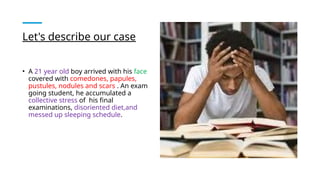
The document discusses a case of a 21-year-old male with severe acne characterized by various lesions, likely due to genetic predispositions and stress-related factors. Despite initial treatments, he required a multi-faceted approach including isotretinoin, antibiotics, and corticosteroids to successfully manage his condition. The document also outlines different types of acne and their underlying causes.











![Acne vulgaris [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/acnevulgarisautosaved-180724092219-thumbnail.jpg?width=640&height=640&fit=bounds)



![ACNE_VULGARIS_2021[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/acnevulgaris20211-220915175500-2b69e7c7-thumbnail.jpg?width=640&height=640&fit=bounds)





































