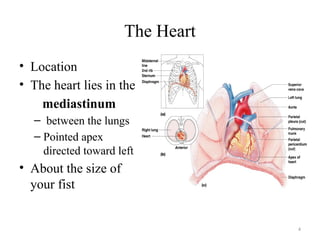
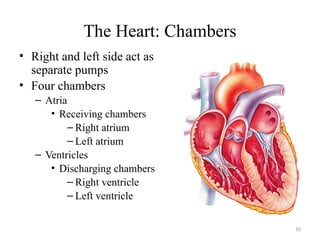
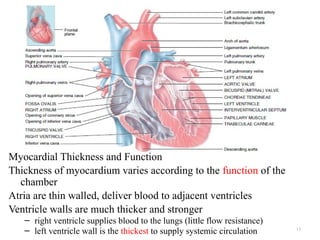
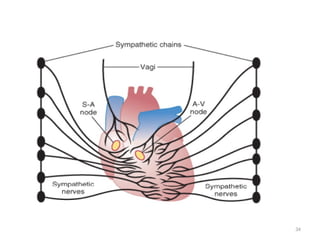
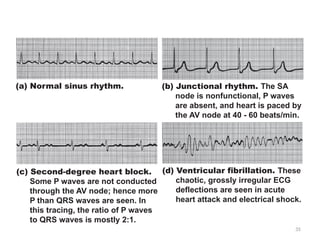
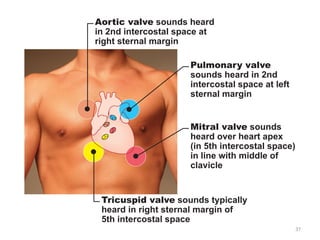
The document provides an overview of the cardiovascular system, describing its components, including the heart, blood vessels, and associated functions, such as delivering nutrients and oxygen while removing waste. It details the structure of the heart, including its layers, chambers, and valves, as well as the conduction system that regulates heartbeats and blood flow. Additionally, it discusses the cardiac cycle, heart sounds, blood pressure, and various cardiovascular health conditions.