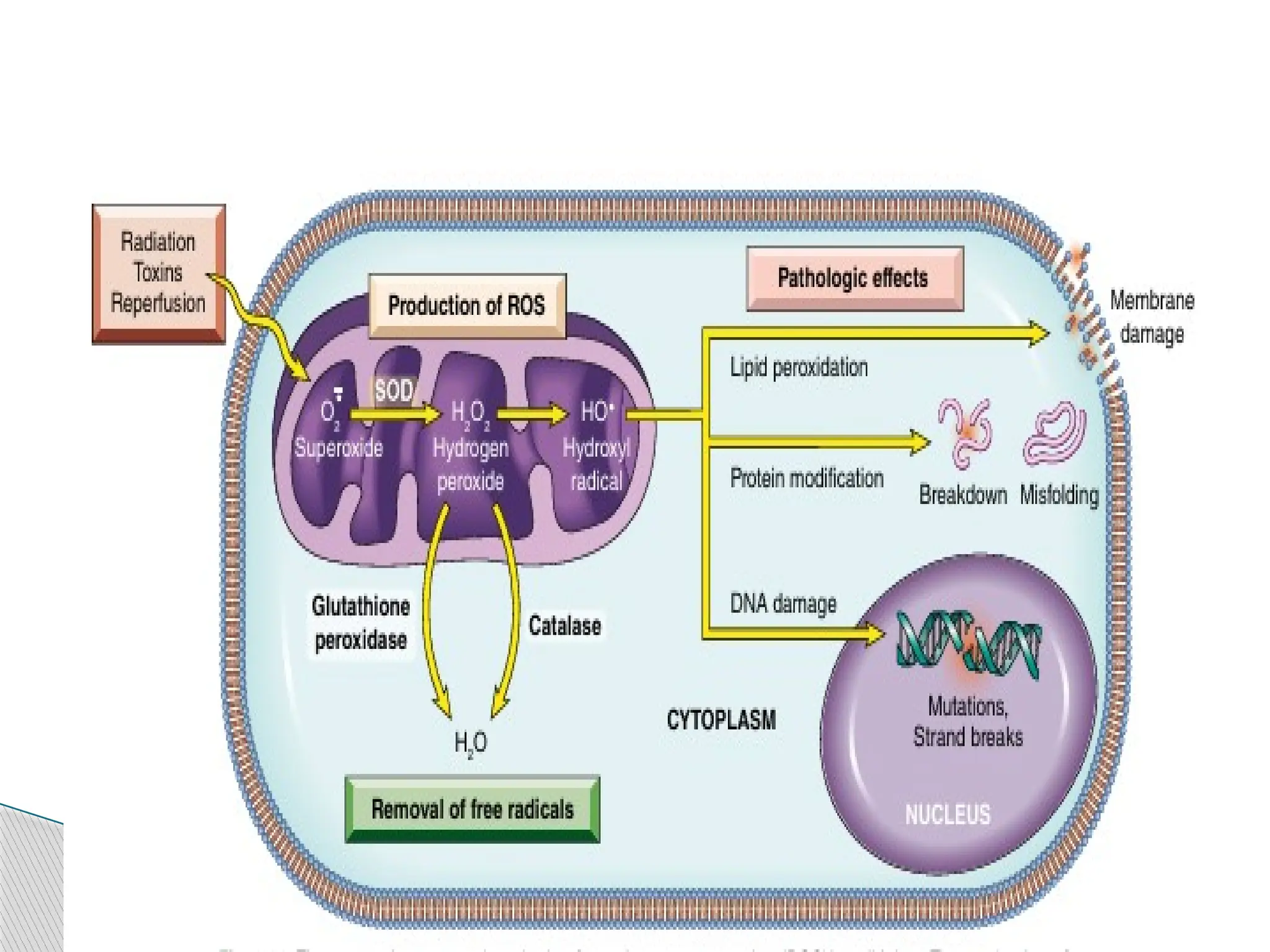
29.
◦ Partially reduced,unavoidable byproducts of
mitochondrial respiration.
◦ E.g., OH-, O2-,H2O2,
Have single unpaired electron in outer orbit;
highly unstable configuration.
Capable of damaging lipids, proteins & nucleic
acids.
Oxygen Free Radicals:
30.
Imbalance betweenfree O2 radical generating
system & radical scavenging system results in
OXIDATIVE STRESS.
During initiate autocatalytic reactions:
molecules with which they react are themselves
convert into free radicals propagating the chain
of reaction.
Oxygen Free Radicals:
31.
Absorption ofradiant energy: ionizing radiation,
UV rays, X-rays.
Enzymatic metabolism of exogenous chemicals
or drugs
The reduction-oxidation Rn that occur during
normal metabolic process.
Production of free radicals:
32.
Transition metals:Copper & Iron ; donate or
accept free electrons and catalyze free radical
formation: Fenton Reaction.
Nitric oxide: an imp. Chemical mediator, that
can act as free radical.
Free radicals include
Superoxide anion
Hydrogen peroxide
Hydroxyl radicals
The most reactive free radical is hydroxyl free
radical.
Production of free radicals:
35.
Lipid peroxidationof membranes
Oxidative modification of proteins
Single stranded breaks in DNA
Effects of Free Radicals:
36.
Membrane lipidsare attacked(plasma and
organelle membrane)
Free radicals and lipids combination releases
formation of unstable peroxides
In turn activates autocatalytic reaction
Leads to extensive tissue damage.
Lipid peroxidation
37.
Most ofthe enzymes are made up of
aminoacids and proteins.
Free radicals cause oxidation of these
aminoacids.
Results in damage to active site of enzymes.
Structural proteins are damaged.
Extensive destruction of protein machinery
DNA DAMAGE
Free radicals breaks the DNA and results in
cross linking.
Protein oxidation
38.
Enzymatic:: Superoxide Dismutase
Glutathione peroxidase
Catalase
Non Enzymatic:: Vit-E, Vit- A, Vit-C,
Ferritin,
Ceruloplasmin.
Anti-Oxidants
39.
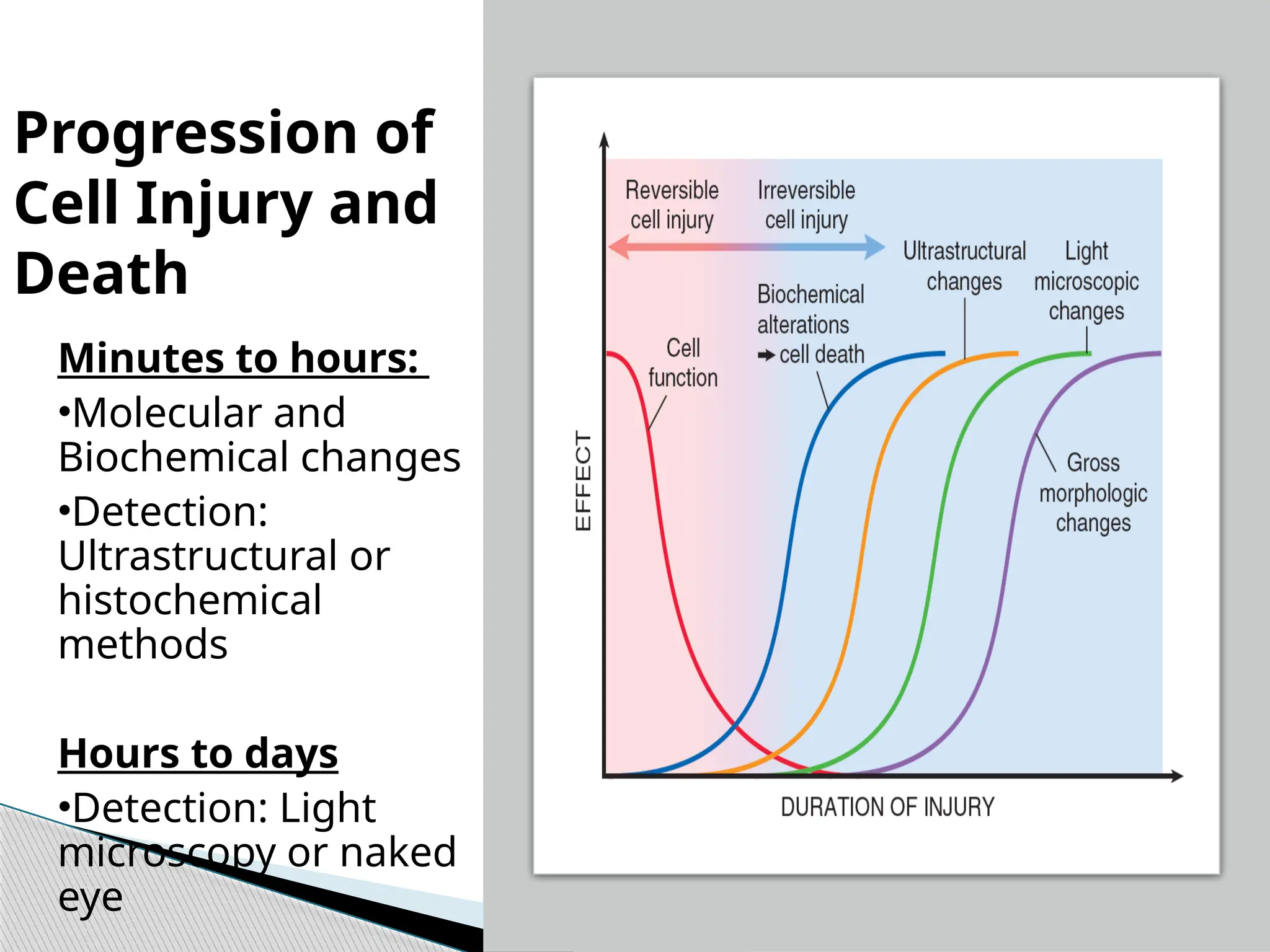
Progression of
Cell Injuryand
Death
Minutes to hours:
•Molecular and
Biochemical changes
•Detection:
Ultrastructural or
histochemical
methods
Hours to days
•Detection: Light
microscopy or naked
eye
40.
Reversible Cell Injury:
Reduced oxidative phosphorylation & ATP
depletion,
Cellular swelling & blebbing of plasma
membrane: due to changes in ion concentrations
and water influx,
Swelling of ER & Mitochondria,
Clumping of chromatin.
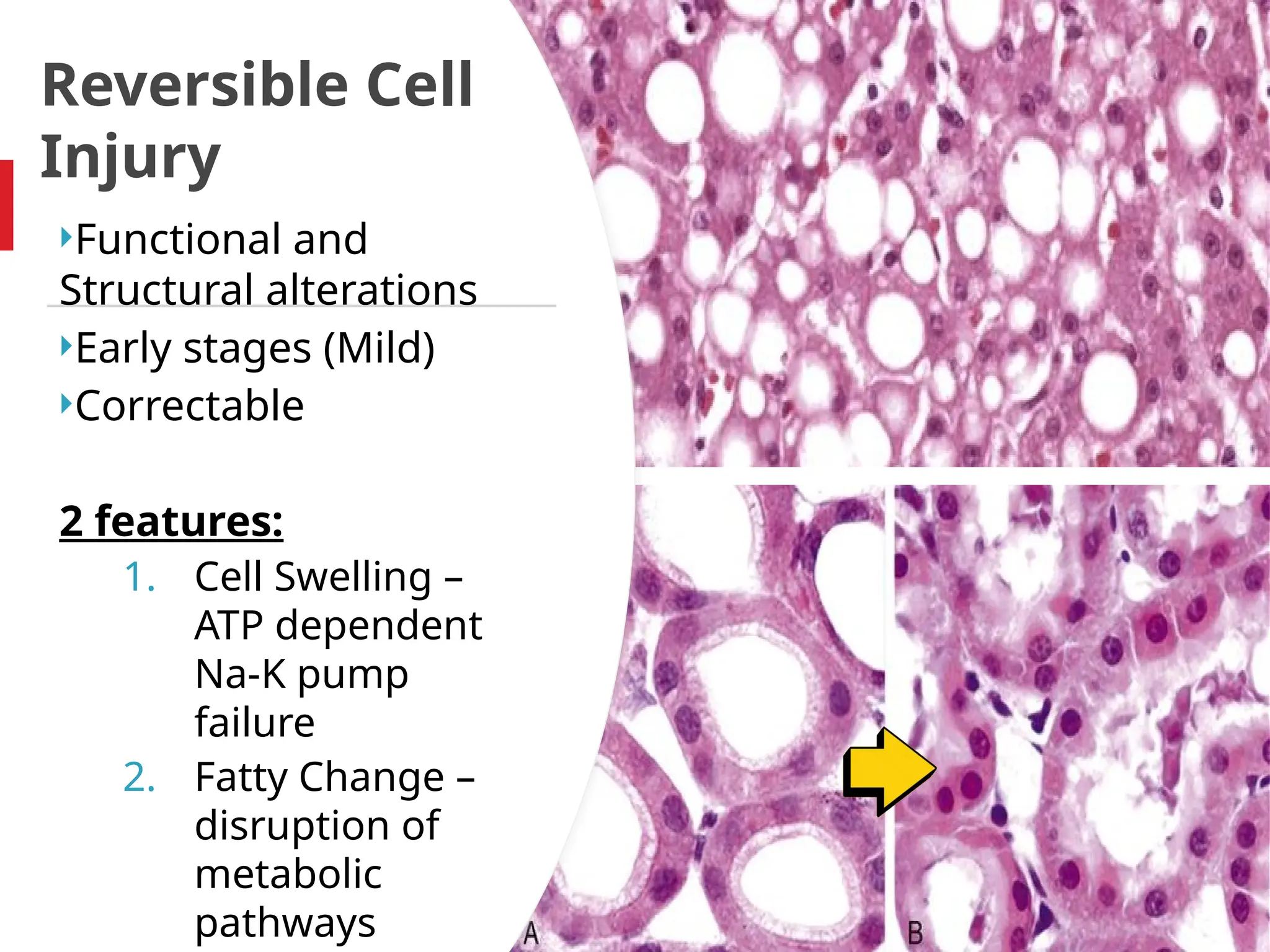
41.
Reversible Cell
Injury
Functional and
Structuralalterations
Early stages (Mild)
Correctable
2 features:
1. Cell Swelling –
ATP dependent
Na-K pump
failure
2. Fatty Change –
disruption of
metabolic
pathways
42.
Reversible Injury (Ultrastructurally)
• Blebbing , blunting,
loss of microvilli
• Mitochondrial
swelling and
amorphous
densities
• Myelin figures
• ER dilatation
• Nucleus:
Disaggregation of
granular and
fibrillar elements
43.
Irreversible Cell Injury:
Point of No return: Lethal Hit– structural
changes like amorphous densities in mitochondria,
loss of membrane permeability.
Swelling of mitochondria, lysosome
rupture,nuclear condensation, Myelin figure
formation.
Final result- cell adaptation /death
Cell death : 2 types
1. Necrosis
2. Apoptosis
44.
Normal cell andthe
Changes in Reversible
And Irreversible
Cell injury
45.
Most commontype of cell injury
Diminished blood flow to the tissue
Aerobic glycolysis Anaerobic glycolysis
Cessation of glycolysis.
1st
Reduced oxidative phosphorylation in
Mitochondria
2nd
Depletion of ATP
3rd
Reduced activity of Na pump
ISCHEMIC & HYPOXIC INJURY
46.
4th
Increasedglycolysis—decreased Ph
5th
Detachment of ribosomes, reduced
protein synthesis, lipid deposition
6th
Cellular swelling, Increased K efflux
ISCHEMIC & HYPOXIC INJURY
48.
Reversible injury–flow restored– may recover
Golden Period of ischemia
Can save many lives
Concept of emergency angiography in cath lab
Rarely the restoration may adversely damage
the tissue This is Reperfusion Injury
ISCHEMIA & REPURFUSION
INJURY
49.
Restored bloodbrings in high concentration of
calcium,calcium overload drives mitochondrial
permeability transition pore opening and
subsequent ATP depletion.
Ischemic injury recruits circulating inflammatory
cells,causes additional tissue injury.
By restoring blood flow, reperfusion may actually
increase local inflammatory cell infiltration.
Damaged mitochondria Increased ROS
ISCHEMIA & REPURFUSION
INJURY