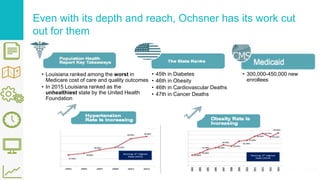
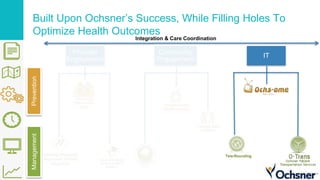
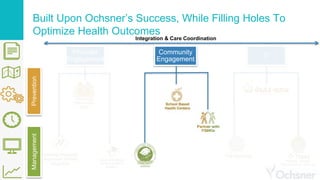
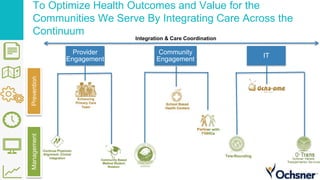
Ochsner Health is enhancing its population health strategy by focusing on access, education, and preventive care to better serve vulnerable populations in Louisiana, which has some of the worst health outcomes in the United States. The health system aims to expand community outreach and collaboration with federally qualified health centers while implementing a three-pronged strategy that includes provider engagement and care coordination. By leveraging existing resources and data analytics, Ochsner seeks to improve healthcare delivery and outcomes while reducing costs for its patients.