Recommended

More Related Content
What's hot
What's hot (20)
Similar to Canada health transfer
Similar to Canada health transfer (20)
Canada health transfer
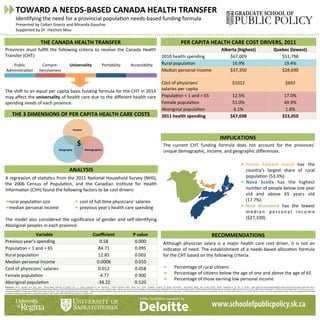
- 1. Provinces must fulfill the following criteria to receive the Canada Health Transfer (CHT): n The shi< to an equal per capita basis funding formula for the CHT in 2014 may affect the universality of health care due to the different health care spending needs of each province. PER CAPITA HEALTH CARE COST DRIVERS, 2011 Alberta (highest) Quebec (lowest) 2010 health spending $67,009 $51,798 Rural populaOon 16.9% 19.4% Median personal income $37,350 $28,690 Cost of physicians’ salaries per capita $1012 $692 PopulaOon < 1 and > 65 12.5% 17.0% Female populaOon 51.0% 49.9% Aboriginal populaOon 6.1% 1.8% 2011 health spending $67,698 $53,050 TOWARD A NEEDS-‐BASED CANADA HEALTH TRANSFER IdenOfying the need for a provincial populaOon needs-‐based funding formula Presented by Colten Goertz and Miranda Gouchie Supported by Dr. Haizhen Mou RECOMMENDATIONS THE CANADA HEALTH TRANSFER ANALYSIS A regression of staOsOcs from the 2011 NaOonal Household Survey (NHS), the 2006 Census of PopulaOon, and the Canadian InsOtute for Health InformaOon (CIHI) found the following factors to be cost drivers: rural populaOon size median personal income The model also considered the significance of gender and self-‐idenOfying Aboriginal peoples in each province. IMPLICATIONS References: Birch, Stephen and John Eyles. “Needs-‐Based Planning of Health Care: A CriOcal Appraisal of the Literature.” CHEPA Working Paper Series 91-‐5. 1991. Canadian InsOtute of Health InformaOon. “QuickStats: Public and Private Sector Health Expenditures by Use of Funds.” hip://apps.cihi.ca/mstrapp/asp/Main.aspx?Server=apmstrextprd_i&project=Quick +Stats&uid=pce_pub_en&pwd=&evt=2048001&visualizaOonMode=0&documentID=9D0E83BC4BACDADE9D4938B338C6B6D5. Dwyer, JusOn and Kathy Eager. “OpOons for reform of Commonwealth and State governance responsibiliOes for the Australian health system.” Na8onal Health and Hospitals Reform Commission. 2008. Government of Canada. “2006 Census of PopulaOon.” StaOsOcs Canada. hips://www12.statcan.gc.ca/census-‐ recensement/2006/rt-‐td/index-‐eng.cfm#tab5. Government of Canada. “2011 NaOonal Household Survey: Data tables.” StaOsOcs Canada. hip://www12.statcan.gc.ca/nhs-‐enm/2011/dp-‐pd/dt-‐td/index-‐eng.cfm. Marchildon, Gregory and Haizhen Mou. “A Needs-‐Based AllocaOon for the Canada Health Transfer. Canadian Public Policy 40, no. 3 (2014): 209-‐223. Penno, Erin, Robin Gauld and Rick Audas. “How are populaOon-‐based funding formulae for healthcare composed? A comparaOve analysis of seven models.” BMC Health Services Research 13 (2013): 470. Prince Edward Island has the country’s largest share of rural populaOon (53.3%). Nova ScoYa has the highest number of people below one year old and above 65 years old (17.7%). New Brunswick has the lowest m e d i a n p e r s o n a l i n c o m e ($27,330). THE 3 DIMENSIONS OF PER CAPITA HEALTH CARE COSTS Although physician salary is a major health care cost driver, it is not an indicator of need. The establishment of a needs-‐based allocaOon formula for the CHT based on the following criteria: Percentage of rural ciOzens Percentage of ciOzens below the age of one and above the age of 65 Percentage of those earning low personal income Public AdministraOon Compre-‐ hensiveness Universality Portability Accessibility The current CHT funding formula does not account for the provinces’ unique demographic, income, and geographic differences. Variable Coefficient P value Previous year’s spending 0.58 0.000 PopulaOon < 1 and > 65 84.71 0.095 Rural populaOon 12.85 0.002 Median personal income 0.0008 0.010 Cost of physicians’ salaries 0.012 0.058 Female populaOon -‐4.77 0.900 Aboriginal populaOon -‐34.22 0.520 Income Geography Demographics $ cost of full-‐Ome physicians’ salaries previous year’s health care spending Poster Competition sponsored by: