Case Presentation
Femalepatient, 77 year old , past history of Hypertension, Diabetes Mellitus, Ischemic Heart Disease. The
patient was presented to Emergency Department (ED) complaining of sudden onset and stationary course of
right sided weakness, impaired speech articulation ,comprehension and repetition 2 hours and 30 minutes
before presentation to ED.
On Examination:
The patient was sleepy , GCS 10/15 , Temperature:37.1 C, Blood Pressure 150/95 mmHg, Respiratory Rate
19 breaths/minute, Heart Rate 98 beat/minute, Random Blood Sugar 230 mg/dl, Oxygen saturation 96% on
room air.
Code Stroke in the hospital was activated in 4 minutes of the patient arrival to ED.
General examination of body systems other than Central Nervous System (CNS) was unremarkable.
Neurological examination:
Global aphasia, right upper motor neuron facial paralysis , conjugate deviation of both eyes to the left side
(Right Gaze Palsy).
Right hemiparesis ( upper limb more than lower limb , distal more than proximal ) power grade in upper
limb was 1 and lower limb was 3.
Right sided hypotonia upper limb more than lower limb , distal more than proximal.
Right sided hypo-reflexia upper limb more than lower limb, distal more than proximal.
2.
Case Presentation
Rightextensor plantar response
Neurological examination to the left side was unremarkable
Sensory examination and tests of coordination could not be assessed at the time due to impaired conscious level.
National Institutes of Health Stroke Scale (NIHSS) was 18
Two wide bore intravenous (IV) access were placed , nasal oxygen 3 liter/minute was placed after drop of oxygen
saturation below 94%.
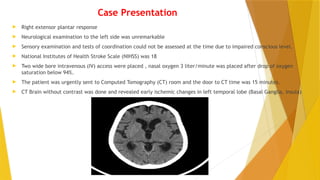
The patient was urgently sent to Computed Tomography (CT) room and the door to CT time was 15 minutes.
CT Brain without contrast was done and revealed early ischemic changes in left temporal lobe (Basal Ganglia, Insula)
3.
Case Presentation
AlbertaStroke Program Early CT Score (ASPECTS) score was 7 and door to CT interpretation was 25 minutes.
Laboratory investigation: INR 1.1 other routine labs were unremarkable
The patient was revised regarding inclusion and exclusion criteria to receive IV recombinant tissue plasminogen
activator (rtPA) and she met it , discussion was done was the patient first degree relatives about benefit/risks of
receiving IV rtPA and written consent was obtained and rtPA (Brand Name: Actilyse) was rapidly prepared after
calculation of total dose at 0.9 mg/kg and bolus (10% of total dose ) was iv given and the rest was given IV over 60
minutes and the door to needle time was 38 minutes and the onset to treatment time was 3 hours and 8 minutes.
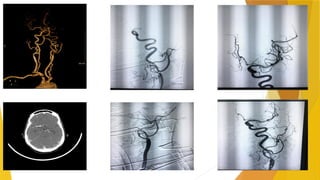
The patient had Computed Tomography Angiography (CTA) while she is on IV rtPA infusion and showed left carotid
bulb calcified atheromatous plaques with luminal stenosis 55% and distal extension of mural thrombus in internal
carotid artery (ICA) with distal progressive narrowing up to total occlusion of distal bifurcation and middle cerebral
artery (MCA).
The patient was candidate to Mechanical Thrombectomy and door to groin puncture was 70 minutes and IV rtPA was
still infused till time of groin puncture and then was holded.
The MCA clot was removed using stent retriever device (Solitaire Platinum 6x40 mm, Medtronic).
Successful recanalization of both left ICA and MCA was achieved as shown in the following images.
5.
Case presentation
Aftersuccessful recanalization the patient was re-evaluated and become fully conscious , mild dysarthria, mild right upper motor
neuron facial paralysis , the right hemiparesis improved from severe weakness to mild weakness in right upper limb power grade 4 and
right lower limb power grade 5.
NIHSS was 4
The patient was then transferred to stroke Intensive Care Unit (ICU) to complete the plan of management with tight control of vital
signs and careful monitoring of both general and neurological condition.
The patient completed her stroke work up which was unremarkable except hyperlipidemia Low Density Lipoprotein (LDL) was 221
mg/dl, also early physiotherapy was started and CT brain without contrast follow up after 24 hours was done and revealed acute left
basal ganglia and insular ischemic infarction with no hemorrhagic transformation, consequently anti-ischemic preventive measures
were started and statins.
After improvement of the patient condition she was discharged to stroke ward and then to home after 5 days of hospital admission and
his Modified Rankin Scale (mRS) that monitor post-stroke disability was1.
The patient was appointed to follow up in stroke preventive clinic and rehabilitation program.
6.
Discussion
In thetreatment of acute ischemic stroke, time is brain. It is crucial to act as soon as possible in order to reduce the
damage to the brain following a lack of blood supply. The impact of bridging therapy on final revascularization outcome,
and on the overall procedural outcome, is still a matter of debate. However, despite an increased risk of intracranial
hemorrhage, in the absence of contraindications to rtPA, the standard therapy for large vessel occlusion above six NIHSS is
a combination of mechanical thrombectomy and rtPA (the so-called “bridging therapy”) for all eligible patients (1-2)
Intravenous thrombolysis (IVT) with rtPA administered within 4.5 hours of an acute ischemic stroke has been the standard
treatment. However, patients with stroke due to a large vessel occlusion respond poorly to intravenous rt-PA alone (3).
Previous clinical trials have demonstrated that mechanical thrombectomy is an effective therapy for acute ischemic stroke
compared to the use of intravenous thrombolysis IVT only (4-5).
Several randomized-controlled studies have consistently shown that patients with a large vessel occlusion in the anterior
circulation benefit from mechanical thrombectomy following IVT with rtPA (6-7). This was hypothesized that IVT may
reduce retrieved clot area and affect the number of passes required to remove clot which in turn may influence re-
vascularization outcome compared to mechanical alone.
Another meta-analysis has suggested that IVT+ mechanical thrombectomy patients had better functional outcomes, lower
mortality, higher rates of successful recanalization, and equal odds of symptomatic intracerebral hemorrhage compared
with patients treated with direct mechanical thrombectomy (8).
However, recent studies seem to conclude that MT alone may offer comparable safety and efficacy to bridging-therapy (9-
10).
So, it is still unclear if, for patients with suspected acute ischemic stroke whether rtPA versus immediate mechanical
thrombectomy should be prioritized, but the previous administration of rtPA may certainly be of help for patients living in
areas where the primary referral hospital is a local stroke center with no availability of mechanical thrombectomy option.
7.
References
1- TheAmerican Heart Association and American Stroke Association (2018) Released updated ischemic stroke guidelines that were
published in Stroke, and released during the International Stroke Conference 2018 (ISC; 24–26 January 2018. Los Angeles, USA).
2- Turc G, Bhogal P, Fischer U, et al. European stroke organization (ESO)– European Society for Minimally Invasive Neurological
Therapy (ESMINT) guidelines on mechanical thrombectomy in acute ischemic stroke endorsed by Stroke Alliance for Europe (SAFE).
Eur Stroke J. 2019; 4(1):6–12
3- Bhatia R, Hill MD, Shobha N, et al. Low rates of acute recanalization with intravenous recombinant tissue plasminogen activator
in ischemic stroke: real-world experience and a call for action. Stroke. 2010;41(10):2254–2258.
4- Berkhemer OA, Fransen PS, Beumer D, et al. A randomized trial of intra-arterial treatment for acute ischemic stroke. N Engl J
Med. 2015; 372:11–20
5- Campbell BC, Mitchell PJ, Kleinig TJ, et al. EXTENDIA investigators endovascular therapy for ischemic stroke with perfusion-
imaging selection. N Engl J Med. 2015;372:1009–1018
6- Muir KW, Ford GA, Messow CM, et al. Endovascular therapy for acute ischemic stroke: the Pragmatic Ischemic Stroke
Thrombectomy Evaluation (PISTE) randomized, controlled trial. J Neurol Neurosurg Psychiatry. 2017;88:38–44.
7- Bracard S, Ducrocq X, Mas JL, et al. Mechanical thrombectomy after intravenous alteplase versus alteplase alone after stroke
(THRACE): a randomized controlled trial. Lancet Neurol. 2016;15:1138–47.
8- Mistry EA, Mistry AM, Nakawah MO, et al. Mechanical thrombectomy outcomes with and without intravenous thrombolysis in
stroke patients: a meta-analysis. Stroke. 2017;48:2450–6.
9- Abilleira S, Ribera A, Cardona P, et al. Outcomes after direct thrombectomy or combined intravenous and endovascular
treatment are not different. Stroke. 2017;48:375–378.
10- Rai AT, Boo S, Buseman C, et al. Intravenous thrombolysis before endovascular therapy for large vessel strokes can lead to
significantly higher hospital costs without improving outcomes. J Neurointerv Surg. 2018;10:17–21.

![Mechanical thrombectomy in acute stroke [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mechanicalthrombectomyinacutestrokeautosaved-230102142009-fe15766f-thumbnail.jpg?width=640&height=640&fit=bounds)


































![dr[1]._fathi1bbbbbbbbbbbbbbbbbbbbbbb.ppt](https://cdn.slidesharecdn.com/ss_thumbnails/dr1-250926211113-fcc6607a-thumbnail.jpg?width=640&height=640&fit=bounds)































